Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
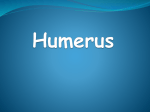
18 Bulletin • Hospital for Joint Diseases Volume 62, Numbers 1 & 2 2004 A Minimally Invasive Approach for Plate Fixation of the Proximal Humerus Michael J. Gardner, M.D., Matthew H. Griffith, M.D., Joshua S. Dines, M.D., and Dean G. Lorich, M.D. Abstract Plate fixation for unstable fractures of the proximal humerus has seen mixed results as evidenced by the trials of new methods of fixation. The deltopectoral surgical approach is most frequently used and requires significant muscle retraction and soft tissue stripping to expose the lateral humeral neck. This may contribute to avascular necrosis and fixation failure. Lateral approaches have been limited to 5 cm distal to the acromion because of the course of the anterior branch of the axillary nerve. A recent anatomic study has demonstrated the predictability of the position of the axillary nerve as it crosses the anterior deltoid raphe, which allows it to be isolated and protected, and dissection can be extended distally. In addition, no accessory motor branches to the anterior head of the deltoid cross the raphe, so extending an incision through the raphe after protecting the main motor branch of the axillary does not place the innervation to the anterior deltoid at risk. This surgical approach allows exposure of the proximal humerus and indirect reduction of the fracture, with subsequent locking plate fixation, adhering to the principles of biological fixation. W ith the advent of locking plates for fixation of proximal humerus fractures, modification of previously described surgical approaches is essential. The traditional deltopectoral approach for the anterior and lateral shoulder region requires extensive soft tissue dissection and muscle retraction to gain adequate exposure to the lateral aspect of the humerus Michael J. Gardner, M.D., Matthew H. Griffith, M.D., Joshua S. Dines, M.D., and Dean G. Lorich, M.D., are in the Department of Orthopaedic Surgery, Hospital for Special Surgery, New York, New York. Correspondence: Michael J. Gardner, M.D., Hospital for Special Surgery, 535 East 70th Street, New York, New York 10021. for application of a plate. Poor results following plate fixation of proximal humerus fractures may be related to complete exposure of the fracture fragments and devascularization during dissection and plating, or disruption of the critical blood supply to the humeral head. In light of the recent trend toward “biological fixation,” which focuses on fixed-angle screws, percutaneous bridge plating techniques, and avoidance of both fracture exposure and anatomic reduction,1 new surgical techniques must be developed for proper application of these devices. For access to rotator cuff tears using a mini-open approach, a small raphe-splitting incision from the acromion several centimeters distally has been well described.2-5 However, distal extension through the raphe of more than 3 or 4 centimeters has been discouraged because of the risk of damaging the axillary nerve. Recently, an anatomic study was performed to characterize the axillary nerve as it crosses the raphe between the middle and anterior heads of the deltoid.6 The anterior motor branch of the axillary nerve was found to cross the surgical neck at a predictable location relative to both the acromion and the greater tuberosity, and at the level of the raphe no other motor branches crossed to innervate the anterior head of the deltoid (Fig. 1). This data may be useful in allowing a more direct surgical approach to the proximal humerus for plate fixation of fractures. Surgical Technique A skin incision was made beginning at the anterolateral tip of the acromion. It was extended approximately 5 cm distally through the subcutaneous tissue layer to the level of the deltoid muscle (Fig. 2A). The avascular raphe separating the anterior and middle heads of the deltoid was then identified as a white band of connective tissue between the two muscular heads. Immediately adjacent to the raphe’s attachment to the acromion, it was incised Bulletin • Hospital for Joint Diseases Volume 62, Numbers 1 & 2 2004 19 B A Figure 1 Examples of exposure of the axillary nerve and posterior humeral circumflex vessels as they traverse the anterior deltoid raphe of a right cadaver shoulder. No other branches cross the raphe to innervate the anterior head of the deltoid. sharply for 2 cm along its length distally, enough to allow the insertion of the surgeon’s finger. The surgeon’s finger was then inserted into the rent in the raphe swept posteriorly to palpate undersurface of the deltoid and raphe. The axillary nerve was readily palpable as a cord-like structure between the deltoid and humerus as it exits the quadrangular space with the posterior humeral circumflex vessels. Once a general idea of the nerve’s location was obtained, the incision in the raphe was carefully extended distally by sharp dissection. Deep to the raphe, approximately 6.5 cm distal to the inferior edge of the acromion and 3.5 cm from the lateral prominence of the greater tuberosity, the axillary nerve and posterior humeral circumflex vessels were identified, isolated, and protected with a vessel loop (Fig. A 2B). With the neurovascular bundle protected, the incision may be extended distally to the deltoid tuberosity. The fracture may be indirectly reduced using ligamentotaxis and Kirschner wires in the head and shaft as joysticks. A fixed-angle plate can then be inserted along the lateral neck and shaft from proximal to distal underneath the nerve and vessels without excessive tension (Fig. 3). Discussion Operative fixation of proximal humeral fractures is indicated in approximately 20% of cases, the majority of which are three- and four-part fractures according to the Neer classification. 7 Treatment options vary from closed reduction with percutaneous pinning to hemiarthroplasty and the appropriate method depends on the fracture pat- B Figure 2 Illustration of the extended anterior acromial approach. The incision begins from the anterolateral corner of the acromion and extends distally. Deep to the subcutaneous layer, the anterior deltoid raphe, separating the anterior and middle heads of the deltoid, is identified (A). After palpating the undersurface of the deltoid to palpate the neurovascular bundle, the raphe is split and the nerve is isolated and protected (B). 20 Bulletin • Hospital for Joint Diseases Volume 62, Numbers 1 & 2 Figure 3 Demonstration in a cadaver shoulder of isolating the axillary nerve and posterior humeral circumflex vessels, followed by advancing a plate from proximal to distal deep to the neurovascular bundle. tern, surgeon’s experience, and specific patient factors such as age and bone quality. Key principles for obtaining a satisfactory result include stable fixation to allow early mobilization and minimization of soft tissue disruption to prevent further vascular compromise. Complications such as rotator cuff dysfunction, stiffness, avascular necrosis, malunion, and nonunion are relatively common with proximal humerus fractures and can be a significant source of morbidity. The anterior and middle heads of the deltoid are separated by an avascular fibrous raphe.8,9 The course of the axillary nerve after it exits the quadrilateral space has been well described,10-16 but its position in relation to the raphe has only recently been reported.6 The anterior motor branch of the axillary nerve crosses the humerus transversely at variable distances as a single nerve and penetrates the fascia of the deltoid before or after dividing into several smaller branches.8,12 Duparc and colleagues11 found that in 12 of 32 shoulders (38%), the anterior trunk branched into smaller motor branches after entry into the anterior head of the deltoid, and in the remaining specimens the division occurred at variable distance prior to muscle entry. These investigators did not focus on the raphe specifically. Innervation of the deltoid is from the axillary nerve, which arises from the posterior cord of the brachial plexus and passes through the quadrilateral space dividing into anterior and posterior branches. The posterior branch sends several smaller branches to the teres minor, the deltoid, and the superior lateral brachial cutaneous nerve. The anterior motor branch courses around the neck of the humerus and passes medially on the anterior surface of the surgical neck to supply the middle and anterior deltoid heads. The locations of the intramuscular branches are variable and when the deltoid is split intramuscularly 2004 for more than several centimeters distally, denervation of the anterior head of the deltoid from disruption of these fibers invariably occurs. Division of the raphe distally may avoid these problems. It has been shown that several branches to the middle head from the main branch occur approximately 9.8 mm before crossing the raphe, the main anterior motor branch crosses the raphe as a single nerve, and the first branches from the main trunk to the anterior head arise approximately 8.5 mm after crossing the raphe.6 Thus, as the raphe is divided, as long as the main anterior motor trunk is protected, no other branches are at risk. The deltopectoral approach for exposure of the anterior and lateral shoulder region has been most commonly used for plating of the proximal humerus. However, accessing the lateral aspect of the proximal humerus using this approach requires extensive soft tissue dissection and retraction, as it is an indirect approach to the plating zone. This is less than ideal for internal fixation of proximal humerus fractures and it further jeopardizes the compromised blood supply to the head of the humerus and fracture fragments. It has been advised that any dissection lateral to the deltoid-pectoral interval in the distal direction be limited to three to five centimeters from the acromion to avoid injury to the axillary nerve.8,9,12,17,18 Recent data has shown that the anterior motor branch of the axillary nerve crosses the raphe at a predictable location relative to the acromion and greater tuberosity,6 which allows more direct access to the proximal humerus after protecting the axillary nerve. The incidence of avascular necrosis after closed reduction ranges from 3% to 14% in three-part fractures and up to 34% in four-part fractures.19 Surgical insult of the soft tissue envelope and direct manipulation of the fracture fragments with disruption of the consolidating callous further increase this risk and avascular necrosis may be as high as 37% following open reduction and internal fixation.20 The head of the humerus is perfused by branches of the anterior humeral circumflex, posterior humeral circumflex, suprascapular, thoracoacromial, and subscapular arteries. The anterior and posterior humeral circumflex vessels have branches that directly penetrate bone; other arteries contribute through anastamosis systems with the circumflex vessels. Gerber and associates21 reported that the anterior humeral circumflex artery was the only artery that could alone supply the entire humeral head and that the posterior humeral circumflex artery mainly supplied the greater tuberosity and a small area of the humeral head through interosseous anastamoses with branches of the anterior circumflex artery. The anterior circumflex humeral artery arises from the axillary artery about one centimeter distal to the inferior border of the pectoralis major and courses laterally along the inferior border of the subscapularis tendon. Its course places it at risk when a standard deltopectoral approach is used, Bulletin • Hospital for Joint Diseases A C Volume 62, Numbers 1 & 2 2004 21 B D Figure 4 A 64-year-old female with osteoporosis fell on her left side and sustained a comminuted proximal humeral fracture (A and B). An extended anterior acromial approach was used; the axillary nerve and vessels were isolated and length, alignment and rotation of the fracture were obtained. A locking plate was then applied (C), to which the tuberosities were sutured anatomically. A postoperative radiograph shows anatomic reduction (D). particularly with distorted anatomy in the setting of a fracture. The posterior humeral circumflex artery passes through the quadrilateral space with the axillary nerve. Both of these structures are readily visualized and protected using the anterolateral raphe-splitting approach, and there is no dissection medially near the course of the 22 Bulletin • Hospital for Joint Diseases Volume 62, Numbers 1 & 2 critical anterior humeral circumflex artery. The recent rise in popularity of using fixed-angle plate-screw constructs to provide biologic fixation has altered many surgeons’ approach to fracture management.1,22 These plating systems act as internal fixators and have the advantage of not requiring periosteal stripping or direct apposition of the plate onto bone. The focus is shifted from absolute mechanical rigidity to biological preservation.23,24 The plate can be inserted through a small incision remote to the fracture site, preserving the soft tissues and precluding the need for direct exposure of the fracture fragments. Because there is only point contact with bone and no friction is required between the plate and bone, these devices act as pure splints. No longer is a tight interface between the plate and bone required for stability, rather load is distributed evenly among all the bone-screw interfaces.25 Reduction of temporary cortical porosis by vascular preservation and improved mechanical stability without fragment compression are two of the key benefits of locked plating. This concept of flexible fixation has been shown to promote callus formation,1,26,27 and animal studies have revealed stronger bone after hardware removal as well as decreased complications, such as infection and stress shielding.27 As internal fixation concepts and techniques continue to evolve, the development of novel minimally-invasive surgical approaches is critical. The degree of soft tissue dissection inherent in the deltopectoral approach is counterproductive when attempting to adhere to the principles of biological fixation. This extended anterior acromial approach allows a limited surgical approach to be used, preserving the periosteum, and when coupled with locked plating, provides stable fixation to initiate indirect bone healing.28 These techniques may be particularly useful in osteoporotic proximal humerus fractures, where screw purchase may be suboptimal, and in unstable surgical neck fractures, which are inherently unstable (Fig. 4). Though further clinical study is warranted, use of this approach may decrease complications and improve outcomes in the operative treatment of proximal humerus fractures. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. References 1. 2. 3. 4. 5. Perren SM: Evolution of the internal fixation of long bone fractures: The scientific basis of biological internal fixation: Choosing a new balance between stability and biology. J Bone Joint Surg Br 84:1093-1110, 2002. Blevins FT, Warren RF, Cavo C, et al: Arthroscopic assisted rotator cuff repair: Results using a mini-open deltoid splitting approach. Arthroscopy 12:50-59, 1996. Norberg FB, Field LD, Savoie FH, III: Repair of the rotator cuff: Mini-open and arthroscopic repairs. Clin Sports Med 19:77-99, 2000. Pollock RG, Flatow EL: The rotator cuff: Full-thickness tears: Mini-open repair. Orthop Clin North Am 28:169-177, 1997. Yamaguchi K: Mini-open rotator cuff repair: An updated 21. 22. 23. 24. 2004 perspective. Instr Course Lect 50:53-61, 2001. Gardner MJ, Griffith MH, Dines JS, et al: The extended anterior acromial approach to the proximal humerus. In press, 2004. Iannotti JP, Ramsey ML, Williams GR, Warner JJP: Nonprosthetic management of proximal humerus fractures. J Bone Joint Surg Am 85:1578-1593, 2003. Burkhead WZ, Scheinberg RR, Box G: Surgical anatomy of the axillary nerve. J Shoulder Elbow Surg 1:31-36, 1992. Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics: The Anatomic Approach. Philadelphia: Lippincott Williams and Wilkins, 1994. Zhao X, Hung LK, Zhang GM, Lao J: Applied anatomy of the axillary nerve for selective neurotization of the deltoid muscle. Clin Orthop (390):244-251, 2001. Duparc F, Bocquet G, Simonet J, Freger P: Anatomical basis of the variable aspects of injuries of the axillary nerve (excluding the terminal branches in the deltoid muscle). Surg Radiol Anat 19:127-132, 1997. Kontakis GM, Steriopoulos K, Damilakis J, Michalodimitrakis E: The position of the axillary nerve in the deltoid muscle: A cadaveric study. Acta Orthop Scand 70:9-11, 1999. McFarland EG, Caicedo JC, Kim TK, Banchasuek P: Prevention of axillary nerve injury in anterior shoulder reconstructions: Use of a subscapularis muscle-splitting technique and a review of the literature. Am J Sports Med 30:601-606, 2002. Loomer R, Graham B: Anatomy of the axillary nerve and its relation to inferior capsular shift. Clin Orthop (243):100-105, 1989. Kulkarni RR, Nandedkar AN, Mysorekar VR: Position of the axillary nerve in the deltoid muscle. Anat Rec 232:316-317, 1992. Tubbs RS, Oakes WJ, Blount JP, et al: Surgical landmarks for the proximal portion of the axillary nerve. J Neurosurg 95:998-1000, 2001. Abbot LC, Saunders CM, Hagey H, Jones EW: Surgical approaches to the shoulder joint. J Bone Joint Surg Am 31:235255, 1949. Hollinshead W: Anatomy for Surgeons. New York: Harper and Row, 1982. Rees J, Hicks J, Ribbans W: Assessment and management of three- and four-part proximal humeral fractures. Clin Orthop (353):18-29, 1998. Wijgman AJ, Roolker W, Patt TW, Raaymakers EL, Marti RK: Open reduction and internal fixation of three and four-part fractures of the proximal part of the humerus. J Bone Joint Surg Am 84:1919-1925, 2002. Gerber C, Schneeberger AG, Vinh TS: The arterial vascularization of the humeral head: An anatomical study. J Bone Joint Surg Am 72:1486-1494, 1990. Lill H, Hepp P, Korner J, et al: Proximal humeral fractures: how stiff should an implant be? A comparative mechanical study with new implants in human specimens. Arch Orthop Trauma Surg 123:74-81, 2003. Perren SM: Evolution and rationale of locked internal fixator technology: Introductory remarks. Injury 32(Suppl 2):B3-B9, 2001. Hofer HP, Wildburger R, Szyszkowitz R: Observations concerning different patterns of bone healing using the Point Bulletin • Hospital for Joint Diseases Contact Fixator (PC-Fix) as a new technique for fracture fixation. Injury 32(Suppl 2):B15-B25, 2001. 25. el-Sayed A, Said HG, Abdel-Aal A, Farouk O: Locked plate fixation for femoral shaft fractures. Int Orthop 25:214-218, 2001. 26. Ilizarov GA: Clinical application of the tension-stress effect for limb lengthening. Clin Orthop (250):8-26, 1990. 27. Klaue K, Fengels I, Perren SM: Long-term effects of plate Volume 62, Numbers 1 & 2 2004 23 osteosynthesis: Comparison of four different plates. Injury 31(Suppl 2):B51-B62, 2000. 28. Hertel R, Eijer H, Meisser A, et al: Biomechanical and biological considerations relating to the clinical use of the Point Contact-Fixator: Evaluation of the device handling test in the treatment of diaphyseal fractures of the radius and/or ulna. Injury 32(Suppl 2):B10-B14, 2001.