Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
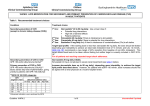
Table 1 . Percent Reduction in LDL-c with Statins Statin dose per day Atorvastatin 10 mg 20 mg 40 mg 80 mg Fluvastatin 20 mg 40 mg 80 mg 80 mg XL* Lovastatin 10 mg 20 mg 40 mg 80 mg Pravastatin 10 mg 20 mg 40 mg 80 mg* Rosuvastatin 5 mg 10 mg 20 mg 40 mg Simvastatin 10 mg 20 mg 40 mg 80 mg Range of percent LDL-c lowering from comparative clinical Trials Mean percent LDL-c lowering from manufacturers prescribing information (and from ATP-III3 if available) Number of clinical trials** 28.9%–40.2% 38.4%–46.1% 45.1%–51.3% 46.3%–54% 39% (37%) 43% 50% 60% (57%) 22 8 5 6 17%–21.8% 22%–26% 29.6%–30.6%+ -- 22% (18%) β 25% β 36% (31%)++ β 35% β 5 6 2 0 21.6%–24% 21%–29% 27.9%–33% 39%–48% 21% 27% (24%) 31% 42% (40%) α 2 8 5 2 18%–24.5% 23%–29% 25.2%–34% -- 22% 32% (24%) 34% 37% (34%) 9 11 8 0 39.1%–46% 37.1%–50.6% 45.7%–52.4% 53.6%–58.8% 45% 52% 55% 63% 6 9 3 3 26%–33.1% 18.5%–40% 34.3%–43% 43%–48.8% 30% 38% (35%) 41% 47% (46%) 17 17 7 5 *Newly-approved dose or dosage form with no head-to-head clinical trial data against another statin. **% LDL-c reduction in clinical trials included in table only if data provided for a specific dosage and not a mean dosage; total number of clinical trials will be more than the number of included trials because some trials studied more than two statins. + Given as fluvastatin 80 mg qd or 40 mg bid (does not include XL product) ++ Given as fluvastatin 40 mg bid α Given as lovastatin 40 mg bid β Median percent change © 2001-2008 by Oregon Health & Science University, Portland, Oregon 97201. All rights reserved. Table 2 . Doses of statins that result in similar percent reductions in LDL-c* Atorvastatin -10 mg 20 mg 40 mg 80 mg -- Fluvastatin 40 mg 80 mg ----- Lovastatin 20 mg 40 or 80 mg 80 mg ---- Pravastatin 20 mg 40 mg 80 mg ---- Rosuvastatin --5 or 10 mg -20 mg 40 mg Simvastatin 10 mg 20 mg 40 mg 80 mg --- *estimates based on results of head-to-head trials (Evidence Table 1) © 2001-2008 by Oregon Health & Science University, Portland, Oregon 97201. All rights reserved. Pagina 1 di 4 Key Question Level of Evidence Conclusion 1. How do statins compare in their ability to reduce LDL-c? Fair. The ideal study would be a doubleblind, intention-to-treat randomized trial in which equipotent doses of different statins were compared with regard to LDL-lowering, withdrawals, and adverse effects. No studies met these stringent criteria. a. Are there doses for each statin that produce similar percent reduction in LDL-c between statins? Fair-to-good Results of a large number of trials are generally consistent with information from the manufacturer. When statins are provided in doses that are approximately equipotent, a similar percent reduction in LDLc can be achieved b. Is there a difference in the ability of a statin to achieve National Cholesterol Education Program (NCEP) goals? Good for most comparisons (see text). For patients who require LDL-c reductions of up to 35% to meet their goal, any of the statins are effective. In patients requiring an LDL-c reduction of 35% to 50% to meet the NCEP goal, atorvastatin 20 mg or more, lovastatin 80 mg, rosuvastatin 10 mg or more, and simvastatin 20 mg or more daily are likely to meet the goal. Atorvastatin 80 mg daily and rosuvastatin 20 mg or more can reduce LDL-C by 50% or more. Based on fair-quality studies, atorvastatin 80 mg daily resulted in 5 to 6 additional percentage points of LDL reduction than simvastatin 80 mg (53%-54% vs. 47%-48%), but had significantly higher rates of some adverse events. In short-term (6 weeks) studies rosuvastatin 40 mg had greater reduction in LDL-c than atorvastatin 80 mg with similar frequency of adverse events. 2. How do statins compare in their ability to raise HDL-c? Fair-to-good When statins are provided in doses that are approximately equipotent, a similar percent increase in HDL-c can be achieved. There is conflicting evidence about simvastatin vs atorvastatin, with some studies finding no difference and others finding simvastatin superior. Some studies found greater increases in HDL-c with rosuvastatin compared with atorvastatin, while other studies found no difference. 3. How do statins compare in their ability to reduce the risk of nonfatal myocardial infarction, angina, CHD mortality, all-cause mortality, stroke or need for revascularization (coronary artery bypass graft, angioplasty or stenting)? NA There are no controlled trials comparing equivalent doses of two or more statins to reduce the risk of coronary events, stroke, or death. Pagina 2 di 4 Key Question Level of Evidence Conclusion Which statins have been shown to reduce all-cause mortality? Good. Patients who have never had CHD: pravastatin (high-risk patients), simvastatin (mixed populations) Patients with CHD: atorvastatin (post-MI), pravastatin, simvastatin. Which statins have been shown to reduce cardiovascular mortality? Good. Patients who have never had CHD: Pravastatin, simvastatin Patients with CHD: simvastatin, atorvastatin Which statins have been shown to reduce CHD events? Fair-to-good. Patients who have never had CHD: atorvastatin (high-risk patients, patients with diabetes), lovastatin (average-risk patients), pravastatin (high-risk patients), simvastatin (mixed populations) Patients with CHD: atorvastatin, simvastatin, pravastatin. Patients after PTCA: fluvastatin, pravastatin. Which statins have been shown to reduce strokes? Good. Atorvastatin, pravastatin, simvastatin Patients with diabetes Good There are good efficacy data for people with diabetes. Atorva 10 mg reduced cardiovascular events in a primary prevention trial of patients with diabetes (CARDS), and simvastatin 40 mg reduced cardiovascular events in patients with diabetes (HPS). In a subgroup analysis of the LIPS trial there was a reduction in coronary events (cardiac death, nonfatal MI, CABG, or repeat PCI) with fluvastatatin 80 mg in patients with diabetes who had undergone successful PCI. Studies that included people with diabetes had rates of adverse effects similar to other studies. 4.a. Are there differences in effectiveness of statins in different demographic groups (age, sex, race)? Good (elderly, women) Poor (African Americans, Hispanics, and other ethnic groups) The benefits of statins have been documented in women and the elderly. There are almost no data about African Americans, Hispanics, or other ethnic groups. There are no data from clinical trials comparing the efficacy of different statins in women, the elderly, or African Americans 4.b. Are there differences in safety of statins in different demographic groups (age, sex, race)? Poor There are no data from clinical trials comparing the safety of different statins in women, the elderly, or African Americans. A pharmacokinetic study of rosuvastatin conducted in the US demonstrated an approximate 2-fold elevation in median exposure in Asian subjects (having either Filipino, Chinese, Japanese, Korean, Vietnamese, or AsianIndian origin) compared with a Caucasian control group. Pagina 3 di 4 Key Question Level of Evidence Conclusion a. General population Good Although CPK elevations are common, the risk of symptomatic myopathy is low. All of the available statins (simvastatin, lovastatin, atorvastatin, fluvastatin, pravastatin, rosuvastatin), when administered alone, have been associated with infrequent myotoxic adverse effects ranging from myalgia, and myopathy to rhabdomyolysis. Two meta-analyses of clinical trials found rates of elevated transaminases (liver function tests) to be no higher among patients taking statins than among those receiving placebo. There is no evidence that elevated transaminases associated with statin use increase the risk of clinically significant liver failure. In a trial of two doses of atorvastatin, the incidence of persistent elevations in liver aminotransferase levels 2 per 1000 in patients taking atorvastatin 10 mg daily, versus 1.2 per 1000 in patients taking 80 mg daily. There is insufficient evidence to determine which statin or statins are safer with regard to muscle toxicity or elevated liver enzymes. Among high potency statins, at doses below 80 mg, rates of adverse events and withdrawals due to adverse events were similar in patients taking atorvastatin or simvastatin. Atorvastatin 80 mg had a higher rate of some adverse effects (GI disturbances and transaminase elevation) than simvastatin 80 mg daily in a trial in which the LDL lowering of atorvastatin was greater than that of simvastatin. Adverse event rates in patients using rosuvastatin 40 mg were similar to rates in patients using atorvastatin 80 mg in short-term trials. b. Special populations: Patients with diabetes Good Studies that included people with diabetes had rates of adverse effects similar to other studies. Patients with HIV and transplant patients One fair-quality observational study; one small trial (pravastatin) case reports; expert opinion; pharmacology. In theory, pravastatin, fluvastatin, and rosuvastatin have the lowest potential for interactions with drugs that are potent inhibitors of CYP 3A4. Atorvastatin, lovastatin and simvastatin have the greatest potential for clinically important interactions. Fluvastatin has a potential for interaction with drugs inhibiting CYP 2C9 (Table 12) and pravastatin has the lowest potential for drug interactions and is the safest choice in those patients receiving potent CYP inhibitors. Experts recommend starting with pravastatin and fluvastatin and using the lowest dose possible. Although there is no proof from clinical studies that these recommendations are correct, on ethical grounds low-dose pravastatin and fluvastatin probably cannot be tested in a good-quality controlled study against high doses or other statins. Drug interactions Fair The combination of any statin with fibrates, and to a lesser extent niacin, can result in a higher risk for myopathy or rhabdomyolysis. 5. Are there differences in the safety of statins? © 2001-2008 by Oregon Health & Science University, Portland, Oregon 97201. All rights reserved. Pagina 4 di 4