Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
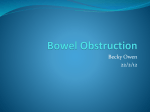
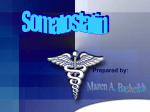
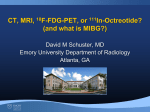
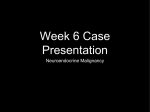
ORIGINAL E n d o c r i n e ARTICLE C a r e Oral Octreotide Absorption in Human Subjects: Comparable Pharmacokinetics to Parenteral Octreotide and Effective Growth Hormone Suppression S. Tuvia, J. Atsmon, S. L. Teichman, S. Katz, P. Salama, D. Pelled, I. Landau, I. Karmeli, M. Bidlingmaier, C. J. Strasburger, D. L. Kleinberg, S. Melmed, and R. Mamluk Chiasma (S.T., S.L.T., S.K., P.S., D.P., I.L., I.K., R.M.), Jerusalem 91450, Israel; Clinical Research Center (J.A.), Tel Aviv Sourasky Medical Center and Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv 69978, Israel; Medizinische Klinik und Poliklinik IV (M.B.), Klinikum der Universität, 80336 Munich, Germany; Division of Clinical Endocrinology (C.J.S.), Department of Medicine, Campus Mitte, Charité Universitätsmedizin Berlin, 10117 Berlin, Germany; School of Medicine (D.L.K.), New York University, New York, New York 10016; and Department of Medicine (S.M.), Cedars Sinai Medical Center, Los Angeles, California 90048 Context: Oral administration of a novel octreotide formulation enabled its absorption to the systemic circulation, exhibiting blood concentrations comparable to those observed with injected octreotide and maintaining its biological activity. Objectives: The aim of the study was to determine oral octreotide absorption and effects on pituitary GH secretion compared to sc octreotide injection. Design: Four single-dose studies were conducted in 75 healthy volunteers. Intervention: Oral doses of 3, 10, or 20 mg octreotide and a single sc injection of 100 g octreotide were administered. Main Outcome Measure: We measured the pharmacokinetic profile of orally administrated octreotide and the effect of octreotide on basal and stimulated GH secretion. Results: Both oral and sc treatments were well tolerated. Oral octreotide absorption to the circulation was apparent within 1 h after dose administration. Escalating oral octreotide doses resulted in dose-dependent increased plasma octreotide concentrations, with an observed rate of plasma decay similar to parenteral administration. Both 20 mg oral octreotide and injection of 0.1 mg sc octreotide resulted in equivalent pharmacokinetic parameters [mean peak plasma concentration, 3.77 ⫾ 0.25 vs. 3.97 ⫾ 0.19 ng/ml; mean area under the curve, 16.2 ⫾ 1.25 vs. 12.1 ⫾ 0.45 h⫻ng/ml); and median time ⱖ0.5 ng/ml, 7.67 vs. 5.88 h, respectively). A single dose of 20 mg oral octreotide resulted in basal (P ⬍ 0.05) and GHRH-stimulated (P ⬍ 0.001) mean GH levels suppressed by 49 and 80%, respectively. Conclusions: The results support an oral octreotide alternative to parenteral octreotide treatment for patients with acromegaly. (J Clin Endocrinol Metab 97: 2362–2369, 2012) ISSN Print 0021-972X ISSN Online 1945-7197 Printed in U.S.A. Copyright © 2012 by The Endocrine Society doi: 10.1210/jc.2012-1179 Received January 23, 2012. Accepted April 2, 2012. First Published Online April 26, 2012 2362 jcem.endojournals.org Abbreviations: AE, Adverse event; AUC, area under the curve; Cavg, average GH concentration; Cmax, peak plasma concentration; PD, pharmacodynamic; PK, pharmacokinetic; PPI, proton-pump inhibitor; Tmax, time to Cmax. J Clin Endocrinol Metab, July 2012, 97(7):2362–2369 J Clin Endocrinol Metab, July 2012, 97(7):2362–2369 ctreotide, a synthetic octapeptide analog of human somatostatin (1–3), is used for treatment of acromegaly and neuroendocrine tumors. Octreotide is more active than native somatostatin in inhibiting GH, insulin, glucagon, and other hormones in animals and in man (1, 2). The difference is due to an elimination half-life of 2–3 min for somatostatin in humans, compared with approximately 100 min for octreotide (4). Octreotide administration also decreases splanchnic blood flow (5, 6) and inhibits release of serotonin, gastrin, vasoactive intestinal peptide, secretin, motilin, and pancreatic polypeptide (7). Clinically, octreotide use has been limited to the parenteral route because it exhibits low and variable systemic bioavailability upon oral administration (8 –10). In chronic conditions, such as acromegaly, the burden of injectable drug regimens adversely impacts patients’ quality of life (11, 12). There have been a number of attempts to augment octreotide intestinal absorption to enable oral octreotide treatment (9, 13–16), but none have become commercially available. Most recently, a new formulation was reported (17), combining octreotide and other excipients to form an oily suspension of hydrophilic particles in a lipophilic medium allowing enhanced intestinal permeability. This preparation was shown in rats to facilitate a transient paracellular passage of octreotide across the gastrointestinal wall in the small intestines (18). Rat enteral octreotide absorption was shown to be dose-dependent, and the effects on the GH levels were comparable to the injectable form of octreotide (17). The present set of studies was designed to test this new formulation in humans and compare pharmacokinetics (PK) of a single-dose of oral and injectable O jcem.endojournals.org 2363 (sc) octreotide in healthy volunteers, to assess the safety and tolerability of the new oral octreotide formulation, and to test whether orally absorbed octreotide is functional and exerts pharmacological suppression of pituitary GH release. Subjects and Methods Subjects Seventy-five healthy volunteers were recruited in the Tel Aviv Sourasky Medical Center (Tel Aviv, Israel; n ⫽ 51) and in Celerion, Inc. (Lincoln, NE; n ⫽ 24) and screened for clinically significant conditions. Four separate studies were carried out at the two sites (Fig. 1). Criteria for inclusion in studies 1, 2, and 4 included subjects between 18 and 49 yr of age, body mass index of 19 to 30 kg/m2, and weight of at least 55 kg. In study 3, the criteria were age between 18 and 35 yr and body mass index of 19 to 25 kg/m2. Volunteers were excluded if they tested positive for drugs in a urine test, smoked (in last 6 months), were treated with another investigational drug within 3 months before screening, or consumed excess alcohol and/or prescription or over-thecounter medications, including vitamins, herbal and/or other dietary supplements 14 d before the study. All participants gave written informed consent according to the Declaration of Helsinki, Seoul and Good Clinical Practice as outlined by ICH guidelines. Experimental protocols were approved by the Institutional Review Board for the Tel Aviv Sourasky Medical Center (no. 20090885, 20100253), and as part of an IND protocol (IND 108,163) for Celerion, Inc. Study treatments Injectable octreotide (Sandostatin; Novartis, Basel, Switzerland) (19) was provided as sterile 1-ml ampoules, each containing 0.1 mg of octreotide acetate. The drug was injected sc in the FIG. 1. Trials profile. Seventy-five healthy volunteers were enrolled in four crossover open-label trials in Tel Aviv, Israel (n ⫽ 3) and Lincoln, Nebraska (n ⫽ 1). Of them, 71 volunteers underwent single 3-, 10-, and 20-mg (or 10-mg twice) oral administration or a single sc injection of 0.1 mg of octreotide acetate. 2364 Tuvia et al. Oral Octreotide for Growth Hormone Suppression deltoid area. Oral formulation (Octreolin; Chiasma, Jerusalem, Israel) consisted of 3, 10, or 20 mg unmodified octreotide acetate, in an oily suspension including polyvinyl pyrrolidone, sodium caprylate, polysorbate 80, glyceryl monocaprylate, glyceryl tricaprylate, and magnesium chloride (20). The oral preparations were administrated in enteric-coated gelatin capsules after a 10-h fast and were swallowed with 240 ml water. In study 2, participants consumed a high-fat, high-calorie meal (900 –1000 calories) immediately before the oral octreotide dosing. The composition of the tested meal was 55% energy derived from fat, 29% energy from carbohydrates, and 16% energy from protein. In study 4, a delayed-release esomeprazole capsule (40 mg Nexium; AstraZeneca Inc., Wilmington, DE) was additionally administered daily on d 2 through 7. Study design PK and pharmacodynamic (PD) data were collected to evaluate the oral octreotide formulation in healthy adult volunteers in four separate studies (Fig. 1). In study 1, octreotide PK measurements were performed in 12 males (mean age, 23 yr) using a partly randomized, dose-escalation two-way crossover design, with 7-d washout intervals. Blood octreotide levels were measured after oral administration of 3, 10, and 20 mg octreotide or injection sc of 0.1 mg octreotide. Next, the food effect was studied (study 2) in 24 volunteers (11 females and 13 males; mean age, 29 yr) using a randomized, single-dose, two-period, crossover design. Oral octreotide capsule (20 mg) was administered to 24 participants while fasting 10 h before and during dosing, or after 10-h fasting and consumption of a high-fat, high-calorie meal 0.5 h before dosing. Parenteral octreotide (0.1 mg) was subsequently administered sc. A PK/PD study (study 3) was conducted next in 24 volunteers (13 females and 11 males; mean age, 24 yr) to evaluate the PK results of a single 20 mg octreotide oral dose and its effects on GH suppression. Additionally, the duration of intestinal permeability was evaluated after oral octreotide capsule administration (data not shown in this report). The study consisted of four dosing periods and three 2-wk washout periods between doses. Five subjects discontinued before completing the study. Lastly, the effect of proton-pump inhibitor (PPI), esomeprazole, on oral octreotide absorption was assessed in 14 volunteers (seven females and seven males; mean age, 29 yr; study 4). Subjects received 20 mg oral octreotide at first, followed by 6 d of PPI administration. On d 7, a second dose of oral octreotide (20 mg) was coadministered with the PPI, and octreotide blood levels and PK were compared between d 0 and 7. One subject discontinued before completing the study. Study assessment Safety was evaluated at enrollment and after the indicated treatments by measuring vital signs, physical examination, 12lead electrocardiogram, and clinical laboratory assessments including blood biochemical and hematological parameters and urinalysis. Before dosing and/or high-fat meal consumption, subjects were required to fast for at least 10 h. An indwelling iv catheter was placed in each subject for the purpose of repeated blood sampling. A basal, i.e. pretreatment, blood sample was obtained, and a single octreotide injection (0.1 mg) or capsule (3, 10, or 20 mg) was then administered sc or orally, respectively. Repeated blood samples (1.0 ml each) were obtained at 5, 10, 20, 30, and 45 min and at 1, 1.5, 2, 3, 4, 5, 6, 8, 10, 12, and 24 h after the J Clin Endocrinol Metab, July 2012, 97(7):2362–2369 end of the sc injection and at 20 and 40 min and then at 1, 1.33, 1.66, 2, 2.33, 2.66, 3, 3.33, 4, 5, 6, 8, 12, and 24 h after oral dosing. Blood was collected into EDTA-containing tubes and centrifuged at 1000 ⫻ g for 15 min at 4 C to isolate plasma. Plasma samples were stored at ⫺80 C for later octreotide measurements. The effect of the oral octreotide treatment (20 mg) was tested on the GH levels using the GHRH/arginine test (21, 22). GHRH (Ferring Pharmaceuticals, Middlesex, UK) 1 g/kg was administered as an iv bolus 2 h after oral octreotide dosing (“time zero”), followed immediately by a 30-min infusion of L-arginine (30 g; Phebra Pty Ltd., Lane Cove, Australia) in 300 ml saline. Blood samples were drawn at 3, 2.66, 2.33, 2.0, 1.66, 1.33, 1.0, 0.66, and 0.33 h before infusion, with the infusion, and at 0.25, 0.5, 0.75, 1, 1.25, 1.5, 1.75, and 2 h after GHRH/arginine administration for serum GH and octreotide measurements. Bioanalytical assessment Octreotide plasma levels were obtained using HPLC with column-switching guard column (ACQUITY UPLC BEH C18 VanGuard); precolumn (2.1 mm ⫻ 5 mm), 1.7 m; and analytical column, (ACQUITY UPLC BEH C18, 2.1 mm ⫻ 100 mm, 1.7 m) (all from Waters Corp., Milford, MA); and mass spectrometer (MS)/MS (Sciex API 4000, Triple quadrupole; AB Sciex, Framingham, CT) detection using multiple reaction monitoring positive ion electrospray with Q1/Q3 mass transitions of 510/120 for the octreotide and 513/120 for the internal standard, [13C6Phe3]octreotide (cyclic). The isocratic elution used a mix of 80% mobile phase A (0.1% formic acid in water) and 20% of mobile phase B (0.1% formic acid in acetonitrile) from 0.0 to 4.7 min. The limit of quantization for octreotide concentration in plasma was defined as 0.025 ng/ml. The interassay coefficients of variation ranged from 3.15 to 5.71%, and intraassay coefficients of variation ranged from 0.01 to 14.6%. Serum GH concentrations were determined using an immunochemiluminometric method (IDS Immunodiagnostic Systems, Boldon, UK). This double monoclonal antibody-based sandwich assay measures only 22-kDa GH, exhibiting no cross-reactivity with other GH forms. The assay had a 0.05 ng/ml limit of detection, and linearity was established in the 0.05–100 ng/ml dynamic range (23). Data analysis Pharmacokinetics Octreotide PK parameters [peak plasma concentration (Cmax), time to Cmax (Tmax), elimination half-life, and AUC] were calculated using standard noncompartmental methods from the plasma concentration vs. time in each subject. PK calculations were performed using SAS version 9.1.3. (SAS Institute, Inc., Cary, NC). Cmax and Tmax were determined directly from the measurement results, and AUC values were determined using the linear trapezoidal rule and extrapolated to infinity using the last octreotide values measured above the detection limit. Pharmacodynamics Effects of octreotide on serum GH levels before and after GHRH induction were assessed. Cmax of GH was derived directly from the data gathered after GHRH induction (2 to 4 h). The GH AUC was calculated using the linear trapezoidal method, and the average GH concentration (Cavg) was calcu- J Clin Endocrinol Metab, July 2012, 97(7):2362–2369 jcem.endojournals.org 2365 TABLE 1. Incidence of the most common side effects encountered after single oral or sc injection of octreotide acetate to healthy subjects Oral octreotide acetate (n ⴝ 105)b Frequency of side effectsa Injection site reaction Abdominal pain Diarrhea Headache Nausea Feces discolored No. of events 0 16 8 10 7 11 Subcutaneous injection of octreotide acetate (n ⴝ 26) % 0 15 8 10 7 10 No. of events 10 3 2 2 2 1 a Events listed constitute more than 5% of documented AE. b Seventy-five healthy subjects participated in four separate studies; 34 volunteers received oral octreotide acetate more than once. lated as the arithmetic mean of the concentrations. Both parameters were calculated per treatment and over the indicated time frame in the assay, i.e. at baseline (baseline to 1 h), before (baseline to 2 h), and after GHRH induction (2 to 4 h). The basal and the GHRH-induced Cavg and AUC in the oral octreotide treated and nontreated groups were compared using a two-sided paired Student’s t test. Results were expressed as mean ⫾ SE if normally distributed or as median (range) if the data were skewed. A significance level of P ⬍ 0.05 was used for all statistical analyses. A total of 71 subjects (all completed the studies) were included in the PK, PD, and safety analysis sets (all exposed). Results Subjects Seventy-five subjects who qualified for study were included in the four studies (Fig. 1). Of these, 71 underwent 20 mg oral octreotide dosing during the studies (95%); four discontinued participation (5.3%) for non-drug-related reasons (three in study 1 and one in study 3). Of the 71 that dosed with 20 mg of oral octreotide, 65 volunteers received oral octreotide more than once. All subjects tolerated both oral and sc treatments, and no serious adverse events (AE) were documented. Incidences of the key AE encountered are presented in Table 1. In total, 60 and 21 AE were recorded in 37 of 105 (35%) and 15 of 36 (42%) healthy subjects after oral and parenteral administration of octreotide, respectively. The most common AE were injection site reaction (38%) and abdominal pain (15%) in the injectable or oral octreotide groups, respectively. In study 1, a few subjects reported light-colored stools 1 or 2 d after a single dose of Octreolin. Although this occurred only after administration of the oral preparation, it was not consistent among subjects and was transient. There was no clinical or laboratory evidence of gallbladder dysfunction, nor did subjects report associated diarrhea or change in odor, which might indicate steatorrhea. At the time the subjects made their reports, this AE had already resolved, and therefore stools were not collected % 38 12 8 8 8 4 for further analysis. We cannot explain this finding which, incidentally, was not reported in other studies being performed simultaneously. PK parameters Octreotide plasma concentrations after 3, 10, and 20 mg oral octreotide administration are shown in Fig. 2. Observed changes in plasma octreotide PK parameters were proportional to the oral dose [mean ⫾ SE values of Cmax, 0.5 ⫾ 0.1, 2.0 ⫾ 0.2, and 3.2 ⫾ 0.7 ng/ml, respectively; AUC0-t, 1.9 ⫾ 0.3, 6.5 ⫾ 0.8, and 14.8 ⫾ 4.3 h⫻ng/ ml, respectively; and AUC⬁, 2.0 ⫾ 0.3, 8.0 ⫾ 0.8, and 15.0 ⫾ 4.2 h⫻ng/ml, respectively]. Likewise, the PK parameters of a single dosing of 20 mg oral octreotide at two capsules of 10 mg or a single capsule of 20 mg were comparable (data not shown). The PK profiles were also characterized by median lag time of 0.3 h (range, 0.3–1.7 h) and comparable mean decay rates (1.9 ⫾ 0.1, 2.3 ⫾ 0.1, FIG. 2. Dose-response effect of oral octreotide acetate on plasma octreotide levels. Mean ⫾ SE of fasting plasma octreotide levels in healthy volunteers after single 3-mg (closed diamonds; n ⫽ 12), 10-mg (closed squares; n ⫽ 12), and 20-mg (closed diamonds; n ⫽ 9) oral administration of octreotide acetate. 2366 Tuvia et al. Oral Octreotide for Growth Hormone Suppression FIG. 3. Comparable plasma octreotide concentrations after oral or sc injection of octreotide acetate. Mean plasma concentrations of octreotide after a single oral administration of 20 mg octreotide acetate (closed diamonds, n ⫽ 24; closed squares, n ⫽ 12; closed circles, n ⫽ 17) and single sc injection of 0.1 mg octreotide acetate (closed squares, dotted line; n ⫽ 14) to healthy volunteers. and 2.5 ⫾ 0.2 h at 3-, 10-, and 20-mg doses, respectively). Single octreotide capsules (20 mg) or injections (0.1 mg) were also administered orally or sc, respectively, to 12–24 healthy volunteers in studies 2, 3, and 4. Profiles of plasma octreotide levels vs. time are presented in Fig. 3, and Table 2 provides the mean PK parameters after oral and parenteral octreotide dosing. After sc injection, octreotide levels increased rapidly, peaked at 0.6 h (Cmax, 3.97 ⫾ 0.19 ng/ml), and remained above 1.0 ng/ml for 3.9 h. After oral capsule administration, plasma octreotide concentrations increased more slowly than after injection, with a comparable peak at 2.7 h (Cmax, 3.77 ⫾ 0.25 ng/ml), and sustained a mean 1.0 ng/ml or greater octreotide level for 5.9 h. Plasma octreotide concentrations declined in the injectable and oral groups with a comparable mean halflife (2.25 ⫾ 0.05 and 2.38 ⫾ 0.07 h, respectively) to subtherapeutic levels (⬍0.5 ng/ml) after 6 and 8 h, respectively. J Clin Endocrinol Metab, July 2012, 97(7):2362–2369 Octreotide uptake after an oral administration of 20 mg octreotide before and after food intake was investigated in study 2. Lower plasma octreotide levels were measured and calculated for all PK parameters (Cmax, 0.42 ⫾ 0.12 and 4.1 ⫾ 0.46 ng/ml, respectively; AUC0-t, 1.4 ⫾ 0.2 and 16.8 ⫾ 2.0 h⫻ng/ml, respectively; and AUC⬁, 1.6 ⫾ 0.2 and 17.0 ⫾ 1.6 h⫻ng/ml, respectively) in volunteers who received a high-fat and high-calorie meal before an oral octreotide intake, compared with the fasted group. Consistently, reduced (90%) bioavailability was observed in the fed group. In addition, pretreatment for 5 d with esomeprazole had a more variable effect on oral octreotide absorption (Cmax, 4.8 ⫾ 0.7 and 2.5 ⫾ 0.3 ng/ml, respectively; AUC0-t, 20.0 ⫾ 4.8 and 10.1 ⫾ 1.2 h⫻ng/ml, respectively; and AUC⬁, 4.9 ⫾ 0.7 and 10.1 ⫾ 1.2 h⫻ng/ ml, respectively) with a mean approximately 40% decrease (range, ⫺85% to ⫹115%) in octreotide bioavailability, compared with the control group. Effect of oral octreotide Response of GH to GHRH-arginine stimulation with or without oral octreotide treatment was evaluated in 16 healthy volunteers in study 3. Mean GH concentrations measured before oral octreotide administration, as well as GH levels before and after GHRH induction are shown in Fig. 4. Normal pulsatile GH secretion in healthy adults is known to be fairly low (24). Indeed, baseline GH blood concentrations were variable, and overall levels were negligible (approximately 1–3 ng/ml). However, low basal GH secretion before GHRH-arginine iv injection was significantly suppressed (P ⬍ 0.05) by oral octreotide treatment (Fig. 4B and Table 3). Peak GH elicited after GHRHarginine stimulation (⬃50 ng/ml) was strongly suppressed (⬃10 ng/ml; Table 3) by prior oral octreotide dosing (20 mg). Similarly, strong inhibition (80%) was shown (P ⬍ 0.001) for the AUC and Cavg parameters of serum GH in this group (Table 3). TABLE 2. Plasma octreotide levels after single oral administration or sc octreotide acetate injection to healthy volunteers Parametera Cmax (ng/ml) Tmax (h) AUC0-t (h⫻ng/ml) AUC⬁ (h⫻ng/ml) Half-life (h) Time lag (h) Time ⱖ0.5 ng/ml (h) Time ⱖ1 ng/ml (h) Oral octreotide acetate (20 mg) 3.77 ⫾ 0.25 (71) 2.67 (71) 关0.330 – 6.04兴 16.2 ⫾ 1.25 (71) 19.0 ⫾ 1.4 (71) 2.38 ⫾ 0.07 (71) 0.33 (31) 关0.33–1.67兴 7.67 (70) 关0.67–23.7兴 6.00 (66) 关0.33–11.7兴 Subcutaneous injection of octreotide acetate (0.1 mg) 3.97 ⫾ 0.19 (26) 0.64 (26) 关0.167– 4.00兴 12.1 ⫾ 0.45 (26) 12.4 ⫾ 0.47 (26) 2.25 ⫾ 0.05 (26) b 5.88 (26) 关3.92–7.92兴 3.92 (26) 关2.67– 4.92兴 Values are expressed as arithmetic mean ⫾ SE (number), except for Tmax, Time lag, and Time ⱖ0.5 or 1 ng/ml, which are expressed as median (number) 关range兴. a b Not applicable to the sc route of administration. J Clin Endocrinol Metab, July 2012, 97(7):2362–2369 jcem.endojournals.org FIG. 4. Oral administration of octreotide acetate suppresses the basal GH levels and secretory response to GHRH stimulation. A, Plasma GH and octreotide (closed triangles) concentrations (mean ⫾ SE; n ⫽ 16) before and after GHRH/arginine administration, with (closed squares) and without (closed circles) oral octreotide acetate treatment (20 mg). B, Inhibition of endogenous GH levels by oral octreotide acetate was also noted within the first 2 h of dosing (arrow), before GHRH stimulation. Discussion Systemic exposure of orally administrated octreotide after (20 mg) was similar to that of sc injection (0.1 mg) of this same peptide in healthy volunteers. Similarly, a comparable safety profile was shown for both octreotide formulations, except for injection-related discomfort in the sc injections. Oral octreotide absorption from enteric-coated capsules resulted in a dose-dependent increase in systemic exposure. Finally, basal levels of GH and the GHRH-stim- TABLE 3. 2367 ulation of GH secretion were significantly suppressed by a single oral octreotide dose. Both parenteral and oral octreotide formulations were well tolerated by the participants. Octreotide has been clinically used for the treatment of acromegaly for over two decades (25). Commercially available octreotide products include a refrigerated sterile octreotide solution for sc daily injection and a 1-month sustained-release octreotide depot formulated in poly-lactic-co-glycolic acid for im injection. These formulations have a well-established safety profile in which the drug-related AE include mostly mild-to-moderate and transient injection-site reactions, gastrointestinal disturbances, and occasional hyperglycemia (26). Moreover, parenteral octreotide administration was associated with pain and discomfort during daily/monthly injection. The oral preparation tested here was shown to exhibit a comparable safety profile to injectable octreotide during a 3-month daily administration in monkeys (17) and after single dosing in the present study in healthy volunteers. In the current study, both treatment groups exhibited 8 –15% incidences of gastrointestinal-related discomfort and headaches, and approximately 40% of volunteers who received the sc octreotide injection reported irritation at the injection site, consistent with previously reported AE of the injectable drug (12, 26). The oral octreotide formulation may therefore be considered as an easy, nonpainful, and comparably safe formulation compared with the parenteral drug. PK exposure observed in this study with single 3, 10, and 20 mg oral octreotide administrations were dose proportional, and the 20-mg dose was comparable to a 0.1-mg sc injection. The chronic requirement for octreotide treatment in acromegaly patients justifies the development of oral alternatives. Early reports (8, 10, 27) suggested enteral absorption of octreotide in aqueous solution; however, the measured bioavailability was low with a marked interindividual variability. Additional attempts to increase intestinal permeability of this octapeptide by employing bile acids in rats and humans (9), poly- Inhibition of basal and GHRH-stimulated GH release by oral octreotide acetate Oral octreotide acetate (20 mg) ⴚ a Parameter AUC (h⫻ng/ml) Cavg (ng/ml) a b Basal GH 2.4 ⫾ 0.7c 1.3 ⫾ 0.4 ⴙ GHRH 64.1 ⫾ 6.6 56.1 ⫾ 6.0 Basal GH 0.8 ⫾ 0.3* 0.5 ⫾ 0.2* % GH inhibition GHRH 11.5 ⫾ 3.2** 12.2 ⫾ 3.6** Basal GH 49 ⫾ 16 44 ⫾ 17.5 GHRH 80 ⫾ 4.5 80 ⫾ 4.8 Predosing GH levels of AUC (h⫻ng/ml) and Cavg (ng/ml) were 1.9 ⫾ 0.6 and 1.1 ⫾ 1.4, respectively. b Postdosing GH levels for up to 2 h, at which time the GHRH stimuli were induced (see text for further details). c Values are expressed as mean ⫾ SE (n ⫽ 16). * P ⬍ 0.05; and ** P ⬍ 0.001 were obtained by two-tailed paired Student t test comparison between the oral octreotide treated and nontreated groups. 2368 Tuvia et al. Oral Octreotide for Growth Hormone Suppression (alkyl cyanoacrylate) nanocapsules in estrogen-treated rats (28), N-trimethyl chitosan chloride in rats and pigs (15, 16), superporous hydrogel polymers in pigs (13), and alkyl-saccharides in mice (29) reported encouraging results. Notwithstanding, to the best of our knowledge, none of these formulations has been developed further. An oily suspension formulation increased rat intestinal permeability and enabled octreotide enteral absorption (17). In the current study, plasma octreotide levels increased proportionally with the oral dose in terms of Cmax and AUC. The oral encapsulated formulation resulted in peak plasma octreotide 2 h later in comparison with approximately 0.6 h for the injectable drug; nevertheless, in the clinical context of the sustained endocrine suppression, such delay is not expected to have clinical significance. Five hours after a single dosing of oral or injectable octreotide peaked, plasma octreotide levels remained within therapeutic concentrations (⬎0.5 ng/ml). In addition, plasma octreotide half-life was comparable between treatments, with an average of 2.5 h measured in both groups. To inform optimal conditions for oral octreotide dosing, the effects of food and PPI on the PK profile of oral octreotide were tested. Food had a pronounced effect on absorption of oral octreotide, inasmuch as there was an almost 90% reduction in plasma concentrations. A more moderate effect (40%) was associated with PPI administration before oral octreotide dosing. Full meal and PPI may reduce octreotide absorption from Octreolin due its effect on raising gastric pH and emptying (30, 31), causing dissolution of the pH-dependent enteric-coated Octreolin capsule in the stomach, rather than in the small intestine where octreotide absorption occurs. Additionally, the presence of large quantities of food may obstruct intestinal wall contact needed for effective octreotide absorption from Octreolin. Suppression of GH secretion by oral octreotide dosing was demonstrated before and after GHRH/arginine infusion in the current study. Somatostatin analogs, such as octreotide, bind to pituitary somatostatin receptors 2, 5, and 3 and markedly reduce GH secretion for several hours (1). Octreotide infusion (0.5 mg) to healthy volunteers suppressed GH concentrations to below 0.25 ng/ml (7). Similar inhibitory effect on GH concentrations for injectable octreotide has also been documented in acromegaly patients (32), associated with a plasma octreotide concentration of approximately 1 ng/ml. In the present study, plasma concentrations of octreotide 2 h after oral dosing of 20 mg achieved mean concentrations of approximately 1.75 ng/ml, and mean GH levels in these healthy participants were indeed less than 0.25 ng/ml (Fig. 4B). Conversely, in the nontreated group, serum GH concentrations were approximately 2.75 ng/ml at this time-point. J Clin Endocrinol Metab, July 2012, 97(7):2362–2369 Moreover, 80% of GH secretion induced by GHRH was suppressed in the octreotide-treated arm (Fig. 4A). These results indicate that oral octreotide exhibits a GH-inhibitory action similar to the parenteral drug form in healthy volunteers. In conclusion, we have shown that oral delivery of octreotide is feasible, using a unique formulation based on an oily suspension. This oral octreotide preparation results in comparable octreotide PK characteristics to sc injection, achieves levels known to be therapeutic, and exerts a notable suppression of basal as well as GHRH-induced GH secretion. A major drawback of current treatments is the need for frequent sc or im injections. The oral formulation tested here is potentially useful for chronic octreotide treatment of patients with acromegaly or neuroendocrine tumors. Acknowledgments Address all correspondence and requests for reprints to: Dr. Roni Mamluk, Ph.D., COO, Chiasma, 10 Hartom Street, Jerusalem 45182, Israel. E-mail: [email protected]. Disclosure Summary: S.T., S.L.T., S.K., P.S., D.P., I.L., I.K., and R.M. are Chiasma employees. References 1. Bauer W, Briner U, Doepfner W, Haller R, Huguenin R, Marbach P, Petcher TJ, Pless 1982 SMS 201–995: a very potent and selective octapeptide analogue of somatostatin with prolonged action. Life Sci 31:1133–1140 2. Melmed S 2009 Acromegaly pathogenesis and treatment. J Clin Invest 119:3189 –3202 3. Lamberts SW, van der Lely AJ, de Herder WW, Hofland LJ 1996 Octreotide. N Engl J Med 334:246 –254 4. Shimon I, Yan X, Taylor JE, Weiss MH, Culler MD, Melmed S 1997 Somatostatin receptor (SSTR) subtype-selective analogues differentially suppress in vitro growth hormone and prolactin in human pituitary adenomas. Novel potential therapy for functional pituitary tumors. J Clin Invest 100:2386 –2392 5. Spahr L, Giostra E, Frossard JL, Morard I, Mentha G, Hadengue A 2007 A 3-month course of long-acting repeatable octreotide (sandostatin LAR) improves portal hypertension in patients with cirrhosis: a randomized controlled study. Am J Gastroenterol 102: 1397–1405 6. Sonnenberg GE, Keller U, Perruchoud A, Burckhardt D, Gyr K 1981 Effect of somatostatin on splanchnic hemodynamics in patients with cirrhosis of the liver and in normal subjects. Gastroenterology 80: 526 –532 7. Chanson P, Timsit J, Harris AG 1993 Clinical pharmacokinetics of octreotide. Therapeutic applications in patients with pituitary tumours. Clin Pharmacokinet 25:375–391 8. Fricker G, Bruns C, Munzer J, Briner U, Albert R, Kissel T, Vonderscher J 1991 Intestinal absorption of the octapeptide SMS 201–995 visualized by fluorescence derivatization. Gastroenterology 100: 1544 –1552 9. Fricker G, Fahr A, Beglinger C, Kissel T, Reiter G, Drewe J 1996 Permeation enhancement of octreotide by specific bile salts in rats J Clin Endocrinol Metab, July 2012, 97(7):2362–2369 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. and human subjects: in vitro, in vivo correlations. Br J Pharmacol 117:217–223 Fuessl HS, Domin J, Bloom SR 1987 Oral absorption of the somatostatin analogue SMS 201–995: theoretical and practical implications. Clin Sci (Lond) 72:255–257 Ben-Shlomo A, Sheppard MC, Stephens JM, Pulgar S, Melmed S 2011 Clinical, quality of life, and economic value of acromegaly disease control. Pituitary 14:284 –294 Newman CB, Melmed S, Snyder PJ, Young WF, Boyajy LD, Levy R, Stewart WN, Klibanski A, Molitch ME, Gagel RF 1995 Safety and efficacy of long-term octreotide therapy of acromegaly: results of a multicenter trial in 103 patients—a clinical research center study. J Clin Endocrinol Metab 80:2768 –2775 Dorkoosh FA, Verhoef JC, Verheijden JH, Rafiee-Tehrani M, Borchard G, Junginger HE 2002 Peroral absorption of octreotide in pigs formulated in delivery systems on the basis of superporous hydrogel polymers. Pharm Res 19:1532–1536 Drewe J, Fricker G, Vonderscher J, Beglinger C 1993 Enteral absorption of octreotide: absorption enhancement by polyoxyethylene-24-cholesterol ether. Br J Pharmacol 108:298 –303 Thanou M, Verhoef JC, Marbach P, Junginger HE 2000 Intestinal absorption of octreotide: N-trimethyl chitosan chloride (TMC) ameliorates the permeability and absorption properties of the somatostatin analogue in vitro and in vivo. J Pharm Sci 89:951–957 Thanou M, Verhoef JC, Verheijden JH, Junginger HE 2001 Intestinal absorption of octreotide using trimethyl chitosan chloride: studies in pigs. Pharm Res 18:823– 828 Tuvia S, Salama P, Weinstein I, Marom K, Neumark E, Arama ML, Mishli N, Levy S, Lapidot T, Kadoshi R, Katz S, Judelman A, Mamluk R 2010 Octreolin a safe oral alternative for parenteral octreotide treatment. Growth Horm IGF Res 20(Suppl 1):S35–S36 Cano-Cebrián MJ, Zornoza T, Granero L, Polache A 2005 Intestinal absorption enhancement via the paracellular route by fatty acids, chitosans and others: a target for drug delivery. Curr Drug Deliv 2:9 –22 Prescribing information 2010 Sandostatin injection. East Hanover, NJ; Novartis Pharmaceuticals Corporation Weinstein I, Tzabari M, Salama P, Mamluk R, Marom K 2010 Pharmaceutical compositions and related methods of delivery. PCT International Patent Application WO 2010/ 032140:122 Growth Hormone Research Society 2000 Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH Research jcem.endojournals.org 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 2369 Society. GH Research Society. J Clin Endocrinol Metab 85:3990 – 3993 Ho KK 2007 Consensus guidelines for the diagnosis and treatment of adults with GH deficiency II: a statement of the GH Research Society in association with the European Society for Pediatric Endocrinology, Lawson Wilkins Society, European Society of Endocrinology, Japan Endocrine Society, and Endocrine Society of Australia. Eur J Endocrinol 157:695–700 Müller A, Scholz M, Blankenstein O, Binder G, Pfäffle R, Körner A, Kiess W, Heider A, Bidlingmaier M, Thiery J, Kratzsch J 2011 Harmonization of growth hormone measurements with different immunoassays by data adjustment. Clin Chem Lab Med 49:1135– 1142 Rudman D, Kutner MH, Rogers CM, Lubin MF, Fleming GA, Bain RP 1981 Impaired growth hormone secretion in the adult population: relation to age and adiposity. J Clin Invest 67:1361–1369 Melmed S, Colao A, Barkan A, Molitch M, Grossman AB, Kleinberg D, Clemmons D, Chanson P, Laws E, Schlechte J, Vance ML, Ho K, Giustina A 2009 Guidelines for acromegaly management: an update. J Clin Endocrinol Metab 94:1509 –1517 Feelders RA, Hofland LJ, van Aken MO, Neggers SJ, Lamberts SW, de Herder WW, van der Lely AJ 2009 Medical therapy of acromegaly: efficacy and safety of somatostatin analogues. Drugs 69:2207– 2226 Köhler E, Duberow-Drewe M, Drewe J, Ribes G, Loubatiéres-Mariani MM, Mazer N, Gyr K, Beglinger C 1987 Absorption of an aqueous solution of a new synthetic somatostatin analogue administered to man by gavage. Eur J Clin Pharmacol 33:167–171 Damgé C, Vonderscher J, Marbach P, Pinget M 1997 Poly(alkyl cyanoacrylate) nanocapsules as a delivery system in the rat for octreotide, a long-acting somatostatin analogue. J Pharm Pharmacol 49:949 –954 Maggio ET, Grasso P 2011 Oral delivery of octreotide acetate in Intravail improves uptake, half-life, and bioavailability over subcutaneous administration in male Swiss Webster mice. Regul Pept 167: 233–238 Aoyagi N, Ogata H, Kaniwa N, Uchiyama M, Yasuda Y, Tanioka Y 1992 Gastric emptying of tablets and granules in humans, dogs, pigs, and stomach-emptying-controlled rabbits. J Pharm Sci 81: 1170 –1174 Lennernäs H 2007 Modeling gastrointestinal drug absorption requires more in vivo biopharmaceutical data: experience from in vivo dissolution and permeability studies in humans. Curr Drug Metab 8:645– 657 Sherlock M, Woods C, Sheppard MC 2011 Medical therapy in acromegaly. Nat Rev Endocrinol 7:291–300