Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
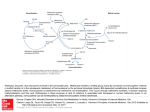
Clinical Chemistry 45, No. 2, 1999 315 Fig. 1. Difference plot with (y 2 x) as a function of (x 1 y)/2 (left) and x 2 y plot (right) with estimated Deming regression line (——) and diagonal y 5 x (zzzzzz). tematic constant difference (intercept different from zero) and a systematic proportional difference (slope different from 1). Therefore, the paired t-test should not be applied uncritically to method comparison data. Only when the graphical display suggests that a systematic constant difference, but not a systematic proportional difference, is involved should this test be applied. With this background, it appears surprising that a clinical chemistry journal has directly prohibited the use of regression analysis in method comparison studies, a point of view also expressed in another journal (7, 8 ). Opposition against this practice has previously been put forward (9 ). References 1. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;i:307–10. 2. Pollock MA, Jefferson SG, Kane JW, Lomax K, MacKinnon G, Winnard CB. Method comparison—a different approach. Ann Clin Biochem 1992;29:556 – 60. 3. Petersen PH, Stöckl D, Blaabjerg O, Pedersen B, Birkemose E, Thienpont L, et al. Graphical interpretation of analytical data from comparison of a field method with a reference method by use of difference plots. Clin Chem 1997;43: 2039 – 46. 4. Westgard JO, Hunt MR. Use and interpretation of common statistical tests in method comparison studies. Clin Chem 1973;19:49 –57. 5. Westgard JO, deVos D, Hunt MR, Quam EF, Carey RN, Garber CC. Concepts and practices in the evaluation of clinical chemistry methods. Part III. Statistics. Am J Med Technol 1978;44: 552–70. 6. Linnet K. Performance of Deming regression analysis in case of misspecified analytical error ratio in method comparison studies. Clin Chem 1998;44:1024 –31. 7. Hollis S. Analysis of method comparison studies [Editorial]. Ann Clin Biochem 1996;33:1– 4. 8. Hollis S. Analysis of method comparison studies. JIFCC 1997;9:8 –12. 9. Stöckl D. Beyond the myths of difference plots [Letter]. Ann Clin Biochem 1996;36:575–7. Kristian Linnet Laboratory of Clinical Biochemistry Psychiatric University Hospital DK-8240 Risskov, Denmark E-mail [email protected] Interlaboratory Variability for Total Homocysteine Analysis in Plasma To the Editor: Total plasma homocysteine consists of free homocysteine and homocysteine that is complexed with itself or with other amino acids or proteins. Free homocysteine has been measured previously as part of a biochemical screen for inherited metabolic disorders. More recently, increased total plasma homocysteine has been suggested as an independent risk factor for atherosclerotic coronary artery disease [reviewed in Ref. (1 )]. In addition, increased total homocysteine is associated with a poor prognosis in patients with angiographically demonstrated coronary artery disease (2 ). These studies have prompted clinicians to include total homocysteine analysis as part of the risk assessment profile of patients with premature coronary artery disease. However, it has yet to be shown that reducing total plasma homocysteine concentration leads to a decrease in cardiovascular risk, although vitamin supplementation may effectively lower or normalize circulating homocysteine concentrations (3 ). From a laboratory standpoint, problems exist in homocysteine analysis. External quality-assurance programs for total homocysteine (proficiency testing) are not available at present, and interlaboratory correlations of total homocysteine measurements have not been evaluated formally. We have contacted many of the reference laboratories in the US that offer this assay and have found that the reference ranges vary considerably between laboratories. Although most laboratories offer reference intervals based on in-house studies, a few base reference intervals on a review of the literature. Other laboratories offer a “target range” based on prospective studies, which correlate total homocysteine concentrations with risk for cardiovascular disease or with mortality (2). To evaluate laboratory variability of total homocysteine analysis, we sent five samples of frozen plasma in EDTA tubes, all drawn and pooled from the same fasting subject, to five different reference laboratories. The analytical variation of the results produced a wide range of possible risk estimates for that subject (Table 1). We evaluated the extent of variability attributable to inherent test imprecision as opposed to bias between laboratories. The variance of the reported homocysteine test results is composed of the sum of variance within the laboratories and variance between laboratories. To estimate variance within the laboratories, we obtained the coefficients of 316 Letters Table 1. Test results and risk assessment for total homocysteine in a specimen that has been aliquoted and sent to five reference laboratories. Reference laboratory Test result, mmol/L Reference or target range, mmol/L Test result/median of reference interval Study A mortality ratioa Study B relative riskb A B C D E 13.5 11.8 11.0 10.1 8.7 4.9–14.6c 8.0–12.0c 4–17c 6.4–13.7c ,7.2d 1.4 1.2 1.0 1.0 1.1 0.9 0.8 0.75 0.7 3.0 1.5 1.0 1.9 0.8 a Relative risk of mortality in patients with angiographically confirmed coronary artery disease during a follow-up period of ;4 years. Mortality ratios were estimated from Fig. 2 in Nygard et al. (2). b Relative risk of vascular disease at the time of homocysteine testing. The relative risk was derived from Fig. 4 in Graham et al. (4). c Reference range. d Target range described by Nygard et al. (2). variation (CVs) for homocysteine testing from the five reference laboratories. At homocysteine concentrations ranging from 8 to 15 mmol/L, the participating laboratories reported CVs of 4.9 –11%. The variances of homocysteine test results within each reference laboratory were estimated to be between 0.44 and 1.46 (mmol/L)2, with an average variance of 0.96 (mmol/L)2. By subtracting the average variance within laboratories from the total variance of 3.25 (mmol/L)2, we found the variance between laboratories to be 2.29 (mmol/L)2. Thus, bias between the laboratories contributed more than random error to the observed variability. Multiple factors could account for the interlaboratory variability, including different methodologies (most common methods are based on fluorescence polarization immunoassays and HPLC), different approaches to test calibration, lack of availability of reference materials for the various forms of homocysteine, or varying efficiencies for the dissociation of homocysteinecontaining complexes. The observed variability makes it difficult to interpret the laboratory result in terms of patient risk for development or progression of cardiovascular disease. References 1. Welch GN, Loscalzo J. Homocysteine and atherothrombosis. N Engl J Med 1998;338: 1042–50. 2. Nygard O, Nordrehaug JE, Refsum H, Ueland PM, Farstad M, Vollset SE. Plasma homocysteine levels and mortality in patients with coronary artery disease. N Engl J Med 1997;337: 230 – 6. 3. Malinow MR, Duell PB, Hess DL, Anderson PH, Kruger WD, Phillipson BE, et al. Reduction of plasma homocysteine levels by breakfast cereal fortified with folic acid in patients with coronary artery disease. N Engl J Med 1998; 338:1009 –15. 4. Graham IM, Daly LE, Refsum HM, Robinson K, Brattstrom LE, Ueland PM, et al. Plasma homocysteine as a risk factor for vascular disease. The European Concerted Action project. JAMA 1997;277:1775– 81. Stephen C. Eliason1 Detlef Ritter1,2* Hyung D. Chung1,2 Michael Creer1 1 Department of Pathology Saint Louis University School of Medicine St. Louis, MO 63104 2 Pathology and Laboratory Medical Service John Cochran Veterans Affairs Medical Center St. Louis, MO 63106 *Address correspondence to this author at: Clinical Laboratories, 3635 Vista at Grand, St. Louis, MO 63110-0250. Fax 314-289-7073; e-mail [email protected]. Urinary Free Cortisol Is Not Affected by Short-term Water Diuresis To the Editor: Urinary free cortisol (UFC) has been shown to be a reliable measure of adrenocortical secretion, and it is generally accepted as being an index of the free fraction in the plasma. However, the interpretation of UFC results reportedly can be compromised when the urine volume in patients is considerably increased because a high fluid intake (5 L/day) increases UFC in healthy subjects (1 ) and UFC was reported to be closely related with the changes in urine volume in women (2 ). The aim of this work was to determine whether short-term changes in urine volume influence UFC. I studied 15 volunteers (6 women and 9 men) with normal body mass indexes (23.9 6 1.9 kg/m2) and ages from 23 to 52 years. Informed consent was obtained from all volunteers and our institution’s responsible committee. Subjects were asked to empty their bladders at 0900 and to collect urine samples at 30-min intervals. At 1000, 10 of the volunteers (6 women and 4 men) were asked to drink 1 L of water within 5 min. The volume of each urine sample was measured and adjusted to a final volume of 300 mL. Urine samples with a volume .300 mL were not diluted. Creatinine and cortisol were measured by a colorimetric method (3 ) or by RIA (4 ). The results are presented as mean 6 SE. Statistical comparisons were made using the Mann–Whitney U-test for unpaired data. As expected, the urine volume was significantly greater during water diuresis (P ,0.002, 60 –180 min after water ingestion) than during the control period (0 –180 min, no water ingested). In contrast, neither urinary excretion of creatinine nor of UFC changed significantly (Fig. 1). A similar lack of change of UFC was found when cortisol concentrations in 40 of the samples were measured again by