Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Electrocardiography wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac surgery wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Atrial septal defect wikipedia , lookup
Atrial fibrillation wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
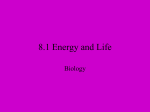
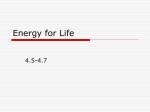
JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 ª 2015 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 2405-500X/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jacep.2015.02.020 Adenosine-Provoked Atrial Fibrillation Originating From Non–Pulmonary Vein Foci The Clinical Significance and Outcome After Catheter Ablation Akio Kuroi, MD, Shinsuke Miyazaki, MD, Eisuke Usui, MD, Noboru Ichihara, MD, Yoshihisa Kanaji, MD, Takamitsu Takagi, MD, Jin Iwasawa, MD, Hiroaki Nakamura, MD, Hiroshi Taniguchi, MD, Hitoshi Hachiya, MD, Yoshito Iesaka, MD JACC: CLINICAL ELECTROPHYSIOLOGY CME This article has been selected as the month’s JACC: Clinical Electrophysiology CME Objective: The existence and location of non-pulmonary vein foci CME activity, available online at www.jacc-electrophysiology.org by revealed by adenosine testing has a prognostic value in the clinical selecting the CME on the top navigation bar. outcome after pulmonary vein isolation for paroxysmal atrial fibrillation. Accreditation and Designation Statement CME Editor Disclosure: CME Editor Smit Vasaiwala, MD, has nothing The American College of Cardiology Foundation (ACCF) is accredited by to declare. the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Author Disclosures: This study was funded in part by grant 8P20GM103447 from the National Institute of General Medical Sciences to Dr. Stavrakis. The ACCF designates this Journal-based CME activity for a maximum The authors have reported that they have no relationships relevant to of 1 AMA PRA Category 1 Credit(s). Physicians should only claim credit the contents of this paper to disclose. commensurate with the extent of their participation in the activity. Medium of Participation: Print (article only); online (article and quiz). Method of Participation and Receipt of CME Certificate To obtain credit for JACC: Clinical Electrophysiology CME, you must: CME Term of Approval 1. Be an ACC member or JACC subscriber. Issue Date: June 2015 2. Carefully read the CME-designated article available online and in this Expiration Date: May 31, 2016 issue of the journal. 3. Answer the post-test questions. At least 2 out of the 3 questions provided must be answered correctly to obtain CME credit. 4. Complete a brief evaluation. 5. Claim your CME credit and receive your certificate electronically by following the instructions given at the conclusion of the activity. From the Cardiovascular Center, Tsuchiura Kyodo Hospital, Tsuchiura, Ibaraki, Japan. The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Manuscript received January 5, 2015; revised manuscript received February 23, 2015, accepted February 26, 2015. 128 Kuroi et al. JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 JUNE 2015:127–35 Non-PV Foci Revealed by an ATP Test Adenosine-Provoked Atrial Fibrillation Originating From Non–Pulmonary Vein Foci The Clinical Significance and Outcome After Catheter Ablation ABSTRACT OBJECTIVES The goal of this study was to systematically investigate the incidence and clinical significance of non–pulmonary vein (PV) foci revealed by adenosine/adenosine triphosphate (ATP) testing during atrial fibrillation (AF) ablation. BACKGROUND ATP is reported to provoke AF. METHODS A total of 464 patients with consecutive paroxysmal AF undergoing ATP testing after PV antrum isolation were included. RESULTS AF originating from non-PV foci was provoked in 26 (5.6%) total patients during first (n ¼ 20) or repeat (n ¼ 8) ablation procedures. Dormant PV conduction was also revealed by ATP testing in 6 patients. Non-PV foci were located in the superior vena cava (SVC) (i.e., the SVC group) and atria (i.e., the atria group) in 10 and 18 (9 each in the right and left atria) patients, respectively. In the multivariable analysis, being female was the sole independent predictor of ATP-provoked AF originating from non-PV foci (hazard ratio [HR]: 2.52 [95% confidence interval (CI): 1.069 to 5.929]; p ¼ 0.034). After additional ablation targeting non-PV foci, freedom from recurrent AF after the last procedure was similar between the SVC group and patients without ATP-provoked AF but was significantly lower in the atria group than in others (p ¼ 0.0008). Atria group membership (HR: 3.725 [95% CI: 1.692 to 8.199]; p ¼ 0.001) and being female (HR: 1.538 [95% CI: 1.189 to 1.989]; p ¼ 0.001) were significant independent predictors associated with recurrence after the last procedure in the multivariable Cox regression model. CONCLUSIONS ATP provoked AF originating from non-PV foci under isoproterenol in 5.6% of patients undergoing paroxysmal AF ablation. ATP testing might be useful for identifying and eliminating AF originating from the SVC. The atria group was associated with a poor outcome after the last procedure despite efforts to eliminate non-PV foci. (J Am Coll Cardiol EP 2015;1:127–35) © 2015 by the American College of Cardiology Foundation. R adiofrequency (RF) catheter ablation of atrial METHODS fibrillation (AF) is an established therapy for drug-resistant paroxysmal AF (1–3). In fact, STUDY POPULATION. The study consisted of 464 recent guidelines include catheter ablation as a first- consecutive patients who underwent ATP testing af- line therapy for specific groups of patients with AF ter a PVAI during the initial ablation procedure for (3). Pulmonary vein antrum isolation (PVAI) is the paroxysmal AF at our hospital. AF was classified ac- cornerstone of AF ablation procedures (3–6), and cording to the Heart Rhythm Society/European Heart non–pulmonary vein (PV) foci have been established Rhythm Association/European Cardiac Arrhythmia as important sources of AF (7). In general, identifying Association 2012 Consensus Statement on Catheter non-PV foci is challenging during procedures mainly and Surgical Ablation of AF (3). All patients provided due to the difficulty in provoking AF. The adenosine/ written informed consent. adenosine triphosphate (ATP) test is reportedly useful SEE PAGE 136 for identifying dormancy after PV isolation (8–10), and it can also provoke AF (11). However, little is known MAPPING about the clinical impact of ATP-provoked AF origi- rhythmic drugs were discontinued for at least 5 half- AND ABLATION PROTOCOL. Antiar- nating from non-PV foci in the context of AF ablation. lives before the procedure. Any atrial thrombi were The goal of the present study was to systematically excluded by using transesophageal echocardiogra- investigate the incidence and clinical significance of phy. The surface electrocardiogram and bipolar in- ATP-provoked AF originating from non-PV foci. tracardiac electrograms were continuously monitored Kuroi et al. JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 JUNE 2015:127–35 and the data stored on a computer-based digital activation sequence when AF occurred dur- ABBREVIATIONS recording system (LabSystem PRO, Bard Electro- ing the initial ATP test; 3) a 10-pole catheter AND ACRONYMS physiology, Lowell, Massachusetts). The bipolar was placed in the lateral RA; and 4) a map- electrograms were filtered from 30 to 500 Hz. A 7-F, ping catheter was used for ablation. Addi- 20-pole, 3-site mapping catheter (BeeAT, Japan Life- tional line Co., Ltd., Tokyo, Japan) was inserted through the eliminate non-PV foci immediately after the right jugular vein for pacing, recording, and internal reproducibility was confirmed. If subsequent GP = ganglionated plexus cardioversion. The 4 proximal electrodes, 8 middle ATP tests still induced AF, multielectrode HR = hazard ratio electrodes, and 8 distal electrodes were positioned in catheters were repositioned close to the foci LA = left atrium the superior vena cava (SVC), high right atrium (RA), to localize the non-PV foci, and additional RF PV = pulmonary vein and coronary sinus, respectively, throughout the applications were applied. During repeat PVAI = pulmonary vein procedure. The procedure was performed under procedures at the outset, the PVs were antrum isolation minimal sedation with pentazocine and hydroxyzine checked with a circumferential catheter, and RA = right atrium pamoate. RF applications were applied to AF = atrial fibrillation ATP = adenosine triphosphate CI = confidence interval any reconnected PVs were reisolated. ATP RF = radiofrequency The ablation was performed according to a strategy tests were undertaken with the same protocol SVC = superior vena cava described previously (12,13). In brief, after a trans- as during the index procedure even in cases septal puncture, pulmonary venography during ven- without any PV reconnections at baseline (14). When tricular pacing and contrast esophagography were an arrhythmogenic SVC was identified during the performed. Heparinized saline was infused to main- procedure (Figure 1), an electrical isolation was per- tain the activated clotting time at 250 to 350 s. Ipsi- formed. The ablation endpoint was elimination of all lateral PVs were circumferentially and extensively SVC potentials recorded on the mapping catheter (15). ablated by using a double-Lasso technique (Lasso, The cavotricuspid isthmus was also ablated to create Biosense Webster, Inc., Diamond Bar, California) bidirectional conduction block if common atrial guided by a 3-dimensional mapping system (CARTO 3, flutter was identified. Biosense Webster, Inc.). The endpoint was achievement of bidirectional conduction block between the left atrium (LA) and PVs. RF current was delivered point-by-point with a 3.5-mm externally irrigated tip quadripolar ablation catheter (THERMOCOOL, FOLLOW-UP. The patients underwent continuous, in- hospital electrocardiogram monitoring for 2 to 4 days after the procedure. The first outpatient clinic visit was 3 weeks’ post-procedure. Subsequent follow-up Biosense Webster, Inc.) with a power up to 35 W (limited to 20 W on the posterior wall close to the esophagus), a target temperature of #38 C, and an F I G U R E 1 Adenosine Triphosphate Provoked Atrial Fibrillation Originating From Superior Vena Cava irrigation rate of 30 ml/min. After completing the PVAI, a 30-mg bolus of ATP was injected from the right jugular vein at least twice to identify any non-PV foci and to unmask any dormant PV conduction with the administration of isoproterenol (increasing the heart rate by w10 to 20 beats/min from baseline) (10). Two circular mapping catheters were placed in the ipsilateral PVs during the ATP test, and the left and right PV pairs were observed individually. Any dormant conduction was eliminated by additional RF applications. If AF was initiated from non-PV foci by the ATP test, attempts were made to identify the site of the origin by observing the initial beats at the onset of the induced AF by using multielectrode catheters (Figure 1). Additional ATP tests were undertaken after the mapping catheters were repositioned as follows: 1) a Two circular mapping catheters were placed in the ipsilateral left pulmonary veins. After 20-pole mapping catheter was inserted from the the completion of the pulmonary vein antrum isolation, an adenosine/adenosine triphos- jugular vein to map the SVC, high RA, and coronary sinus; 2) a circular mapping catheter was placed in the left atrial appendage or septum close to the transseptal hole 129 Non-PV Foci Revealed by an ATP Test depending on the coronary sinus phate test was performed during sequential atrial (coronary sinus [CS]) and ventricular (right ventricular apex [RVA]) pacing. Atrial fibrillation was initiated from the superior vena cava (SVC) (red arrow) after atrioventricular block. LIPV ¼ left inferior pulmonary vein; LSPV ¼ left superior pulmonary vein. 130 Kuroi et al. JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 JUNE 2015:127–35 Non-PV Foci Revealed by an ATP Test visits consisted of clinical interviews, electrocardio- patients, and dormant PV conduction was revealed by grams, and 24-h Holter monitoring every 3 months at ATP testing in 164 (35.3%) during the initial proce- our cardiology clinic. No antiarrhythmic drugs were dure. Among the 464 first and 115 second ablation prescribed after the procedure. Patients with palpita- procedures, AF originating from non-PV foci was tions were encouraged to use patient-activated event provoked repeatedly by ATP injections in 20 (4.3 %) recorders for 30 consecutive days. For the detection of and 8 (6.9 %) patients, respectively. AF was provoked any asymptomatic events, an external loop recorder during both the first and second procedures in was used (SpiderFlash, Sorin Group, Clamart, France), 2 patients. Therefore, in total, ATP-provoked AF which enabled the automatic detection of any atrial originating from non-PV foci was observed in 26 tachyarrhythmia for 14 consecutive days (16). Recur- (5.6%) patients. AF was initiated from non-PV foci rence was defined according to the patient’s symp- spontaneously, during an isoproterenol infusion, and toms and/or if an arrhythmia lasting >30 s was after electrical cardioversion in 7, 3, and 2 other documented. patients, respectively. The clinical characteristics of STATISTICAL ANALYSIS. Continuous data are expressed as the mean SD for normally distributed variables or as the median (25th to 75th percentiles) for nonnormally distributed variables, and they were compared by using a Student t test or Mann-Whitney U test, respectively. Categorical variables were compared by using the chi-square test. All parameters with a significance of <0.2 in the univariable analysis were entered into a multiple logistic regression analysis. The multivariable Cox method was used to determine the predictors of recurrent arrhythmias. Variables whose univariable analyses had p values <0.05 were included in the multivariable Cox regression model. A Kaplan-Meier analysis was used to determine the percentage of patients free from recurrence. The difference in the arrhythmia-free survival was evaluated by using the log-rank test. The proportional hazards assumption was investigated graphically, with a test based on Schoenfeld residuals. The following variables were evaluated in association with being arrhythmia-free after the procedure: age, sex, body mass index, presence of structural heart disease, hypertension, left atrial diameter, left ventricular ejection fraction, CHADS 2 score (congestive heart failure, hypertension, age $75 years, diabetes mellitus [1 point for presence of each], and stroke/transient ischemic attack [2 points]), CHA 2DS2VASc (congestive heart failure, hypertension, age $75 years, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age 65 to 74 years, sex category score), pro–B-type natriuretic peptide level, high-sensitivity C-reactive protein level, estimated glomerular filtration rate, and ATP-provoked AF. A probability value of p < 0.05 indicated statistical significance. the patients with and without ATP-provoked AF are shown in Table 1. In the univariable analysis, a younger age, female sex, and higher glomerular filtration rate showed a trend toward being associated with ATP-provoked AF originating from non-PV foci. In the multivariable analysis, female sex (hazard ratio [HR]: 2.52 [95% confidence interval (CI): 1.069 to 5.929]; p ¼ 0.034) was the sole independent pre-procedural predictor of ATP-provoked AF originating from non-PV foci. RESPONSE TO THE ATP INJECTION DURING THE INITIAL PROCEDURE. Among the 20 patients in whom AF originating from non-PV foci was provoked by ATP injections during the initial procedure, AF terminated spontaneously at a median of 180 s (40 to 595 s) after initiation in 9 (45.0%) patients; it persisted and required electrical cardioversion to be terminated in the remaining 11 (55.0%) patients. Immediate recurrent AF after cardioversion was observed in 4 (20.0%) patients and was initiated from the SVC in all patients. AF was provoked before, during, and following the occurrence of AV block after ATP injections in 3 (15.0%), 16 (80.0%), and 1 (5.0%) patients, respectively. An AF trigger was identified in the SVC, RA, and LA in 9 (45.0%), 5 (25.0%), and 6 (30.0%) patients, respectively (Figure 2). In patients with AF originating from the SVC, an electrical SVC isolation was successfully achieved in all patients. In 11 (55.0%) patients with AF originating from the atria, focal ablation targeting the non-PV foci was added, and a subsequent repeat ATP test did not provoke any AF except in 1 patient. A transient PV reconnection was observed according to an ATP test in 6 (30.0%) patients at the right-sided, left-sided, and bilateral ipsilateral PVs in 1, 3, and 2 patients, respectively. These transient PV reconnec- RESULTS tions did not lead to the initiation of AF. PREVALENCE AND CLINICAL CHARACTERISTICS. A patients were free from any recurrent arrhythmias successful PVAI was achieved in all 464 study without any antiarrhythmic drugs at 1 year. There was After the initial ablation procedure, 55.3% of the Kuroi et al. JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 JUNE 2015:127–35 Non-PV Foci Revealed by an ATP Test T A B L E 1 Clinical Characteristics of Patients With and Without ATP-Provoked AF ATP-AF (þ) (n ¼ 26 [5.6%)] ATP-AF (–) (n ¼ 438 [94.4%]) Univariable p Value Multivariable p Value Age, yrs 58.7 12.8 62.6 10.8 0.083 0.136 Female 11 (42.3) 121 (27.6) 0.107 0.034 1 (3.9) 50 (11.4) 0.231 SHD Hypertension 15 (57.7) 251 (57.3) HR 95% CI 2.52 1.069–5.929 0.969 Body mass index, kg/m2 24.0 3.8 24.3 3.7 CHADS2 score 0.73 0.96 0.79 0.93 0.745 CHA2DS2-VASc score 1.54 1.58 1.58 1.38 0.889 LA diameter, mm 39.9 5.5 40.3 5.8 0.724 LV ejection fraction, % 65.5 9.0 66.5 7.0 0.476 proBNP, pg/ml 270 356 hs-CRP, mg/dl 0.17 0.28 0.24 0.81 0.662 Estimated GFR, ml/min 77.3 17.8 71.1 19.4 0.114 0.692 332 1,033 0.801 0.393 Values are mean SD or n (%). AF ¼ atrial fibrillation; ATP ¼ adenosine triphosphate; CHADS2 score ¼ congestive heart failure, hypertension, age $75 years, diabetes mellitus (1 point for presence of each), and stroke/transient ischemic attack (2 points); CHA2DS2-VASc score ¼ congestive heart failure, hypertension, age $75 years, diabetes mellitus, stroke/transient ischemic attack, vascular disease, age 65 to 74 years, sex category; CI ¼ confidence interval; GFR ¼ glomerular filtration rate; HR ¼ hazard ratio; hs-CRP ¼ high-sensitivity C-reactive protein; LA ¼ left atrium; LV ¼ left ventricular; proBNP ¼ pro–B-type natriuretic peptide; SHD ¼ structural heart disease. no significant difference in the freedom from recur- whom AF was provoked by an ATP injection during rent arrhythmias after the initial procedure between the second procedure, AF terminated spontaneously the patients with and without ATP-provoked AF at a median of 75 s (30 to 300 s) after the initiation in 4 (p ¼ 0.61) (Figure 3). (50.0%) patients; it persisted and required electrical RESPONSE TO THE ATP INJECTION DURING THE REPEAT PROCEDURE. Among 115 patients undergo- ing a second procedure, PV reconnections were observed in 98 (85.2%) patients. Among 8 patients in cardioversion to terminate it in the remaining 4 (50.0%) patients. Immediate recurrent AF after cardioversion was observed in 3 (37.5%) patients, and AF initiated from the SVC, RA, and LA in 1 each. AF was provoked during AV block after an ATP injection in all patients. An AF trigger was identified in the SVC, RA, and LA in 1 (12.5%), 4 (50.0%), and 3 (37.5%) patients, F I G U R E 2 Distribution of the Origins of ATP-Provoked AF respectively (Figure 2). In the patient with AF originating from the SVC, an electrical SVC isolation was successfully achieved. In 7 patients with AF originating from the atria, focal ablation targeting the non-PV foci eliminated the ATP-provoked AF in 5 (62.5%) but not in 3 (37.5%) patients. No PV reconnections were provoked in any of the patients with the ATP test. After the second procedure, 50% of the patients were free from recurrent arrhythmias without any antiarrhythmic drugs at 1 year. Among the 4 patients with recurrent arrhythmias, the ATP-provoked AF was eliminated in 2 but not in the remaining 2 patients. CLINICAL OUTCOME IN PATIENTS WITH ATP-PROVOKED AF ORIGINATING FROM NON-PV FOCI. In all 26 paNon–pulmonary vein foci were identified along the crista terminalis (CT), septum, and close to the distal CS. AF ¼ atrial fibrillation; ATP ¼ adenosine triphosphate test; IVC ¼ inferior vena cava; PW ¼ posterior wall; RIPV ¼ right inferior pulmonary vein; RSPV ¼ right superior pulmonary vein; other abbreviations as in Figure 1. tients, the reproducibility of ATP-provoked AF was confirmed, and a mean of 4.0 3.2 APT tests per procedure were performed. No multiple non-PV foci were observed in any patients. Freedom from recurrent AF after the last procedure was significantly lower in the 26 patients with ATP-provoked AF 131 132 Kuroi et al. JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 JUNE 2015:127–35 Non-PV Foci Revealed by an ATP Test F I G U R E 3 Freedom From Recurrent AF After a Single Procedure Freedom from recurrent arrhythmias after a single ablation procedure in patients with and without ATP-provoked AF originating from non–pulmonary vein foci during the initial procedure. Abbreviations as in Figure 2. originating from non-PV foci during either the initial after the last procedure in the multivariable Cox or second procedure compared with those without regression model. (p ¼ 0.002) (Figure 4A). However, when the patients with ATP-provoked AF were divided into 2 groups, including patients with AF originating from the SVC (i.e., the SVC group) and those with AF originating from the atria (i.e., the atria group), the freedom from recurrent AF after the last procedure was significantly lower in the atria group but similar in the SVC group compared with patients without ATP-provoked AF (p ¼ 0.0008) (Figure 4B). An increased age, higher CHA2DS2 -VASc score, being female, and ATP-provoked AF originating from non-PV foci were correlated with a recurrence after the last procedure as identified by the univariable analysis, and being female (HR: 1.538 [95% CI: 1.189 to 1.989]; p ¼ 0.001) and ATP-provoked AF originating from non-PV foci (HR: 3.328 [95% CI: 1.632 to 6.783]; p ¼ 0.001) were the significant factors in the multivariable Cox regression model DISCUSSION MAJOR FINDINGS. First, the ATP test under an isoproterenol infusion provoked AF originating from non-PV foci in 5.6% of patients undergoing paroxysmal AF ablation. Second, being female was the sole independent predictor of ATP-provoked AF originating from non-PV foci. Third, the SVC was the important source (38.2%) of non-PV foci, revealed by results of the ATP test, which can aid in the identification of an arrhythmogenic SVC during the procedure. Fourth, ATP-provoked AF originating from the atria was the independent predictor associated with a recurrence of arrhythmia after the last procedure. ADENOSINE/ATP TEST IN THE CONTEXT OF AF (Table 2). Further analysis revealed that the atria ABLATION. The adenosine/ATP test has been used group was significantly associated with a recurrence for the identification of the dormancy during the after the last procedure (HR: 3.725 [95% CI: 1.692 to initial procedure after electrical isolation (8–10). A 8.199]; p ¼ 0.001), but the SVC group was not prospective study is ongoing to investigate the clin- (p ¼ 0.247). Similarly, when analyzing the 115 pa- ical implications of targeting dormant PVs by addi- tients undergoing repeat procedures, being female tional ablation (17). Datino et al. (18) showed that (HR: 2.595 [95% CI: 1.095 to 6.147]; p ¼ 0.030) and adenosine acutely restores the PV–LA conduction by ATP-provoked AF originating from non-PV foci hyperpolarizing the PV cells and thereby enhancing (HR: 3.324 [95% CI: 1.284 to 8.603]; p ¼ 0.013) were the Naþ current availability. A similar dormancy was the significant factors associated with recurrence also reported in PVs during the chronic phase after Kuroi et al. JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 JUNE 2015:127–35 133 Non-PV Foci Revealed by an ATP Test F I G U R E 4 Freedom From Recurrent AF After the Last Procedure (A) Freedom from recurrent arrhythmias after the last ablation procedure in patients with and without ATP-provoked AF originating from non– pulmonary vein foci. (B) Freedom from recurrent arrhythmias after the last ablation procedure in patients with ATP-provoked AF originating from the SVC, those with ATP-provoked AF originating from the atria, and those without ATP-provoked AF. Abbreviations as in Figures 1 and 2. the isolation (14), at the cavotricuspid isthmus, after This finding might be explained by the difficulty in achievement of linear conduction block (19), and in identifying the precise foci from a single earliest beat the SVC after isolation (20), presumably with a similar by using conventional mapping techniques and the mechanism. low reproducibility of AF induction by the ATP test. The ATP test is also useful for provoking AF Among the 8 patients in whom AF was provoked by during the procedure. Isoproterenol is widely used the ATP test during the second procedure, 6 patients to identify AF triggers, and it usually provokes did not have any ATP-provoked AF during the initial catecholamine-dependent arrhythmias. In the pre- procedure, presumably due to the variable autonomic sent study, additional ATP injections were used to tone during the time course and the impact of the identify non-PV foci. Recently, Tao et al. (21) reported PVAI on the autonomic tone. Recently, Zhang et al. that the ATP test facilitated the identification of arrhythmogenic PVs in patients with paroxysmal AF undergoing ablation. They showed that the majority T A B L E 2 Factors Associated With Recurrent Arrhythmias After the Last Procedure of ATP-induced AF originated from the PVs. In Univariable p Value contrast, ATP tests were undertaken after the PVAI in our large consecutive series, and the prevalence of Age, yrs ATP-provoked AF originating from non-PV foci was Female 5.6% with isoproterenol infusions. SHD The identification of an arrhythmogenic SVC is 0.001 <0.001 Hypertension 0.513 Body mass index, kg/m2 0.200 ing an established effective therapy (22). In our se- CHADS2 score ries, the SVC was the important source of non-PV foci revealed by ATP, and the ATP test aided in the 95% CI Multivariable p Value 1.043 1.017–1.070 0.124 3.039 1.906–4.843 0.001 1.348 1.162–1.564 0.417 2.802 1.392–5.643 0.001 LA diameter, mm 0.154 LV ejection fraction, % 0.840 proBNP, pg/ml 0.323 clinical outcome can be expected in cases with an hs-CRP, mg/dl 0.065 arrhythmogenic SVC because the complete elimina- Estimated GFR, ml/min 0.581 tion of the trigger is relatively easy by electrical ATP-AF 0.004 isolation. In fact, the clinical outcome after the last ATP-AF from SVC 0.247 procedure was similar in the SVC group and in those ATP-AF from atrium 0.001 outcome was significantly poorer in the atria group. 95% CI 1.538 1.189–1.989 0.057 <0.001 identification of the arrhythmogenicity. A better without ATP-provoked AF. Conversely, the clinical HR 0.645 generally challenging despite electrical isolation be- CHA2DS2-VASc score HR SVC ¼ superior vena cava; other abbreviations as in Table 1. 3.328 1.632–6.783 3.725 1.692–8.199 134 Kuroi et al. JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 JUNE 2015:127–35 Non-PV Foci Revealed by an ATP Test (23) reported that 13% of ATP-induced non-PV foci STUDY LIMITATIONS. First, the study used a ret- were observed after PVAI. Their reported prevalence rospective of ATP-provoked non-PV foci was considerably although non-PV foci were localized by using a higher than in the present study, presumably due to number of multielectrode catheters, identification of the different study population. The majority of their precise non-PV foci is challenging because of the lack study population were women (52% female) and of a single-beat mapping system. Third, the pure the age was younger (mean 57.4 years) than in impact of an ATP injection on non-PV foci could not our study. Our study has shown that being female be evaluated because the ATP test was undertaken was an independent predictor of ATP-induced non- under an isoproterenol infusion. The utility of the PV foci and that the location of the non-PV foci was ATP test should be evaluated and compared with strongly associated with the clinical outcome after other approaches for identifying non-PV foci, such as the last procedure, which seems to be clinically isoproterenol infusions, in a prospective clinical trial. significant. Fourth, the ATP test was not undertaken before the and nonrandomized design. Second, PVAI, and thus the impact on the PVs was not MECHANISMS OF ATP-PROVOKED AF. Adenosine is evaluated. a purine nucleoside closely related to adenosine5 0 -triphosphate, which is important in multiple CONCLUSIONS biochemical processes (24). Both exert transient negative chronotropic and dromotropic responses on An ATP injection under an isoproterenol infusion the sinoatrial and atrioventricular nodes. It is well provoked AF originating from non-PV foci in 5.6% of known that adenosine can induce AF in clinical patients undergoing paroxysmal AF ablation. The SVC practice (11), and previous studies have postulated was the origin of 38.5% of the non-PV foci revealed by that shortening of atrial action potential duration is ATP, which aides in identifying an arrhythmogenic the principal mechanism of adenosine-induced AF SVC. ATP-provoked AF originating from the atria is a (25). In addition, adenosine has sympathoexcitatory significant independent predictor associated with effects mediated through a baroreflex activation and recurrent arrhythmias after the last procedure. chemoreceptor stimulation (26). ACKNOWLEDGMENT The authors thank Mr. John Another hypothesis is the activation of the Martin for the preparation of the manuscript. autonomic nervous system via the ganglionated plexus (GP). An injection of acetylcholine into the REPRINT REQUESTS AND CORRESPONDENCE: Dr. GP at the PV–LA junction has been shown to acutely Shinsuke Miyazaki, Cardiology Division, Cardio- result in the induction of spontaneous PV ectopy vascular Center, Tsuchiura Kyodo Hospital, 11-7 (27). The preferential role of the SVC–aorta GP in Manabeshin-machi, modulating the electrophysiological function of the Japan. E-mail: [email protected]. Tsuchiura, Ibaraki 300-0053, SVC sleeves in canines has also been shown (28). Adenosine and acetylcholine act on identical receptor pathways to induce antiadrenergic effects, and hyperactivity of the SVC–aorta GP induced by direct injection of acetylcholine can lead to rapid firing from the SVC. Thus, adenosine can trigger vagally mediated AF. The reason why ATP-provoked AF was identified more frequently in female patients is unclear from the present data. Previous large studies showed that the outcome after AF ablation was worse for female patients and speculated that non-PV foci were one of the causes of a higher recurrence rate (29,30). Differences in sex in cardiac autonomic regulation are well known (31). Given that an ATP injection has a strong influence on autonomic tone, it is possible that the impact of ATP on the arrhythmia inducibility has sex differences and that residual non-PV foci after PVAI are revealed more frequently in female patients. PERSPECTIVES COMPENTENCY IN MEDICAL KNOWLEGDE: Adenosine injection provoked AF originating from non-PV foci in 5.6% of patients undergoing paroxysmal AF ablation. The SVC was the origin of 38.5% of the non-PV foci revealed by adenosine, which aids in identifying an arrhythmogenic SVC. Moreover, adenosine-provoked AF originating from the atria was a significant independent predictor associated with recurrent arrhythmias after the last procedure. TRANSLATIONAL OUTLOOK: The utility of the adenosine test should be evaluated and compared with other approaches for identifying non-PV foci, such as isoproterenol infusions, in a prospective clinical trial. Kuroi et al. JACC: CLINICAL ELECTROPHYSIOLOGY VOL. 1, NO. 3, 2015 JUNE 2015:127–35 Non-PV Foci Revealed by an ATP Test REFERENCES 1. Haïssaguerre M, Jaïs P, Shah DC, et al. Electrophysiological end point for catheter ablation of atrial fibrillation initiated from multiple pulmonary venous foci. Circulation 2000;101:1409–17. 9. Tritto M, De Ponti R, Salerno-Uriarte JA, et al. Adenosine restores atrio-venous conduction after apparently successful ostial isolation of the pulmonary veins. Eur Heart J 2004;25:2155–63. 2. Nault I, Miyazaki S, Forclaz A, et al. Drugs vs. 10. Hachiya H, Hirao K, Takahashi A, et al. Clinical implications of reconnection between the left ablation for the treatment of atrial fibrillation: the evidence supporting catheter ablation. Eur Heart J 2010;31:1046–54. 3. Calkins H, Kuck KH, Cappato R, et al., Heart Rhythm Society Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. 2012 HRS/ EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA), a registered branch of the European Society of Cardiology (ESC) and the European Cardiac Arrhythmia Society (ECAS); and in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), the Asia Pacific Heart Rhythm Society (APHRS), and the Society of Thoracic Surgeons (STS). Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Heart Rhythm 2012;9:632–96. atrium and isolated pulmonary veins provoked by adenosine triphosphate after extensive encircling pulmonary vein isolation. J Cardiovasc Electrophysiol 2007;18:1–7. 11. Belhassen B, Pelleg A. Electrophysiologic effects of adenosine triphosphate and adenosine on the mammalian heart: clinical and experimental aspects. J Am Coll Cardiol 1984;4:414–24. 12. Miyazaki S, Kuwahara T, Kobori A, et al. Long-term clinical outcome of extensive pulmonary vein isolation-based catheter ablation therapy in patients with paroxysmal and persistent atrial fibrillation. Heart 2011;9:668–73. 13. Uchiyama T, Miyazaki S, Taniguchi H, et al. Six-year follow-up of catheter ablation in paroxysmal atrial fibrillation. Circ J 2013;77:2722–7. 14. Miyazaki S, Kobori A, Komatsu Y, et al. Clinical implication of adenosine test at repeat atrial fibrillation ablation procedure: the importance of detecting dormant thoracic vein conduction. Circ Arrhythm Electrophysiol 2012;5:1117–23. 15. Miyazaki S, Usui E, Kusa S, et al. Prevalence and clinical outcome of phrenic nerve injury during superior vena cava isolation and circumferential pulmonary vein antrum isolation using radiofrequency energy. Am Heart J 2014;168:846–53. 4. Takahashi A, Iesaka Y, Takahashi Y, et al. Electrical connections between pulmonary veins: implication for ostial ablation of pulmonary veins in patients with paroxysmal atrial fibrillation. Circulation 2002;105:2998–3003. 16. Takagi T, Miyazaki S, Kusa S, et al. Role of 5. Arentz T, Weber R, Bürkle G, et al. Small and large isolation areas around the pulmonary veins for treatment of atrial fibrillation? Results from a prospective randomized study. Circulation 2007; 115:3057–63. 17. Macle L, Khairy P, Verma A, et al., ADVICE Study Investigators. Adenosine following pulmo- 6. Liu X, Dong J, Mavrakis HE, et al. Achievement of pulmonary vein isolation in patients undergoing circumferential pulmonary vein ablation: a randomized comparison between two different 18. Datino T, Macle L, Qi XY, et al. Mechanisms by which adenosine restores conduction in dormant isolation approaches. J Cardiovasc Electrophysiol 2006;17:1263–70. 19. Lehrmann H, Weber R, Park CI, et al. “Dormant transisthmus conduction” revealed by adenosine after cavotricuspid isthmus ablation. Heart Rhythm 2012;9:1942–6. 7. Shah D, Haissaguerre M, Jais P, Hocini M. Nonpulmonary vein foci: do they exist? Pacing Clin Electrophysiol 2003;26:1631–5. 8. Arentz T, Macle L, Kalusche D, et al. “Dormant” pulmonary vein conduction revealed by adenosine alter ostial radiofrequency catheter ablation. J Cardiovasc Electrophysiol 2004;15:1041–7. extended external auto-triggered loop recorder monitoring for atrial fibrillation: validation and utility after catheter ablation procedures. Circ J 2014;78:2637–42. nary vein isolation to target dormant conduction elimination (ADVICE): methods and rationale. Can J Cardiol 2012;28:184–90. canine pulmonary veins. Circulation 2010;121: 963–72. 20. Miyazaki S, Taniguchi H, Komatsu Y, et al. Clinical impact of adenosine triphosphate injection on arrhythmogenic superior vena cava in the context of atrial fibrillation ablation. Circ Arrhythm Electrophysiol 2013;6:497–503. 21. Tao S, Yamauchi Y, Maeda S, et al. Adenosine triphosphate-induced atrial fibrillation: the clinical significance and relevance to spontaneous atrial fibrillation. J Interv Card Electrophysiol 2014;39: 103–9. 22. Goya M, Ouyang F, Ernst S, Volkmer M, Antz M, Kuck KH. Electroanatomic mapping and catheter ablation of breakthroughs from the right atrium to the superior vena cava in patients with atrial fibrillation. Circulation 2002;106:1317–20. 23. Zhang J, Tang C, Zhang Y, Su X. Origin and ablation of the adenosine triphosphate induced atrial fibrillation after circumferential pulmonary vein isolation: effects on procedural success rate. J Cardiovasc Electrophysiol 2014;25:364–70. 24. Lerman BB, Belardinelli L. Cardiac electrophysiology of adenosine. Basic and clinical concepts. Circulation 1991;83:1499–509. 25. Kabell G, Buchanan LV, Gibson JK, Belardinelli L. Effects of adenosine on atrial refractoriness and arrhythmias. Cardiovasc Res 1994;28:1385–9. 26. Biaggioni I, Killian TJ, Mosqueda-Garcia R, Robertson RM, Robertson D. Adenosine increases sympathetic nerve traffic in humans. Circulation 1991;83:1668–75. 27. Scherlag BJ, Yamanashi W, Patel U, Lazzara R, Jackman WM. Autonomically induced conversion of pulmonary vein focal firing into atrial fibrillation. J Am Coll Cardiol 2005;45:1878–86. 28. Lu Z, Scherlag BJ, Niu G, et al. Functional properties of the superior vena cava (SVC)-aorta ganglionated plexus: evidence suggesting an autonomic basis for rapid SVC firing. J Cardiovasc Electrophysiol 2010;21:1392–9. 29. Patel D, Mohanty P, Di Biase L, et al. Outcomes and complications of catheter ablation for atrial fibrillation in females. Heart Rhythm 2010;7:167–72. 30. Takigawa M, Kuwahara T, Takahashi A, et al. Differences in catheter ablation of paroxysmal atrial fibrillation between males and females. Int J Cardiol 2013;168:1984–91. 31. Huikuri HV, Pikkujämsä SM, Airaksinen KE, et al. Sex-related differences in autonomic modulation of heart rate in middle-aged subjects. Circulation 1996;94:122–5. KEY WORDS adenosine, adenosine triphosphate, atrial fibrillation, catheter ablation, non–pulmonary vein foci Go to http://cme.jaccjournals.org to take the CME quiz for this article. 135