Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Blast-related ocular trauma wikipedia , lookup
Photoreceptor cell wikipedia , lookup
Vision therapy wikipedia , lookup
Idiopathic intracranial hypertension wikipedia , lookup
Mitochondrial optic neuropathies wikipedia , lookup
Retinal waves wikipedia , lookup
Visual impairment due to intracranial pressure wikipedia , lookup
Fundus photography wikipedia , lookup
Optical coherence tomography wikipedia , lookup
Diabetic retinopathy wikipedia , lookup
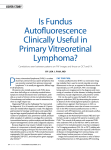
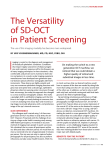
cover story Using Fundus Autofluorescence This is an essential tool for a definitive diagnosis. By Karl G. Csaky, MD F undus autofluorescence (FAF) is yet another diagnostic imaging modality that has drastically changed due to advances in research and technology. Previous diagnostic techniques required the injection of sodium fluorescein into the eye to highlight structures such as optic nerve drusen. These structures were then documented on high ISO film or monochrome digital sensors, with inconsistent and unreliable results. Today, diagnostic images can be captured by exciting naturally occurring chemicals in the eye. These chemicals absorb energy from light and then emit light at wavelengths longer than the excitation lightsource. This form of autofluorescence occurs in structures such as optic nerve drusen, astrocytic hamartomas, lipofuscin pigments in the retina, and the aging crystalline lens. Uses for FAF FAF imaging provides information beyond that obtained by imaging methods such as fundus photography or optical coherence tomography (OCT), and is particularly useful anytime there is unexplained vision loss or when detailed information is needed about the retinal pigment epithelium (RPE). It is a quick way to look at the integrity of the RPE and determine if there are any changes in its level that may explain changes in vision. FAF is also useful for defining the diagnosis of whitish deposits seen via fundus examination, subretinal deposits identified by OCT imaging, or when looking for any pertubations of retinal epithelium. In central serous retinopathy, Stargardt disease, adult vitelliform macular dystrophy (AVMD), along with a host of other retinal dystrophies, the lipofuscin leaves a very intense hyperfluorescence in a striking pattern, allowing physicians to confirm any preliminary diagnosis made with other imaging techniques. Finally, FAF makes it possible to precisely define areas of geographic atrophy, and its use is a requirement with any clinical trials in which geographic atrophy is relevant. Figure 1. OCT image shows retinal elevation with hyperreflective material. Case Study A 72 year-old woman was referred to me for possible injection of anti-VEGF agents for the treatment of choroidal neovascularization (CNV) secondary to age-related macular degeneration (AMD). The patient had noticed a relatively sudden change in vision in her right eye and was referred by a general ophthalmologist for a consultation. The first step with any patient is a standard visual exam. Her visual acuity in the right eye was 20/100 and 20/40 in the left eye. Her examination was otherwise unremarkable, and she reported no past history of previous vision problems, and her family’s ocular medical history was unremarkable. The patient’s anterior segment appeared normal with posterior chamber intraocular lenses in both eyes. Posteriorly, the periphery and cup-to-disc ratios were normal. Whitish/yellowish deposits on the macula were visible, predominantly on the right side, but there was no clear evidence of drusen or hemorrhage. The next step was OCT imaging, which revealed evidence of retinal elevation overlying a discrete region of September 2013 Retina Today 73 cover story FAF is clearly a secondary tool, but one that is invaluable because it shows things that other instrumentation does not. Figure 2. FAF reveals hyperfluorescent subretinal deposits. intense hyperreflective material with disruption of the RPE and some suspicion of the presence of subretinal fluid (Figure 1). However, the OCT images did not provide clear evidence of a neovascular process. We next performed fluorescein angiography (FA), which showed progressive staining of the lesion, but no clear evidence of discrete leakage. Finally, I performed FAF, which revealed an area of intense hyperfluorescent subretinal deposits corresponding to the area of the widest lesion on the fundus exam, characteristic of AVMD (Figure 2). Definitive Diagnosis AVMD is not an uncommon finding. In patients who present with vision loss and macular lesions, OCT imaging will show accumulation of lipofuscin rich material of unclear etiology, and FA will merely show progressive staining of material. Although the OCT presentation was highly suggestive of AVMD, the intense hyperfluorescence seen in the subretinal deposit is typically only found in retinal dystrophies, confirming the diagnosis of AVMD. Current treatment for AVMD is observation. It is crucial, however, to have a definitive diagnosis so that patients are not given incorrect treatment. Anti-VEGF has no impact on these lesions and is not indicated, and treatment of AVMD with photodynamic therapy has been associated with severe vision loss. This particular patient has been followed for 6 months and remains stable. OCT, FA, and FAF imaging were all performed with the Spectralis (Heidelberg Engineering), which, in addi74 Retina Today September 2013 tion to having the luxury of multiple imaging modalities in the same system, offers a unique tracking feature. The eye tracking system, called TruTrack, creates a detailed retinal map each time a patient is imaged, and this map is used to place follow-up scans in precisely the same location as the baseline scan. This allows careful and precise comparisons of one slice of the retina with the exact same slice from a previous visit. Without it, judgment of progression of pathology can be somewhat of a guess. Conclusion FAF is clearly a secondary tool, but one that is invaluable because it shows things that other instrumentation does not. Published literature has shown FAF to be useful in diagnostics, understanding pathophysiologic mechanisms, phenotype-genotype correlation, identification of predictive markers for disease progression and monitoring of novel therapies.1 Physicians who do not have access to FAF must rely on clinical acumen to make a diagnosis, or in cases where they are unsure, use fluorescein angiography. Overall, I find FAF to be an essential feature that helps me to fully manage my patients. n Karl G. Csaky is a vitreoretinal specialist with the Texas Retina Associates and is the T. Boone Pickens Senior Scientist at the Retina Foundation of the Southwest. Dr. Csaky states that he is a consultant for Heidelberg Engineering. Dr. Csaky can be reached at [email protected]. 1. Schmitz-Valckenberg S, Holz FG, Bird AC, Spaide RF. Fundus autofluorescence imaging: review and perspectives. Retina. 2008;28(3):385-409. Contact Us Send us your thoughts via e-mail to [email protected].