Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Infectious and
Parasitic disease
2nd Year Pathology 2010
Topics
Types of organisms.
Host barriers to organisms.
Methods of invasion by organisms.
Types of response they cause within the
body.
Organisms by system.
2nd Year Pathology 2010
Classification of organisms
Viruses
Bacteria
Fungi
Nucleic acids
DNA or RNA
DNA or RNA
DNA or RNA
Nuclear
membrane
No
No
Yes
External cell
wall
No
Yes
Yes
Antibiotic
sensitivity
No
Yes
No
Replication
Within host cells
(can’t replicate
themselves)
Within and
outside host
cells by binary
fission
Within and
outside host
cells by binary
fission and
sexually
2nd Year Pathology 2010
Classification of bacteria
Gram positive
1.
2.
Rods (bacilli)
Cocci
Gram negative
- Can be further divided
into anaerobic and
aerobic
2nd Year Pathology 2010
Classification of viruses
1.
2.
DNA
RNA
Further classification:
Single or double
strand
Envelope on no
envelope
2nd Year Pathology 2010
Host barriers to organisms
Intact skin
Mucosal surfaces
Their secretory and excretory products
Lysozyme secreted by tear glands
Acid gastric juice
2nd Year Pathology 2010
Defenses in gut
Acid gastric juice.
Viscous mucous layer covering gut.
Lytic pancreatic enzymes and bile
detergents.
Secreted IgA antibodies.
2nd Year Pathology 2010
Modes of transmission
Aerosol
Mucosal contact
Bloodstream
Placental-foetal route
2nd Year Pathology 2010
How microorganisms cause disease
1.
2.
3.
Contact or enter host cells and directly
cause cell death.
Release endotoxins or exotoxins that kill
cells.
Induce host cellular responses that are
directed against invader but cause
additional host damage such as scarring
and hypersensitivity reactions.
2nd Year Pathology 2010
Special techniques for diagnosing infectious
agents
Gram stain
Most bacteria
Acid-fast stain
Mycobacteria, nocardiae
Silver stains
Fungi, legionellae, pneumocystis
Periodic acid-Schiff
Fungi, amoebae
Mucicarmine
Cryptococci
Giemsa
Campylobacteria, leishmaniae,
malaria parasites
Antibody probes
Viruses, rickettsiae
Culture
All classes
DNA probes
Viruses, bacteria, protozoa
2nd Year Pathology 2010
Inflammatory responses to
infection
5 major patterns
1.
2.
3.
4.
5.
2nd Year Pathology 2010
Suppurative inflammation
Mononuclear and granulomatous inflammation
Cytopathic-cytoproliferative inflammation
Necrotising inflammation
Chronic inflammation and scarring
Suppurative Inflammation
Production of large amounts of pus
Comprised of:
Neutrophils (attracted by chemoattractants generated by bacteria)
Necrotic cells
Oedematous fluid
Certain organisms (Staphylococcus) localised suppuration –
pyogenic
e.g. acute appendicitis
Abscess = focal, localised collection of purulent inflammatory
tissue
Bacteria also attract neutrophils by releasing endotoxins that
stimulate macrophages to release IL-1 or TNF
2nd Year Pathology 2010
Mononuclear and
granulomatous inflammation
Diffuse, predominantly mononuclear infiltrate
in response to viruses, intracellular bacteria,
spirochetes, intracellular parasites or
helminths.
Occurs when aggregates of altered
macrophages form around necrotic focus or
fuse to form giant cells.
e.g. M. tuberculosis
2nd Year Pathology 2010
Cytopathic, cyto-proliferative
inflammation
Characteristic of viral mediated damage in
absence of host inflammatory response.
Viral particles may be visible as inclusions or
cause cells to fuse (e.g. measles,
herpesviridiae)
Can stimulate epithelial cells to proliferate
(e.g. warts)
2nd Year Pathology 2010
Necrotising Inflammation
Organisms that secrete toxins (e.g.
Clostridium perfringens) cause rapid and
severe tissue damage.
Cell death is predominant feature
Resemble ischaemic necrosis in appearance
Disruption of nuclear staining and preservation of
cellular outlines.
2nd Year Pathology 2010
Chronic Inflammation and
scarring
Final common pathway of many infections
Leads to healing or extensive scarring
Can see similar pattern in response to
physical or chemical agents
2nd Year Pathology 2010
Acute Inflammation
Acute inflammation is
marked by an increase
in inflammatory cells.
Perhaps the simplest
indicator of acute
inflammation is an
increase in the white
blood cell count in the
peripheal blood, here
marked by an increase
in segmented
neutrophils (PMN's).
2nd Year Pathology 2010
Seen here is vasodilation with exudation that
has led to an outpouring of fluid with fibrin into
the alveolar spaces, along with PMN's. The
series of events in the process of inflammation
are:
1.
Vasodilation: leads to greater blood flow to the
area of inflammation, resulting in redness and
heat.
Vascular permeability: endothelial cells become
"leaky" from either direct endothelial cell injury
or via chemical mediators.
Exudation: fluid, proteins, red blood cells, and
white blood cells escape from the intravascular
space as a result of increased osmotic pressure
extravascularly and increased hydrostatic
pressure intravascularly
Vascular stasis: slowing of the blood in the
bloodstream with vasodilation and fluid
exudation to allow chemical mediators and
inflammatory cells to collect and respond to the
stimulus.
2.
3.
4.
2nd Year Pathology 2010
Acute inflammation
The PMN's seen here are in
alveoli, indicative of an
acute bronchopneumonia of
the lung. The PMN's form
an exudate in the alveoli.
This patient had a
"productive" cough because
large amounts of purulent
sputum were produced. The
source, the neutrophilic
alveolar exudate, is seen
here.
2nd Year Pathology 2010
Here is an example of
the fibrin mesh in fluid
with PMN's that has
formed in the area of
acute inflammation. It is
this fluid collection that
produces the "tumor" or
swelling aspect of acute
inflammation.
2nd Year Pathology 2010
A purulent exudate is seen beneath the meninges in the brain of this patient
with acute meningitis from Streptococcus pneumoniae infection. The exudate
obscures the sulci.
2nd Year Pathology 2010
Chronic inflammation is more difficult to understand, because it is so
variable. Seen here is chronic endometritis with lymphocytes as well as
plasma cells in the endometrial stroma. In general, the inflammatory infiltrate
of chronic inflammation consists mainly of mononuclear cells ("round cells"):
lymphocytes, plasma cells, and macrophages.
This is a case of viral hepatitis
C which is at a high stage with
extensive fibrosis and
progression to macronodular
cirrhosis, as evidenced by the
large regenerative nodule at
the center right.
The screening laboratory test
for this form of viral hepatitis is
the hepatitis C antibody test.
Hepatitis C accounts for most
(but not all) cases formerly
called "non-A, non-B hepatitis".
In addition to this serologic test
PCR and genotyping can be
performed.
2nd Year Pathology 2010
This is a healing biopsy site on
the skin seen a week following
the excision.
The skin surface has reepithelialized, and below this is
granulation tissue with small
capillaries and fibroblasts
forming collagen.
After a month, just a small
collagenous scar will remain.
2nd Year Pathology 2010
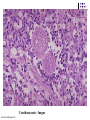
Cellular interactions with chronic inflammation
There is a small tan-yellow subpleural
granuloma in the mid-lung field on the
right. In the hilum is a small yellow tan
granuloma in a hilar lymph node next
to a bronchus. This is the "Ghon
complex" that is the characteristic
gross appearance with primary
tuberculosis. In most persons, the
granulomatous disease will not
progress. Over time, the granulomas
decrease in size and can calcify,
leaving a focal calcified spot on a
chest radiograph that suggests
remote granulomatous disease.
2nd Year Pathology 2010
The Ghon complex is seen here at closer range. Primary tuberculosis is
the pattern seen with initial infection with tuberculosis in children.
Reactivation, or secondary tuberculosis, is more typically seen in adults.
2nd Year Pathology 2010
Here are two pulmonary granulomas. Granulomatous inflammation typically
consists of mixtures of cells including epithelioid macrophages, giant cells,
lymphocytes, plasma cells, and fibroblasts. There may even be some
neutrophils.
2nd Year Pathology 2010
Giant cells are a "committee" of epithelioid macrophages. Seen here
are Langhans type giant cells in which the nuclei are lined up around
the periphery of the cell. Additional pink epithelioid macrophages
compose most of the rest of the granuloma.
2nd Year Pathology 2010
This is an acid fast stain of Mycobacterium tuberculosis (MTB). Note the
red rods--hence the terminology for MTB in histologic sections or smears:
acid fast bacilli.
2nd Year Pathology 2010
Two foreign body giant cells are seen just to the right of center
where there is a bluish strand of suture material from a previous
operation.
2nd Year Pathology 2010
This is cytomegalovirus (CMV) infection in the lung. Note the very large
cells that have large violet intranuclear inclusions with a small clear halo.
Basophilic stippling can be seen in the cytoplasm.
2nd Year Pathology 2010
An acute duodenal ulcer
2nd Year Pathology 2010
The strongest association with Helicobacter pylori is with duodenal peptic
ulceration--over 85% of duodenal ulcers. Seen here is a penetrating acute
ulceration in the duodenum just beyond the pylorus.
2nd Year Pathology 2010
Gastritis is often accompanied by infection with Helicobacter pylori. This
small curved to spiral rod-shaped bacterium is found in the surface
epithelial mucus of most patients with active gastritis. The rods are
seen here with a methylene blue stain.
2nd Year Pathology 2010
This yellow-green exudate on the surface of an inflamed, hyperemic
(erythematous) bowel mucosa consists of many neutrophils along with
fibrin and amorphous debris from dying cells.
2nd Year Pathology 2010
Budding cells with pseudohyphae seen here are characteristic for Candida infection.
2nd Year Pathology 2010
With a PAS stain, the budding cells and pseudohyphae (short filaments that are
not true hyphae) of Candida stain bright red.
2nd Year Pathology 2010
This is a microscopic section from the edge of one of a group of small round
clear vesicles on the skin, just above the lip. Notice the mauve to pink
homogenous intranuclear inclusions in the epithelial cells of the epidermis.
This is typical for Herpes simplex virus (HSV) infection. The most common
sites for Herpes simplex virus infections (either primary or reactivation) are
skin and mucus membranes. HSV type I is seen most often in oral cavity,
while HSV type II is more commonly
a sexually
transmitted disease.
Herpes
simplex
2nd Year Pathology 2010
By electron microscopy, viral particles of any herpesvirus appear as arrays
and scattered single particles as shown here in a nucleus of a neuron from
the cerebrum from a patient with herpes simplex encephalitis. Herpesviruses
are large encapsulated viruses that contain double-stranded DNA in the
nucleocapsid surrounded by the viral envelope.
2nd Year Pathology 2010
This is Cryptococcus neoformans infection of the lung. There are
numerous organisms that have a large mucoid capsule, giving the
appearance of a clear zone around a faint round nucleus.
2nd Year Pathology 2010
This is a Cryptococcus neoformans meningitis stained with GMS to reveal
the nuclei. In this AIDS patient, the organisms didn't even bother to make a
capsule. The budding cells of Cryptococcus have a narrow base.
2nd Year Pathology 2010
The little blue organisms lined up along the brush border of the small intestinal
epithelium are Cryptosporidium parvum organisms causing the disease
cryptosporidiosis. This infection may cause a mild diarrhea in immunocompetent
persons but more severe illness in immunocompromised hosts.
Cryptosporidium
2nd Year Pathology 2010
Cryptosporidium parvum
Coccidian protozoan parasite.
Causes watery diarrhoea in normal children.
Chronic debilitating diarrhoea in patients with
AIDS.
Not killed by chlorine.
Adhere to intestinal and colonic epithelial
cells.
2nd Year Pathology 2010
2nd Year Pathology 2010
Giardia lamblia
Most prevalent pathogenic intestinal
protozoan worldwide.
Infection may be subclinical or may cause
acute or chronic diarrhoea.
Not killed by chlorine.
Reside in duodenum.
Adhere to but do not invade intestinal
epithelial cells.
2nd Year Pathology 2010
Histoplasma - fungus
2nd Year Pathology 2010
Histoplasma
2nd Year Pathology 2010
Coccidomycosis - fungus
2nd Year Pathology 2010
This is a scabies mite. The official name is Sarcoptes scabiei. These little
organisms burrow in the epidermis, usually on the hands but sometimes
elsewhere, and produce itching along the linear burrows. These lesions
are often excoriated because of the itching.
2nd Year Pathology 2010
Lice are arthropods of the class Insecta which generally inhabit hair and bite
the human host for a blood meal.
At the left is the head louse (Pediculus humanis capitis) and at the right is the
crab (pubic) louse (Phthirus pubis).
2nd Year Pathology 2010
2nd Year Pathology 2010
2nd Year Pathology 2010
Pneumocystis carinii
A ubiquitous organism, thought to be a fungus.
Produces no disease in normal individuals.
Severe pneumonia in most patients with AIDS and
in children with protein-calorie malnutrition.
Alveolar air spaces filled with pink, foamy
amorphous material composed of proliferation
parasites and cell debris.
2nd Year Pathology 2010
Malaria - Plasmodium falciparum
2nd Year Pathology 2010
2nd Year Pathology 2010
2nd Year Pathology 2010
2nd Year Pathology 2010
2nd Year Pathology 2010
These red blood cells,
shown in a coloured
electron micrograph, are
infected with malarial
parasites.
The parasites swell the
cells and eventually break
out and spread, infecting
additional cells.
The more blood cells
infected, the more severe
the disease.
(a) Example of sequestration. Fresh coronal section of brain is swollen and slightly grey in
colour, and has no visible haemorrhages. Bottom left, high-power (x100) view of cortex
showing many parasitized vessels. Bottom right, single cortical vessel (under oil immersion
(x1,000) containing unpigmented parasites.
(b) Pattern of sequestration and microvascular pathology. Fixed coronal section of brain is
swollen and has multiple petechial haemorrhages in the cortical white matter. Bottom left,
high-power (x400) view of cortex showing haemorrhage surrounding a parasitized vessel.
Bottom right, higher-power (x400) view of cortex showing ring haemorrhage around vessel
containing parasites and a thrombus.
2nd Year Pathology 2010