Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
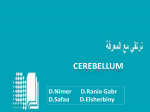
Introduction Lesions in the cerebellar peduncle include variou s pathological conditions: infarction, various primary or secondary degeneration, demyelinatiing disease, toxic metabolic diaease, trauma, and benign and malignant tumors. Their differential diagnoses are occasionally difficult. We illustrate the anatomy, pathology and imaging findings of the cerebellar peduncle. Anatomy Gross anatom y (Figure 1A-F). The cerebellum is connected to the brainstem by three cerebellar peduncles: 1) the inferior cerebellar peduncle (restiform body and juxtrarestiform body) 2) the middle cerebellar peduncle (brachium pontis), and 3) the superior peduncle (brachium conjunctivum) (1). The wall and lateral roof of the 4th ventricle are formed by the inner surfaces of the ce rebellar pedun cles; the rost ral portion by the superior peduncles; and the caudal portions by the inferior peduncles (Figure 1A -F). The middle cerebellar peduncle is lateral to inferior and superior peduncles and is not directly exposed to the cavity of the 4th ventricle. The middle cerebellar peduncle can be divided into three portions: brain stem portion, ventricular portion, and cerebellar portion (Figure 1E). This classification can be a useful application in surgery (2). Toshio Moritani MD, PhD, Akio Hiwatashi MD, Henry Z Wang MD, PhD, Yuji Numaguchi Numaguchi,, MD, PhD, Leena Ketonen MD, PhD, Sven E Ekholm MD,PhD MD,PhD,, Per-Lennart A Westesson MD, PhD, DDS Division of Diagnostic and Interventional Neuroradiology, Department of Radiology, University of Rochester Medical Center, Rochester NY F E-mail: [email protected] G. Cerebellar connections. The cortico-ponto-cerebellar pathway (corticopontine tract and pontocerebellar tract) is major afferent fibers through the middle cerebellar peduncle. Olivocerebellar fibers (afferent fibers) are through the inferior cerebellar peduncle. Efferent fibers mainly arise from the dentate nucleus to the red nucleus through the superior cerebellar peduncle (cerebello-rubro-thalamic tract). Figure 6. Wallerian degeneraion in the middle cerebellar peduncle. 50-year-old man with quadriparesis and loss of co nsciousness after chiropract ic. A Solvent encephalopathy (Figure 8) There have been a few case reports of middle cerebellar peduncle lesions in solvent encephalopathy (chronic toluene intoxication) in which the cerebral and cerebellar white matter, thalamus, basal ganglia, internal capsule, and brain stem are also involved (9, 10) (Figure 8). These patients' symptoms are usually composed of pyramidal tract and cerebellar signs. The middle cerebellar peduncle lesions can be p rimary or secondary degeneration. B Figure 8. Solvent encephalopathy. 38year-old man presenting with blurred vi sion, ataxi c speech and bilateral pyramidal signs. T2WI shows diffuse hyperintense lesions in the white matter of both temporal lobes and mildly hyperintense lesions in the pons and bilateral middle cerebellar peduncles (arrows). Cerebellar connections (Figure 1G). The cerebellum is linked to other parts of the brain by numerous efferent and afferent fibers that are grouped together on each side of the cerebellum in three peduncles (1). Most of the afferent tracts enter the cerebellum via the inferior and middle cerebellar peduncles. A few enter via the superior cerebellar peduncle. Afferent fibers are far more numerous that efferent fibers by a ratio of 40:1 (3). The cortico-pontocerebellar pathway, composed of the corticopontine tra ct and the pontocerebellar tract, i s major affe rent f ibers through the middle cerebellar peduncle. It arises from the cerebral cortex and enter the ipsilateral pontine nucleous and almost entirely crossed to the contralateral cerebellum. Olivocerebellar fibers form the large st component of the inferior cerebellar peduncle. Most of efferent tracts of the cerebellum are via the superior cerebellar peduncle. They mostly arise from dentate nucleus and decussate at the levels through the inferior collicu lus. Most of the fibers enter the contralateral red nucleus and project the cerebral cortex via the thalamus. Symptomatology Lesions of the cerebellar peduncle result in variable clinical symptoms, ranging from vertigo or vomiting as the only clinical presentation to facial palsy, ataxia, nystagmus, diplopia, dysphagia, dysarthria, deafness, contralateral motor weakness, trigeminal sensory loss, dysmetria of the limb, loss of pain and temperature sense, Horner's syndrome, and "locked-in" syndrome (1,4,5). Imaging of normal anatom y(Figure 1F). The posterior fossa is difficult to evaluate on CT because of poor contrast resolution and artifacts. MRI more clearly demonstrates the anatomy and pathology of the middle cerebellar peduncle in the posterior fossa than does CT. FLAIR images occasionally show a slight increase in signal intensity in normal middle cerebellar peduncles (Figure 1F). s s i i m s B A, B, FLAIR image and DWI show a hyperintense lesion, representing a small acute infarct in the left inferior cerebellar peduncle. D m B V C F A m i B Figure 3. An infarct in the inferior cerebel lar peduncle. 57year-old man with ataxia and diplopia. A B Figure 4. infarcts involving the superior cerebellar peduncle. 58year-old man with loss of consciousness. i A. Coronal FLAIR image. B,C,D, Sagittal T1WI. E, Axial T2WI. F. FLAIR image occasionally shows slightly high signal intensity in the normal superior (not shown), inferior and middle cerebellar peduncles. middle cerebellar peduncle (m), superior cerebellar peduncle (s), inferior cerebellar peduncle (i). brain stem portion (B), ventricular portion (V), and cerebellar portion (C) of the middle cerebellar peduncle. E A, B. DWI and T2WI shows hyperintense lesions in the right cerebellar hemisphere and the left side of the pons at 10 days after onset, which represents subacute hemorrhagic infarcts. C, D. On follow-up MRI at 8 months after onset, old infarcts show very high intensity on T2WI and low intensity on FLAIR image as CSF. Symmetrical round hyperintense lesions in bilateral middle cerebellar peduncles are seen on T2WI and FLAIR image (arrows). These lesions represent wallerian degeneration of the pontocerebellar tracts secondary to pontine infarction. E. T2WI at the level of the medulla demonstrates symmetric hyperintense lesions corresponding to the bilateral olivary nuclei, representing hypertrophic olivary degeneration (arrows). F. On the pathological specimen of another patient, wallerian degeneration of the pontocerebellar tracts is recognized as symmetric rounded lesions (arrows) in bilateral middle cerebellar peduncles and extends out to the mossy fibers in the cerebellar cortex (open arrows) (Ref. 3. Int J Neuroradiol Figure 2. An infarct in the inferior cerebellar peduncle. 72-year-old man with vertigo. A,B. T2WI and DWI at 24 hrs after onset clearly reveal homogenous round hyperintensity areas representing acute infarcts in the bilateral middle cerebellar peduncles and both cerebellar hemispheres. i E The inferior cerebellar peduncle is mainly supplied by the posterior inferior cerebellar artery (PICA). The middle cerebellar peduncle is supplied by the anterior inferior cerebellar artery (AICA) and partly by the superior cerebellar artery (SCA). The superior cerebellar peduncle is mainly supplied by the SCA. These arteries vary greatly in origin, size, course, and supply area, the aera of infarction are variable in extent and location, ranging from a small infarct localized into the cerebellar peduncle (Figure 2 and 3) to la rge involvement of the cerebella r hemisphere, and can be associated with the involvement of pons, midbrain, thalamus and occipital lobe (Figure 4) (4). Bilateral AICA territory infarcts a re very rare (Figure 5), and can occur due to hypoperfusion in the watershed area between the AI CA and the SCA (6). D 1998;4:171-177. Toshihiro O'uchi MD with permission). F G. Wallerian degeneration in bilateral middle cerebellar peduncles The lesion involving the pontine nucleus can also involve the pontocerebellar tract from the contralateral pontine nucleus, which results in wallerian degeneration in bilateral middle cerebellar peduncles. B B Walle rian degenera tion of the pon tocerebella r trac ts secondary to pontine hemorrhage or infarction (Figure 6). Wallerian degeneration secondary to pontine hemorrhage or infarction is usually bilateral. Differentiating from infarction is important. This is because of damage to both ipsilateral pontine nuclei (which deliver axons to the contralateral cerebellar hemisphere) and the ipsilateral axons (which originate from the contralateral pontine nuclei and course into the ipsilateral cerebellar hemisphere) (Figure 6G) (3). The T2 prolongations were first recognized from 26 days to 4.5 months after insult Theoretically, the wallerian degeneration of the pontocerebellar tracts should extend out to the mossy fibers in the cerebellar cortex, as seen on the pathological specimen; however this is beyond the resolution of MRI(3). Hypertrophic olivary degeneration occasionally coexists with these lesions, because the lesion can also involve the area in the Guillain-Mollaret triangle (Figure 6H) (7). Bilateral middle cerebellar peduncle lesions were present in a patient with herpes encephalitis with bilateral temporal lobe involvement (Figure 9). The cause of these lesions is unknown. Secondary transneuronal degeneration via bilateral cortico-ponto-cerebellar pathways may be one of the possible explanations for these lesions (F igure 6G) (11). Figure 9. Herpes encephalitis A. T2WI shows diffuse hyperintense lesions in the cortex and white matter in bilateral temporal lobes, which represents herpes encephalitis. B. Coronal FLAIR image shows hyperintense lesions in the bilateral middle cerebellar peduncles (arrows) and the temporal lobes. Crossed cerebellar diaschisis and atrophy (Figures 10 and 11) Crossed cerebellar diaschisis and atrophy presumed to be associated with transneuronal metabolic depression in the cerebellum through corticoponto-cerebellar pathways (middle cerebellar peduncle) or other pathways su ch as cerebello-rubro-thalamic tract (superior cerebellar peduncle) (Figure 10) (12,13) Unilateral atrophy of the middle cerebellar peduncle and cerebellar hemisphere occurs as a sequela of ischemic or destructive injury of the contralateral cerebral hemisphere (14). These findings are found in children with a history of extreme prematurity, perinatal intracranial hemorrhage, and recurrent seizures (Figure 11). C A. FLAIR image shows hyperintensity lesions in the right cerebellar hemisphere (arrows) and contralateral diffuse cerebral hyperintensity associ ated with status epilepticus. B,C. FLAIR images at the level of the brain stem show a hyperintense lesion in the right superior cerebellar peduncle (arrows). These findings suggest that crossed cerebellar diaschi sis of this case is related to retrograde transneuronal degeneration through the cerebello-rubro-thalamic tract. Figure 11. Crossed cerebellar atrophy B A. B. T2WI shows a hyperintense lesion in the central pons representing CPM. T2WI also shows symmetrical round lesions in the bilateral middle cerebellar peduncles (arrows). These lesions maybe due to myelinolysis itself or secondary degeneration. Leukodystrophy and leukoencephalopathy (Figure 13). Some kinds of leukodystrophy and leukoencephalopathy can also involve in the cerebellar peduncles. This leukoencephalopathy with vanishing white matter is an autosomal recessive disorder with chronic and progressive episodes of rapid deterioration, provoked by fever and minor head trauma. This is primarily an axonopathy, with myelin being secondarily affected (19) (Figure 13). A. T2WI shows diffuse white matter signal abnormalities similar to CSF intensity. B. T2WI also shows hyperintense lesions in the central tegmental tracts (arrows), pyramidal tracts (arrows), and inferior and middle cerebellar peduncles with atrophy (arrows). A B Demyelinating disease: multiple sclerosis (MS), acute disseminated encephalomyelitis (ADEM) and progressive multifocal leukoencephalopathy (PML) (Figures 14-16) Brain stem and cerebellar involvement including cerebellar peduncles is common in patients with MS and ADEM. Cerebellar symptoms and signs are commonly seen in 50-80% in MS patients. On MRI brainstem lesions in 68% and cerebellar lesions in 49%-88% were detected (20). These lesions in MS or ADEM are often bilateral but asymmetric (Figures 14 and 15). In PML involvement of the posterior fossa including the cerebellar peduncles is also common (32%). Isolated disease in the posterior fossa is in 10% of PML patients (21) (Figure 16). Figure 14. MS. 40-year-old woman with multiple sclerosis, presenting with speech disturbance and ataxia. A, B.T2WI shows multiple asymmetric hyper-intense lesions in the pons, middle cerebellar peduncles (arrows) cerebellar hemispheres, and in the deep white matter, which is characteristic of MS. A B A, B.T2WI and FLAIR image shows hyperintense lesions in the pons, and inferior cerebellar peduncles (arrows), and in the callosomarginal interface in the deep white matter, which is characteristic of MS. A. T2WI shows right cerebral atrophy with ventricular dilatation representing a sequela of perinatal intracranial hemorrhage. B. T2WI through the posterior fossa shows atrophy of the contralateral cerebellar middle cerebellar peduncle (arrow) and hemisphere. Wallerian degeneration of ipsilateral brain stem is also seen (arrow). A,B A mass lesion is located in the ventricular portion to the cerebellar portion of the left middle cerebellar peduncle. It is high signal on T2WI and low signal on T1WI and with no enhancement (not shown). This lesion can be removable by surgery. B B 17-year-old female presenting with hearing loss and progressive ataxia A B A,B Axial T2WI and sagittal T1WI shows an extra-axial cerebellopontine angle mass lesion which deviates the left middle cerebellar peduncle posteriorly and superiorly (arrows). Neurofibrom atosis (Figure 19) Hamarto matous lesions are obse rved in 80% of all patients with neurofibromatosis type 1. Multiple lesions in the basal ganglia, optic radiation, brainstem, and cerebellar peduncles are common (Figure 19). Pathologically, these lesions are foci of hyperplastic or dysplastic glial proliferation and considered malformations rather than neoplasms. Figure 19. Neurofibromatosis type 1. 4-year-old girl presenting with developmental delay. A,B T2WI and FLAIR image show multiple asymmetric lesions in the pons, middle and inferior cerebellar peduncles, and A cerebellum. B Diffuse axonal injury (DA I) (Figure 20) The gray-white matter interface, the corpus callosum, and dorsal aspect of the upper brainstem including the superior cerebellar peduncle are three specific areas for the occurrence of DAI. Other less frequent locations include the caudate nuclei, thalamus and internal capsule. Cerebellar involvement including the middle cerebellar peduncle is uncommon (Figure 20). Figure 20. DAI. 29-year-old woman with DAI, presenting with loss of consciousness after motor vehicle accident. A B A. FLAIR image shows a hyperintense lesion in the left middle cerebellar peduncle to cerebellar hemisphere due to DAI. B. DWI shows hyperintense lesions in the corpus callosum and bilateral internal capsules, which is typical findings of DAI. Conclusion 1) Carpenter MB. Cerebellum. In, Core Textbook of Neuroanatomy. 5th edition. Baltimore, MD: Williams &Wilkins, 1996;583-623. 2) Tomita T. Surgical management of cerebellar peduncle lesions in children. Neurosugery 1986;18:568-575. 3) O'uchi T. Wallerian degeneration of pontocerebellar tracts after pontine hemorrhage. Int J Neuroradiol 1998;4:171-177. 4) Amenco P, Rosengart A, DeWitt D, Pessin MS, Caplan LR. Anterior inferior cerebellar artery teritory infarcts. Mechanisms and clinical features. Arch Neurol 1993;50:154-161. C, D. Hyperintense lesions are also seen in the midbrain, and the superior cerebellar peduncle (arrows). A. T2WI shows an isolated hyperintense lesion in the right middle cerebellar peduncle extending into the cerebellar hemisphere. B. Gd-enhanced T1WI shows this lesion as hypointensity with no A enhancement. A Figure 18. Acoustic schwannoma. Re feren ces A 5) Milandre L, Rumeau C, Sangla I, Peretti P, Khalil R. Infarction in the territory of the anterior inferior cerebellar artery: report of five cases. Neuroradiology 1992;34:500-503. 6) Akiyama K, Takizawa S, Tokuoka K, Ohnuki Y, Kobayashi N, Shinohara Y.Bilateral middle cerebellar peduncle infarction caused by traumatic vertebral artery dissection. Neurology 2001;56:693-694. 7) Kitajima M, Korogi Y, Shimomura O, Sakamoto Y, Hirai T, Miyayama H, Takahashi M.Hypertrophic olivary degeneration: MR imaging and pathologic findings. Radiology 1994;192:539-543. 8) Mangat KS, Sherlala K. Cerebellar peduncle myelinolysis: case report. Neuroradiology 2002;44:768-769. D Figure 16. PML. 25-year-old man presenting with right-sided weakness and headache. He has had a history of HIV infection. B Figure 17. Low grade astrocytoma. 4-year-old boy presenting with autism. Lesions in the middle cerebellar peduncle include various pathological conditions, ranging from infarction, tumor, infection, trauma and demyelination to primary and secondary degeneration. Understanding the anatomy, pathology, imaging characteristics is important for the differential diagnosis of lesions in the middle cerebellar peduncle. C A Benign tumors such as astrocytoma or cavernous angioma can involve in the cerebellar peduncle (Figures 17). An extra-axial tumor such as benign acoustic schwannoma occasionally displaces the middle cerebellar peduncle (Figure 18). Malignant tumors such as metastasis or glioblastoma multifo rme also o ccu r in the cerebellar peduncle. Tumors involving the ventricular portion or the cerebellar portion of the middle cerebellar peduncle can be removed by surgery (3). A, B. Axial and sagittal FLAIR images show hyperintensity in the middle (arrows) and inferior cerebral peduncles (arrows). C. Axial FLAIR image also shows cruciform hyperintensity in the transverse pontine fibers on the anterior and lateral aspect of the pons. The tegmentum (arrows ) and the pyramidal tracts (arrows) are spared. Figure 15. MS. 57-year-old man presenting with speech disturbance and ataxia. B Tumor (Figures 17 and 18). C B B 19-year-old female. She had a history of recurrent seizures and perinatal intracranial hemorrhage. A A An 11 year-old boy. A A Figure 7. CPM 50-year-old female presenting with loss of consciousness after rapid correction of hyponatremia. Figure 12. Ol ivopontocerebellar atrophy (sporadic type). 54-yearold woman presenting with dysarthric speech and dizziness. 40-year-old male presenting with a seizure. 27-year-old male, presenting with status epilepticus. He has a history of recurrent generalized seizures. Symmetrical lesions in bilateral middle cerebellar peduncles without central pontine myelinolysis (CPM) was reported as cerebellar peduncle myelinolysis (8). However, in our case, bilateral cerebellar peduncle lesions accompanied by CPM (Figure 7). These lesions are presumed to be due to myelinolysis itself or secondary degeneration related to CPM. OPCA is a degenerative disease characterized by atrophy of the pons, middle cerebellar peduncles, and cerebellar hemispheres. There are characteristic histologic changes, such as loss of specific fiber tracts and the presence of gliosis in the pons, middle cerebellar peduncles and cerebellum (15). The fibers affected in the pons are the transverse pontine fibers, while the pyramidal tracts and tegmentum are spared (Figure 12). Increased hyperintensity in the middle cerebellar peduncles are also reported in other multiple system atrophy, autosomal do minant spinocerebellar atrophy (16), Wilson’s disease, non-Wilsonian hepatocerebral degeneration (17), and fragile X syndrome (18). Figure 13.Leukoencephalopathy with vanishing white matter. Figure 10. Crossed cerebellar diaschisis Osmotic myelinolysis (Figure 7). A Herpes encephalitis (Figure 9) H. Guillain-Mollaret triangle and hypertrophic olivary degeneration The lesion involving the pontine nuclei can extend into the areas within the Guillain-Mollaret triangle, which causes hypertrophic olivary degeneration. Figure 5. Bilateral infarcts in the middle cerebellar peduncle. 80year-old man with ataxia and vertigo. m C Infarction (Figures 2-5) A, B, FLAIR image and DWI show hyperintensity lesionsin the left cerebellar hemisphre, and the midbrain including the left superior cerebellar peduncle. A m A C A, B, T2WI and DWI show a hyperintense lesion, representing an acute infarct in the right middle cerebellar peduncle. Figure 1. Normal anatomy. Olivopon toce rebellar atrophy (OPCA) and othe r p rimary degenerative diseases (Figure 12). Anatomy and Pathology of the Cerebellar Peduncle 9) Aydin K, Sencer S, Demir T, Ogel K, Tunaci A, Minareci O.Cranial MR findings in chronic toluene abuse by inhalation. AJNR Am J Neuroradiol 2002;23:1173-1179. 10) Uchino A, Kato A, Yuzuriha T, Takashima Y, Heijima S, Murakami M, Endoh K, Yoshikai T, Kudo S. Comparison between patient characteristics and cranial MR findings in chronic thinner intoxication. Eur Radiol 2002;12:1338-1341. 11) Thajeb P, Shih BF, Wu MC. Crossed cerebellar diaschisis in herpes simplex encephalitis. Eur J of Radiol 2001;38:55-58. 12) Pantano P, Baron JC, Samson Y, et al. Crossed cerebellar diaschisis: further studies. Brain 1986;109:677-694. 13) Chung HD. Retrograde crossed cerebellar atrophy. Brain 1985;108;811-889. 14) Rollins NK, Wen TS, Dominguez R. Crossed cerebellar atrophy in children: a neurologic sequela of extreme prematurity. Pediatr Radiol 1995;25:S20-25. 15) Savoia rdo M , Strada L, Gir otti F, Zimm erma n RA, G risoli M, T esta D, Petr i l o R .Olivo pontocer ebella r atr ophy:MR dia gnosis an d relationship to mu ltisystem a troph y. R adiology 1990;17 4:693- 696. 16) Nakaga wa N , Katayama T , Makita Y, et al. A case of spinocer ebella r ata xia type 6 mimicking olivo pontocer ebellar at rophy. N eur orad iology 199 9;41:503 -505. 17) Lee J, Lacomis D , Co mu S, et al. Acquired hepato cer ebr al dege nera tio n : MR and pathologic findings. AJNR AM J N eur orad iol 199 8;19:485 -487. 18) Brun berg JA , Jacquemo nt S, Hag erma n RJ, et al. Fr agile X prem utation car riers: C hara cter i stic MR im aging findings of ad ult male patients with pr ogr essive cereb ellar and cognitive dysfun ction. AJNR Am J Neur or adiol 2 002;23:1 757- 1766 19) van der Knaap MS, Ba rth PG , G abre els F J, et a l. A ne w leukoencepha lo pathy with vanish ing white matte r. Ne urolog y 19 97;48:84 5-85 5. B 20) Ormerod IE, Miller DH, McDonald WI, du Boulay EP, Rudge P, Kendall BE, Moseley IF, Johnson G, Tofts PS, Halliday AM. The role of NMR imaging in the assessment of multiple sclerosis and isolated neurological lesions. A quantitative study. Brain 1987;110:1579-1616. 21) Whiteman ML, Post MJ, Berger JR, Tate LG, Bell MD, Limonte LP. Progressive multifocal leukoencephalopathy in 47 HIV-seropositive patients: neuroimaging with clinical and pathologic correlation. Radiology 1993;187:233-40.