Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
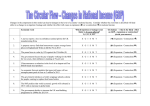
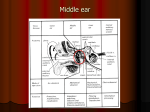
The Laryngoscope C 2012 The American Laryngological, V Rhinological and Otological Society, Inc. TRIOLOGICAL SOCIETY CANDIDATE THESIS Effects of Tensor Tympani Muscle Contraction on the Middle Ear and Markers of a Contracted Muscle Manohar Bance, MB, MSc; Fawaz M. Makki, MD; Philip Garland, PhD; Wael A. Alian, MD, PhD; Rene G. van Wijhe, MEng; Julian Savage, MBBS, FRCS Objectives/Hypothesis: Many otologic disorders have been attributed to dysfunction of the tensor tympani muscle, including tinnitus, otalgia, Meniere’s disease and sensorineural hearing loss. The objective of this study was to determine adequate stimuli for tensor tympani contraction in humans and determine markers of the hypercontracted state that could be used to detect this process in otologic disease. Study Design: Multiple types of studies. Methods: Studies included 1) measuring middle ear impedance changes in response to orbital puffs of air, facial stroking, and self-vocalization; 2) measuring changes in stapes and eardrum vibrations and middle ear acoustic impedance in response to force loading of the tensor tympani in fresh human cadaveric temporal bones; 3) measuring changes in acoustic impedance in two subjects who could voluntarily contract their tensor tympani, and performing an audiogram with the muscle contracted in one of these subjects; and 4) developing a lumped parameter computer model of the middle ear while simulating various levels of tensor tympani contraction. Results: Orbital jets of air are the most effective stimuli for eliciting tensor tympani contraction. As markers for tensor tympani contraction, all investigations indicate that tensor tympani hypercontraction should result in a low-frequency hearing loss, predominantly conductive, with a decrease in middle ear compliance. Conclusions: These markers should be searched for in otologic pathology states where the tensor tympani is suspected of being hypercontracted. Key Words: Tensor tympani, middle ear muscles, laser Doppler vibrometry, tensor tympani syndrome. Laryngoscope, 123:1021–1027, 2013 INTRODUCTION The middle ear muscles (MEM) have a long history of being implicated in many inner ear otologic disorders such as tinnitus, otalgia, Meniere’s disease, and sensorineural hearing loss (e.g., Weber1). More recently, spasm of the tensor tympani (TT) has been implicated in a range of conditions including tinnitus,2 otologic symptoms in myofascial pain-dysfunction syndrome,3 and Meniere’s disease, for which sectioning of the TT has been a sugFrom the Division of Otolaryngology, Department of Surgery (M.B., School of Biomedical Engineering (P.G.), and Ear and Auditory Sciences Laboratory (R.G.V.W.), Dalhousie University, Halifax, Nova Scotia, Canada; Department of Otolaryngology and Head and Neck Surgery (W.A.A.), Sahlgrenska University Hospital, Goteborg University, Goteborg, Sweden; and Division of Otolaryngology (J.S.), Hôtel-Dieu, University de Sherbrooke, Sherbrooke, Quebec, Canada. Editor’s Note: This Manuscript was accepted for publication August 9, 2012. This work was performed entirely at the Ear and Auditory Research Laboratory, Division of Otolaryngology, Department of Surgery, Dalhousie University, Halifax, NS, Canada. Part of this work was funded by grants from Dalhousie University Faculty of Medicine, Nova Scotia Health Research Foundation. The authors have no other funding, financial relationships, or conflicts of interest to disclose. Send correspondence to Manohar Bance, MB, Professor, Division of Otolaryngology, Department of Surgery, Dalhousie University, 3184 Dickson Building, VGH Site, QEII HSC, 1278 Tower Road, Halifax, NS, Canada B3H 2Y9. E-mail: [email protected] F.M.M.), DOI: 10.1002/lary.23711 Laryngoscope 123: April 2013 gested treatment.4 Klockhoff5 also described a tensor tympani syndrome characterized by fluctuation in the middle ear impedance and complaints of fullness, tinnitus, and dysacusis, and highly related to tension headache and vertigo. It has also been speculated that the TT medializes the stapes into the oval window, resulting in changes in inner ear perilymphatic pressures,6 which in turn may lead to various inner ear disorders. Although clonic (dynamic) contractions of the TT might be detected easily, tonic (fixed) contractions are not, because of the large normal ranges in the tests that could detect contractions (e.g., middle ear compliance). Today, the role of the TT in physiology and otologic disease is largely speculative. Unlike the stapedius, the TT is not normally activated by sound.7 After a flurry of scientific activity in the late 19th and early 20th century, the TT has been almost ignored in recent decades (see Wever and Lawrence8 for an excellent review). Reflex contraction of the TT muscle has been reported to be elicited by tactile stimulation of facial areas,7 electrical stimulation of the tongue,9 a puff of air against the orbit,10,11 swallowing,12 and during activation of some muscular groups of the face, neck, and phonation.13 The TT is most commonly reported to contract as part of the startle reaction.10 Reports implicating the MEM as the cause of otologic pathology tend to focus on the TT muscle, as does this work, but it should be recognized that contraction of the TT Bance et al.: Markers of Tensor Tympani Muscle Contraction 1021 Fig. 1. Modified mechanical lumped parameter model for human ear including the tensor tympani. cannot be directly measured or reliably distinguished from that of the stapedius with most tests, and they may well co-contract in many pathologic situations. As such, several lines of investigations were used in this report because none can directly measure TT contraction. MATERIALS AND METHODS Experiments were approved by our institutional ethics boards. This work is divided into several sections. Stimuli Eliciting TT Contraction in Live Subjects Twenty subjects with self-reported normal hearing and tympanograms were tested. Middle ear compliance was tested with a 226-Hz tone using a GSI TympStar (Grason-Stadler, Eden Prairie, MN) middle ear analyzer. Impedance changes were measured for the following stimuli: 1) stroking the face with a fine brush for 5 seconds, 2) mentally counting from 1 to 10 (true vocalization would cause sound radiation into the ear), and 3) delivering four puffs of air at random intervals from a rubber bulb to the closed ipsilateral eye or to the contralateral eye. The conditions and left and right ears were randomized in presentation. Temporal Bone Data Middle ear laser Doppler vibrometry measurements. Five temporal bones were harvested from cadaveric donors within 48 hours of death. Cortical mastoidectomy and posterior tympanotomy were performed. This preparation has been described for other experiments.14 Vibrations of the tympanic membrane (TM) and stapes were measured using either a single-point laser Doppler vibrometer (LDV) (OFV-302 sensor head, OFV-3000 vibrometer controller), or during later experiments a scanning laser Doppler vibrometer (PSV-I-400 scanhead, OFV-505 laser head, OFV-5000 vibrometer controller) by Polytec PI (Tustin, CA). Three bones were tested with the single point and two with the scanning laser. To simulate TT contraction, a 5-0 nylon suture was looped around the TT and directed posteriorly, and connected to a pulley system to provide force loading. In-line loading directly in the axis of the TT would require drilling into the cochlea. Single-point LDV measurements were performed on the stapes footplate center and on the umbo in three temporal bones corresponding to pulley masses of 0, 20, and 60 g. Measurements with the scanning LDV were performed on the whole TM and stapes footplate, with masses of 0, 26, 52, 76, and 100 g (and 13 g for the last bone). Not all measurements could be completed on all bones because of various noise and preparation artifacts. Therefore, one of the two bones used for scanning LDV only has measurements on the umbo. Two further bones were prepared similarly, and a tympanometer was used to measure the impedance change for a force of 0.5 N (equivalent to 50-g mass) applied to the TT tendon. Laryngoscope 123: April 2013 1022 Live Subject Data Several subjects were screened who could voluntarily move their TMs, but most could not hold contractions for more than few seconds. We hypothesized that eardrum movements large enough to be macroscopically visible could only come from TT contraction, although the stapedius may co-contract. Only two participants, a male aged 45 years and a female aged 37 years, could hold contractions long enough for us to measure tympanometry, and only one long enough to perform an audiogram. Acoustic impedance using a tympanometer was also measured using a standard 226-Hz probe tone. Only the right ear is reported, as results were symmetrical. Computer Models A lumped parameter computer model was created based on the model by Feng and Gan.15 The nonlinear mechanical properties of the TT described by Cheng and Gan16 were incorporated into this model. Details of this model can be found in Garland et al.17 Essentially, the nonlinear effect of this muscle is incorporated into the mathematical model by choosing a given static load value (and corresponding displacement) on the TT and taking the effective stiffness (KTT) as the slope of the curve at this load point. The effect of TT contraction is implemented by including a linear spring attached to the malleus. Figure 1 shows the slightly modified schematic representation of the model presented by Feng and Gan15 used for this study. The values of the masses were taken from previously published works and some ad hoc assumptions.17 Wideband reflectance measurements were also made in several TT conditions, but the results were complex, and due to article size limitations will be discussed in a separate publication. RESULTS Eliciting TT Contraction in Normal Subjects A measurable impedance change associated with stroking the side of the subject’s face or having the subject mentally vocalize counting 1 to 10 was not found in any of subjects tested. Results for orbital jets of air over the closed eye are shown in Table I, as are the average compliance changes. In general, positive changes (increase in impedance, decrease in compliance) were more than twice as common as negative (decrease in impedance, increase in compliance) changes. Only one subject had no change in impedance to either ipsilateral or contralateral orbital jets. Temporal bone LDV measurements. Figure 2A and 2B show results of the single LDV measurements on the vibrations of the umbo and stapes footplate, respectively, averaged over three temporal bones. With increased traction on the TT, the vibration responses in the lower frequencies are attenuated; at higher frequencies the responses remain relatively stable. Bance et al.: Markers of Tensor Tympani Muscle Contraction TABLE I. Change in Impedance in the Middle Ear Associated With a Puff of Air Directed Toward the Closed Ipsilateral and Contralateral Eyes in 20 Subjects With Normal Hearing. Stimulus Response Type No. of Subjects Average Amplitude (mL) Standard Deviation (mL) Positive 12 (60%) 0.073 0.044 Negative 5 (25%) 0.030 0.046 None 3 (15%) — — Ipsilateral Contralateral Positive 13 (65%) 0.062 0.046 Negative None 6 (30%) 1 (5%) 0.033 — 0.011 — the stapes footplate in one temporal bone. Scanning LDV measurements average across the entire measured surface over many points, and so are less affected by spatial vibration modal nulls and peaks at a single point. A clear reduction of responses in the lower frequencies can be seen in both figures. In Figure 3B, there appears to be an improvement in footplate vibrations in the higher frequencies with increasing force on the TT. Tympanometry. In both bones tested, both the tympanogram (Fig. 4A) and reflex decay (Fig. 4B) showed a drop in static peak compliance with TT contraction. The position of peak pressure of the tympanogram showed no major shift in either bone. Results were very similar to those seen in the live human data (Figs. 5 and 6). A positive amplitude indicates an increase in impedance (decrease in compliance), similar to a normal stapedial reflex compliance change, and a negative amplitude indicates a decrease in impedance (increase in compliance). Live Subject Measurements Figure 3A shows the average response of all measurement points on the TM as measured with the scanning LDV in two temporal bones; Figure 3B shows the averaged response of all the measurement points on Subject 1 could hold his contraction long enough to perform a contracted MEM audiogram, one frequency at a time. Results in Figure 5A show a conductive hearing loss with an air-bone gap of 30 and 20 dB at frequencies of 250 and 500 Hz, respectively, on TT contraction. Fig. 2. Vibration amplitudes measured using single-point laser Doppler vibrometer. (A) Tympanic membrane (umbo), and (B) center of stapes footplate at baseline (blue) and with tensor tympani traction of 20 g (green) and 60 g (red). Shown are averages for three temporal bones. Y-axis is log10 velocity/pressure, and on this log scale the change in the stapes velocity is larger than that of the umbo velocity. Fig. 3. Scanning laser Doppler vibration velocity measurements on the tympanic membrane (TM), averaged for two bones (A) and on the footplate for one bone (B). Laryngoscope 123: April 2013 Bance et al.: Markers of Tensor Tympani Muscle Contraction 1023 Fig. 4. (A) Temporal bones 1 (left) and 2 (right). Tympanogram before and after force applied to the tensor tympani (TT). Tympanograms before and after TT force applied. Black is baseline, and red is after TT force applied. Temporal bone 1 is on the left, and temporal bone 2 is on the right. Compliance changes from 0.6 to 0.3 mL in bone 1, and from 1 to 0.6 mL in bone 2. (B) Reflex decay measurements before and after force applied to TT. Reflex decay recordings after force applied to the TT (arrows). Temporal bones 1 (left) and 2 (right). [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.] Interestingly, there was a small but repeatable drop in the bone curve at 250 Hz as well. The tympanogram (Fig. 5B for subject 1 and Fig. 6A for subject 2) and reflex decay (Fig. 5C for subject 1 and Fig. 6B for subject 2) showed a drop in compliance with MEM contraction (increase in impedance). The tympanometric peak pressure did not change with TT contraction (i.e., there does not seem to be any associated change in middle ear pressure). This would also be evidence against these changes being due to pumping of the middle ear by the eustachian tube. Computer Modeling Computer simulations predicted results qualitatively similar to temporal bones and live subject results. The simulated admittance (i.e., reciprocal of impedance) results for the TM and stapes footplate during various Fig. 5. Subject 1. Tests before and after tensor tympani (TT) contraction. (A) Effect on audiogram of TT contraction in subject 1. Each frequency was separately tested before and after contraction. (B) Tympanogram before and after voluntary middle ear muscle (MEM) contraction. Compliance changes from 1 mL before MEM contraction to 0.5 mL after MEM contraction. (C) Reflex decay during voluntary contractions of MEM (arrows). [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.] Laryngoscope 123: April 2013 1024 Bance et al.: Markers of Tensor Tympani Muscle Contraction Fig. 6. Subject 2. (A) Tympanogram before and after voluntary tensor tympani (TT) contraction. (B) Reflect decay during TT contractions. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.] levels of TT contraction can be seen in Fig. 7A and 7B, respectively. The amount of TT contraction is given as a fraction of the maximum change of length of the TT. The frequency at which the peak admittance occurs increases with larger TT contractions. Somewhat surprising is the drastic decrease in peak admittance magnitude experienced by the stapes footplate with TT contraction compared to the slight increase in peak admittance magnitude of the TM. do not have any change in eardrum stiffness and usually, in clinical practice, show no static compliance changes from normal. On the eliciting factors for TT contraction, overall, 95% of the subjects had an impedance change in response to the orbital jets of air (65% an increase, 30% a decrease). These results are similar to other published studies with orbital air jets. Mulder et al.18 found 97% of the control subjects had an impedance change in response to the startle reaction, 57% had an increase in impedance, 23% had a decrease in impedance (so-called reversed response), and in 17% the response was not clearly an increase or decrease in impedance. It is unclear why this startle reaction causes an increase in impedance in some subjects and a decrease in impedance in others. Mulder et al.18 postulate that the decrease in the impedance is caused by the TT, and the increase in impedance is dominated by contraction the stapedius. Our results in temporal bones do not support this theory (Fig. 4), as TT contraction causes an increase in impedance. In the past, other authors have also postulated that a reversed ipsilateral reflex (i.e., decrease in impedance) in response to acoustic stimulation is caused by the TT (e.g., Ochi et al.19), but this is unlikely because such a reversed reflex has been observed by us and others,20 even in cadaveric temporal bones where no TT muscle contraction is possible. Our results from Figure 3 would indicate that in contraction of the stapedius and TT muscles, both increase the tympanometric impedance of the middle ear. The two human subjects who could DISCUSSION Overall, the investigations in this work tend to reinforce and support each other in several aspects. First, all seem to point to contraction of the TT causing attenuation of low-frequency acoustic energy transmission through the middle ear. This can be inferred from the decreased low-frequency stapes and umbo vibrations in temporal bone LDV, the computer model results, and finally the audiogram in one subject who could voluntarily contract his MEM for long enough to obtain this measure. Hence, certainly we would expect a low-frequency conductive component with TT contraction, but whether there is a partial sensorineural component is not easy to infer from our results. The small drop in the bone curve in subject 1 could also have been from masking from the tinnitus he experienced with TT contraction. Second, all the results seem to point to a decrease in tympanometric static compliance with TT contraction (measured with a standard 226 Hz probe tone). This distinguishes TT contraction from other entities such as otosclerosis or ossicular fixation or erosion, which often Laryngoscope 123: April 2013 Fig. 7. Model simulations of the effects on admittance of tensor tympani (TT) contraction on admittance for (A) the tympanic membrane and (B) the stapes footplate. V ¼ velocity, F ¼ Force. Bance et al.: Markers of Tensor Tympani Muscle Contraction 1025 move their TM would also point to TT contraction causing an increase in acoustic impedance (Figs. 5 and 6), both in static compliance measurements with tympanometry and on dynamic changes using the reflex decay settings. In neither of these patients, nor in the temporal bones, could we see a reliable change in the orientation of the malleus handle, or shape of the eardrum with TT contraction. Eardrum movements that could be seen were quite subtle. The underlying shape of the eardrum or malleus is not a clue to static contraction. In this, we agree with Pau et al.,21 who conducted similar experiments to ours in five temporal bones. Pau et al. found a decrease in compliance, similar to our findings, and an increase in middle ear resonant frequency with force applied to the TT. The results of the temporal bone LDV experiments shown in Figures 2 and 3 would suggest that there is decreased transmission of low frequencies through the middle ear when the TT is contracted. Figure 2 shows single point recordings, and Figure 3 shows scanning laser recordings averaged over many points. In terms of amplitude, clearly, there is a graded reduction in low-frequency vibrations in both the umbo and the stapes footplate when increasing force is applied to the TT. Using single-point LDV, there appears to be little change at higher frequencies. The scanning LDV results show a similar low-frequency reduction in both the TM and stapes footplate. At the TM, the effects are a nicely graded reduction in low-frequency transmission with little effect on the higher frequencies. Also, there is little change in the first broad resonance peak frequency. For the footplate, a scanning laser is possibly more accurate, as the whole structure may rock, and single-point laser results may be somewhat misleading, as it does not show the net change in deflection of the structure, whereas the scanning laser will average over all recorded points. This may explain why the single-point measurements do not show an increase in high-frequency transmission with TT tension, whereas the scanning laser in Figure 5 clearly does for all weights except the 13-g weight. The scanning laser also shows a clear increase in the first broad resonance frequency of the stapes with TT tension. The computer model seems to qualitatively predict some similar findings to our empirical data, but not in all aspects. It does predict mostly a low-frequency drop in admittance at the stapes. It also predicts that TT contraction would cause a much greater effect on the stapes vibrations and resonant frequency than on the TM. Figure 3 shows that the stapes drop is bigger than the TM drop, but not hugely so. In both the TM and the stapes, there is a reduction in low-frequency vibrations, although with the TM, the peak amplitude changes very little with TT tension. The empirical data for the single laser point umbo recordings could be interpreted as showing this effect (Fig. 2A). The model also clearly shows an increase in high-frequency transmission for the stapes footplate, again similar to the effect seen in Figure 3B. Overall, the model is qualitatively similar, but not exactly the same, to what is seen empirically. Laryngoscope 123: April 2013 1026 Geometric and material property data differences between the actual bones tested and the values used in the simulation are most likely responsible for the lack of quantitative agreement. CONCLUSION Of the stimuli tested, the most effective stimulus for eliciting TT contraction is the startle reaction induced from a jet of air on the closed eye. It is very difficult to detect changes in the TM position alone due to TT contraction, so tonic contractions of the TT would be difficult to detect by visual inspection alone. The main effect of TT contraction seems to be an increase in middle ear stiffness, and this primarily affects the passage of low-frequency acoustic energy to the inner ear, resulting in a predominately low-frequency conductive hearing loss. Any change in inner ear hearing is slight, at least acutely. Pure sensorineural hearing loss (SNHL) is difficult to explain from TT dysfunction alone. The expected markers for TT contraction are: 1) a decrease in peak static compliance measured with acoustic tympanometry; and 2) a low-frequency conductive hearing loss, with a possible smaller low-frequency SNHL component. These markers should be sought in disorders thought to be associated with TT spasm (such as Meniere’s disease), or in subjects with tinnitus, otalgia, low-frequency SNHL, or other symptoms/signs where tonic TT spasm is thought to be involved. Future work would look for these markers in various otologic disorders, particularly Meniere’s disease. Acknowledgments Jean MacLachlan was a summer medical student who collected some of the data on the electing stimuli for TT contraction. BIBLIOGRAPHY 1. Weber FE. Tenotomie des Tensor Tympani. Monatsschr Ohrenheilkd 1870; 10:120–126. 2. Kamerer DB Electromyographic correlation of the tensor tympani and tensor veli palatini muscles in man. Laryngoscope 1978;88:651–662. 3. Curtis AW. Myofascial pain-dysfunction syndrome: the role of nonmasticatory muscles in 91 patients. Otolaryngol Head Neck Surg 1980;88: 361–367. 4. Franz P, Hamzavi JS, Schneider B, et al. Do middle ear muscles trigger attacks of Meniere’s disease? Acta Otolaryngol 2003;123:133–137. 5. Klockhoff I. Impedance fluctuation and a ‘‘tensor tympani syndrome.’’ In: Proceedings of the 4th International Symposium on Acoustic Impedance Measurements; Lisbon Universidad Nova de Lisboa Ed Penha and Pizarro; September 25–28, 1979:69–76. 6. Rock EH. Objective tinnitus and the tensor tympani muscle. Int Tinnitus J 1995;1:30–37. 7. Djupesland G. Middle ear muscle reflexes elicited by acoustic and nonacoustic stimulation. Acta Otolaryngol Suppl 1964;188:287–292. 8. Wever GE, Lawrence M. The Tympanic Muscles in Physiological Acoustics. Princeton, NJ: Princeton University Press; 1954. 9. Bosatra A, Russolo M, Semeraro A. Tympanic muscle reflex elicited by electric stimulation of the tongue in normal and pathological subjects. Acta Otolaryngol 1975;79:334–338. 10. Klockhoff I, Anderson H. Reflex activity in the tensor tympani muscle recorded in man; preliminary report. Acta Otolaryngol 1960;51:184–188. 11. Greisen O, Neergaard E. Middle ear reflex activity in the startle reaction. Arch Otolaryngol 1975;101:348–353. 12. Salen B, Zakrisson JE. Electromyogram of the tensor tympani muscle in man during swallowing. Acta Otolaryngol 1978;85:453–455. 13. Salomon G, Starr A. Electromyography of the middle ear muscles in man during motor activities. Acta Neurol Scand 1963;39:161–168. 14. Bance M, Morris DP, Vanwijhe RG, Kiefte M, Funnell WR. Comparison of the mechanical performance of ossiculoplasty using a prosthetic malleus-to-stapes head with a tympanic membrane-to-stapes head Bance et al.: Markers of Tensor Tympani Muscle Contraction assembly in a human cadaveric middle ear model. Otol Neurotol 2004; 25:903–909. 15. Feng B, Gan RZ. Lumped parameter model of the human ear for sound transmission. Biomech Model Mechanobiol 2006;3:33–47. 16. Cheng T, Gan RZ. Experimental measurement and modeling analysis on mechanical properties of tensor tympani tendon. Med Eng Phys 2008; 30:358–366. 17. Garland P, Makki F, Deas R, Bance M. A lumped parameter mechanical model of TT muscle contraction of the middle ear. In: Proceedings of 2nd Pan-American/Iberian Meeting on Acoustics; Cancun, Mexico. Proceedings of Meetings on Acoustics 2011;11:050001. Available at: http://asadl.org/poma/resource/1/pmarcw/v11/i1/p050001_s1?bypassSSO¼ 12010. Accessed on October 2012. Laryngoscope 123: April 2013 18. Mulder JJS, Vantrappen G, Snik AFM, et al. The use of the startle reflex measurement in patients with various types of fixation of the ossicular chain. Scand Audiol 1993;22:257–260. 19. Ochi K, Ohashi T, Kinoshita H. Acoustic tensor tympani response and vestibular-evoked myogenic potential. Laryngoscope 2002;112: 2225–2229. 20. Lehnhardt E, Battmer RD, Becker D. Diagnostic reliability of ipsilateral evoked impedance changes of the tympanic membrane. Laryngol Rhinol Otol (Stuttg) 1977;56:683–694. 21. Pau HW, Punke C, Zehlicke T, Dressler D, Sievert U. Tonic contractions of the tensor tympani muscle: a key to some non-specific middle ear symptoms? Hypothesis and data from temporal bone experiments. Acta Otolaryngol 2005;125:1168–1175. Bance et al.: Markers of Tensor Tympani Muscle Contraction 1027