Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
MTOR inhibitors wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Discovery and development of neuraminidase inhibitors wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Discovery and development of integrase inhibitors wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Clinical Cancer Research 227
Vol. 2, 227-243, February 1996
Minireview
Thymidylate Synthase Inhibitors
Nikolaos Touroutoglou and Richard Pazdur 1
Division of Medicine, The University of Texas M. D. Anderson
Cancer Center, Houston, Texas 77030
Abstract
Folate analogues that inhibit thymidylate synthase (TS)
selectively were developed based on TS and folate molecular
structures and properties. The structure-activity relationship, preclinical and clinical development, and issues of
potential importance in the future success of these TS inhibitors are reviewed herein. Properties of these new compounds depend mainly on the use of the reduced folate
carrier (RFC) proteins for cellular entry and on intracellular polyglutamation, which augments TS inhibitory function
and cellular retention. CB3717 [Zeneca (formerly ICI Pharmaceuticals), Macclesfield, United Kingdom], the first selective TS inhibitor developed, demonstrated antineoplastic
activity in Phase I trials, but its development was abandoned
due to nephrotoxicity. ZD1694 (Tomudex; Zeneca), a watersoluble, nonnephrotoxic quinazoline, demonstrated activity
in colorectal, breast, and pancreatic cancer. Phase III trials
of Tomudex in advanced colorectal cancer were completed
recently. LY231514 (Eli Lilly Research Labs, Indianapolis,
IN) uses the RFC and polyglutamation to exert its selective
TS inhibitory action. Phase I trials of this compound have
been completed. ZD9331 (Zeneca), currently in preclinical
studies, was designed to obviate the use of the RFC for
cellular entry. 1843U89 (Glaxo-Wellcome, Research Triangle Park, NC), currently in Phase I trial, does not require the
RFC; polyglutamation of this potent TS inhibitor leads to its
higher cellular retention without augmenting its TS inhibitory activity. Currently in clinical trials, AG337 (p.o. and i.v.
forms) and AG331 (both by Agouron, La Jolla, CA) are
lipophilic potent TS inhibitors with action independent of
the RFC and polyglutamation. Multiple mechanisms
through which cells may overcome TS inhibition have been
described. Combining TS inhibitors with other agents that
affect TS, interfere with TS gene and mRNA regulation, or
inhibit salvage mechanisms of thymidylate depletion may
potentially enable greater clinical utility of this class of
compounds.
Received 5/31/95; revised 9/11/95; accepted 9/27/95.
1 To whom requests for reprints should be addressed, at Division of
Medicine, Box 92, The University of Texas M. D. Anderson Cancer
Center, 1515 Holcombe Boulevard, Houston, TX 77030. Phone: (713)
792-3634; Fax: (713) 745-1827.
Introduction
TS 2 inhibitors are a new class of compounds that target TS,
an enzyme in the folate metabolic pathways necessary for thymidylate synthesis, specifically. By inhibiting TS, these agents
decrease de novo thymidylate synthesis, which is necessary for
DNA synthesis and repair. Contrary to prior empiric approaches
to anticancer drug discovery, the development of new TS inhibitors was based on the targeted and specific design of new
molecules and relied on extensive knowledge of the structure,
conformation, and properties of TS and the mode of action of
folate analogues. These compounds are being tested currently in
preclinical and clinical settings, and their role in clinical practice
as single agents or in combination regimens remains to be
defined. This review will provide a background of the mechanism of TS inhibition, the development and current status of
folate analogues that inhibit TS selectively, the mechanisms of
resistance to TS inhibition, and the current approaches to augment the efficacy of these new compounds.
TS
A critical step in the de novo pathway of DNA synthesis is
the production of the pyrimidine nucleotide TMP from dUMP.
This reaction is catalyzed by the enzyme TS using the folate
cosubstrate CH2THF (Fig. 1) and is the only source of de novo
cellular thymidylate.
TS (Fig. 1) is a two-substrate enzyme that accepts both
dUMP and CHzTHF to form a ternary complex through which
reductive methylation of dUMP to TMP occurs. In this process,
tetrahydrofolate is oxidized to dihydrofolate. This reaction provides the de novo cellular thymidylate nucleotides necessary for
DNA synthesis and repair. TS inhibition results in a thymineless state, which is toxic to actively dividing cells. This cytotoxicity is effected likely by DNA fragmentation that results
from dTTP depletion, which increases misincorporation of
dUTP (1). Cells containing the salvage enzyme TK, which uses
circulating thymidine, can circumvent this cytotoxicity. However, in normal tissues and in some tumor cells, the circulating
thymidine concentrations may not be sufficient to achieve a
significant effect (2).
The enzyme involved in regeneration of tetrahydrofolate
from dihydrofolate is DHFR (Fig. 1). Folate analogues (antifolates), such as MTX, inhibit DHFR, deplete tetrahydrofolate,
and cause a marked decrease in pyrimidine and purine synthesis
(3-5). Mechanisms of resistance to MTX include reduced drug
transport across cell membranes (6-8), reduced drug polyglu-
2 The abbreviations used are: TS, thymidylate synthase; CH2THF, 5,10methylene tetrahydrofolate; DHFR, dihydrofolate reductase; MTX,
methotrexate; 5-FU, 5-fluorouracil; FdUrd, fluorodeoxyuridine; IdUrd,
iododeoxyuridine; RFC, reduced folate carrier; FPGS, folylpolyglutamate synthase; FdUMP, fluoro-dUMP; TK, thymidine kinase; DLT,
dose-limiting toxicity; MTD, maximum tolerated dose; PR, partial response; LV, leucovorin; ICso, 50% inhibitory concentration; AZT,
zidovudine.
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
228 Thymidylate Synthase Inhibitors
MTX
MTX (Glun)
I
t
........
"~ " ,~
I
'
u
I
I Thymidylate
Synthase I
N5-'1°methylene
FH4 Glun)
I=,,, MTX
FH2 (Glun)
FH4 (Glun)
I,DMFRI
FH4 (Glun)
A
!
t°~
I
1
dUMP
dTMP
de novo Pyrimidine
DNA Synthesis
i
Synthesis
......L..2... ~ ~ ~-iv
~
_ ..:L
~
:..~~
V
N 5"I°methenyl _.., IcYCLO I
FH4 (Glun)
E
o
-r
N5 meth'¢l FH4 - ' ~
-'"
T
"=
N10 formyl
"'- FH4 (Glun)
I G.APJAICAR I
~
-__....__"--
FH4 (Glun)
Purines
N5 formyl FH4
Fig. 1 Folate metabolic pathways. Inner square, role of TS in DNA synthesis. Dashed arrows, inhibitory effect. FH4, tetrahydrofolate; FH2,
dihydrofolate; (Glu.), polyglutamate; MS, methionine synthase; CYCLO, cyclo,5,10,methenyl-FH4-cyclohydroxylase; GAR, glycinamide ribotide
transformylase; A1CAR, aminoimidazole carboxamide ribotide transformylase.
tamation (polyglutamation confers intracellular drug retention),
gene mutation resulting in altered forms of DHFR to which
MTX cannot bind effectively, and an increase in cellular DHFR
via D H F R gene amplification (9). The development of antifolates that inhibit TS (rather than DHFR) selectively may circumvent MTX tumor resistance, especially that resulting from
increased levels of DHFR.
TS inhibition can be achieved with either fluoropyrimidines or folate analogue compounds. The first compounds to
have clinically significant TS-inhibiting activity were the fluoropyrimidines 5-FU and FdUrd; these are metabolized to
5-fluoro-2-deoxyuridylate (the most efficacious analogue of deoxyuridylate) and form a ternary complex together with TS and
CH2THF, resulting in potent TS inhibition. These drugs also
may become incorporated into RNA or DNA via fluoro-UTP
(10, 11) or 5-fluoro-dUTP (12), respectively. These events may
obscure quantitation of TS inhibition. Despite this, potentiation
of the cytotoxic effects of 5-FU and FdUrd was predicted and
achieved successfully by the addition of folinic acid to increase
the intracellular level of CHaTHF, resulting in the stabilization
of the ternary complex and thus a higher degree and duration of
TS inhibition (13, 14).
Selective TS inhibition is of interest in drug development
for a variety of reasons. Immunological quantitation using
monoclonal antibodies against TS (15, 16) revealed an inverse
association between the treatment response to 5-FU and the
cellular expression of TS; thus, TS overexpression of tumor
cells can be a marker and prognostic indicator for 5-FU resistance. An association between the degree of TS inhibition and
the clinical response to chemotherapy in colorectal and breast
cancers has been noted (17, 18). Moreover, expression of TS
was found to predict for disease-free survival and survival in
patients with rectal cancer independently (19). Folate analogues
are less susceptible to metabolic degradation than fluoropyrimidines and are not incorporated into RNA or DNA (3). Finally,
tetrahydrofolate is a relatively large molecule providing a variety of sites amenable to manipulation in the design of novel
TS-specific inhibitors.
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Clinical Cancer Research 229
HN--N
I
II
Ptefldlne Ring p-AmlnobenzolcAcid GlutamylResidues
0
3
10
. .NH__~
N
O
COOH
II
I
,~--C- NH-- CH
I
1
"
N
CONH
ZD9331
COOH
"
Tetrahydrofolate
H."
/
.-(.
.,,,"~ CHe~"~,. '~
.'T -"X
~",
II
I
H , N / ~ N ~
~
/NH"('.
i(~
CIOOH
, ) - C - NH-- CH
o
COOH
H.N,,~N,,~
l/
I
]",
c
IcflH CB 3717
CH
c~oo.
/
COOH
I
CH
HN~ C H r ~ %
I
II
I c,,
Memotrexam
COOH
0
?.
NH~
I-
H
s \~
/~'C -NH-iH'
ZD 1694
CH.
COOH
/NH2
NH
COOH
--c~
so~--.
i"oo.
j
1843U89
H~C
CH2
SO,- N
\
CH~
/
O
AG-331
Fig. 2
Chemical structures of tetrahydrofolate, MTX, 1843U89, ZD9331, CB3717, ZDl694, AG337, and AG331.
To reach and inhibit target enzymes such as DHFR or TS,
antifolates enter the cell via the RFC protein transport system on
the cell membrane. Efficient or poor cellular antifolate uptake is
determined by the molecular structure and polarity of the antifolate, the presence of reduced folates or antifolates (which may
compete for the use of RFC), the intracellular folate depletion,
and RFC deficiency (20). Once antifolates are inside the cell,
glutamate residues are added by the enzyme FPGS in a ~-carboxyl linkage (Fig. 2). Polyglutamates with as many as seven or
eight glutamyl residues have been identified (21). These add
more negative charges to the antifolate molecule and increase
solubility (22), resulting in the agent's marked reduction in
efflux from cells and its prolonged retention in tissues having
high FPGS activity, such as the liver. Formation of ternary
complexes with dUMP and folate protects the enzyme from
carboxypeptidase inactivation. Moreover, polyglutamation increases the affinity of folate analogues for folate-dependent
enzymes (but not for DHFR) markedly and results in a poten-
tiation of TS inhibition that may exceed by 100-fold that of the
monoglutamated form (23, 24).
Cellular uptake of antifolates via the RFC and the ability of
antifolates to undergo polyglutamation have major roles in TS
inhibition. A compound that has weak TS inhibitory activity in
enzyme assays may undergo rapid cellular uptake by the RFC
and extensive polyglutamation by FPGS in cell cultures or in
vivo, resulting in potent TS inhibition. Alternatively, a compound that is a potent TS inhibitor in enzyme assays may show
only weak activity in vivo if it does not enter the cell readily or
is an extremely poor substrate for FPGS. Folate analogues may
be regarded as prodrugs with polyglutamation as an activation
step (24).
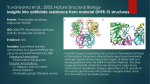
TS Structure. Iterative protein crystallographic analysis
enabled the study of Escherichia coli TS and, subsequently,
human TS in both the native form (25, 26) and the complex with
dUMP and folate cofactor or a folate analogue (26-31). The
primary sequence of the E. coli enzyme has high homology
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
230 Thymidylate Synthase Inhibitors
(46% identity) to the human TS sequence (25), and in the human
enzyme, the active site residues are conserved, with 75% identity (29).
TS is a symmetric, obligate dimer of chemically identical
units of about 35 kilodaltons each (25). Each of the two subunits
folds into a three-layer domain anchored by a large, sixstranded, mixed [3 sheet. A [3 sandwich is created by the backside of one sheet in juxtaposition against the corresponding face
of the equivalent sheet in the second protomer. This back-toback apposition of the two [3 sheets forms the interface between
the two subunits. Although the left-handedness of the [3 sheet
twist in each monomer is normal, the twist of one sheet relative
to the other is unexpectedly right-handed, in contrast to that of
other proteins of similar structure (25, 32). Each [3 sheet is
distorted by a series of stacked [3 bulges, dividing each sheet
into two smaller classical [3 sheets orthogonal to one another.
The stacked [3 bulges are stabilized by hydrogen bonding and
account for the unusual right-handed twist of the opposing [3
sheets. An extended structure is created that anchors the phosphate of bound dUMP and controls the precise orientation of the
catalytically essential sulfhydryl group on a conserved cysteine
residue in the active site (32).
The unique TS portion of the ternary complex crystal form
is a dimer. However, in unliganded TS crystal structures of
humans, E. coli, Lactobacillus casei, and T 4 bacteriophage, this
unit is a monomer. Thus, structural differences between monomers can be observed only in the ternary complex crystal form.
The monomers in this form are similar to one another but differ
from the unliganded structures in mobility, reflecting mechanistic nonequivalence of active sites in TS (27).
The substrate-binding site is a funnel-shape cleft extending
into the interior of each subunit. Components of each monomer
contribute to each of two active sites (25), which are separated
widely on either side of the molecule. This fact accounts for the
inability to dissociate the native enzyme into catalytically active
monomers. Moreover, it suggests a way for the active sites to
communicate in the process of ligand binding (25, 33). There is
no conclusive evidence for cooperativity between monomers.
However, ligand binding is associated with large conformational
changes and involves most of the domains of the protein. Thus,
the liganded state at both active sites will play a role in ligand
affinity (34). Binding studies using equilibrium dialysis and
spectroscopy suggest that the two active sites may not react
equivalently, although both active sites can be filled through
covalent attachment of an inhibitor and folate. Binding studies
of FdUMP suggest that both active sites contribute to this
process in an asymmetric fashion, wherein one site is preferred
over the other and, in some cases, only one active site is used at
a time (33). In the presence of folates or folate analogues,
binding of FdUMP to both active sites is enhanced greatly (35,
36). However, the novel folate analogue and TS inhibitor
1843U89 (Glaxo-Wellcome, Research Triangle Park, NC) promotes the formation of ternary complexes with TS and dUMP as
well as with selective purine nucleotides (36). There has been no
prior evidence that purine nucleotides bind to TS in the presence
or absence of folates or other folate analogues. Surprisingly,
1843U89 not only enhanced the binding of FdUMP or dUMP to
TS but also enabled that of dGMP, GMP, and IMP, which did
not bind TS in its absence. The significance of these findings
remains to be determined.
The tetraglutamated forms of ZD1694 [Tomudex; Zeneca
(formerly ICI Pharmaceuticals) Macclesfield, United Kingdom]
or CB3717 (Zeneca) bind to both active site regions, whereas
CH2THF and 1843U89 prefer one of the two sites (35). The
number of binding sites for dUMP, dGMP, and GMP was only
one per TS dimer in the presence of 1843U89, with the second
site being extremely weak even in the presence of folylpolyglutamates (36). These results suggest that each of the two TS
subunits binds folate substrates or analogues differently, and
that fact has a major role in the inhibition kinetics of each folate
analogue. However, such studies are difficult to perform; interpretation of the data has in the past produced conflicting results;
and this issue has been a subject of considerable debate (27, 36).
TS Catalytic Activity. Methylene tetrahydrofolate is the
source of the methyl group to be transferred to dUMP. It is a
one-carbon donor as well as the subsequent reductant of the
transferred methylene group. The details of this process have
been deduced by studying the ternary complex of TS with
FdUMP and methylene tetrahydrofolate, a stable structural analogue of a true catalytic intermediate. Comparison of the threedimensional structure with that of the apoenzyme provided
insight into the conformational changes that accompany ternary
complex formation and their significance in the reaction process
(26). In a different approach, the ternary complex of TS with
dUMP and CB3717 (a selective TS inhibitor discussed below)
has been used (31).
The above studies suggest that TS may activate dUMP by
the formation of a covalent bond between the sulfhydryl group
of the conserved cysteine residue at the TS active site and C-6
of dUMP (see Fig. 3). This binding is induced by the folate (37)
and converts C-5 of dUMP to a powerful nucleophile (38).
Monoglutamylated folates bind to TS in an ordered fashion in
which dUMP binds first. However, the intracellular pool of
folates consists mainly of polyglutamylated molecules with affinities for TS that may exceed 100-fold (39). This high binding
affinity of the polyglutamates results in a random binding order
of ligands to TS. Moreover, folate analogues that, as a result of
their structures, have a high affinity for TS even in the monoglutamated form can bind to the enzyme before dUMP (31). The
binding of the polyglutamyl moiety to TS involves only a few
localized interactions, such as hydrogen bonds and van der
Waals forces, and seems to depend on more diffuse electrostatic
forces, which permit flexibility and freedom of motion (30).
Only the first glutamate residue near the p-aminobenzoic acid
ring of the folate is fixed rigidly by its interaction with TS. The
additional glutamate molecules are progressively more disordered. The polyglutamyl chain thus originates within the confines of the active site cavity and stretches out along the surface
of TS exposed to solvent (30). This chain acts mainly to constrain the motion of the cofactor but has no significant effect on
the conformation of the ternary complex compared with that of
the monoglutamate. This action leads to augmented binding
affinity of the cofactor for TS, whereas the Vmax/Km value is left
unaffected (40).
Ternary complex formation is associated with a large conformational change involving four residues at the carboxyl
terminus of the protein that close down on the distal side of the
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Clinical Cancer Research 231
H
H
~
"11
--%
o
N~-'N~,/-N
_,x,Ng.
~ ~. CH2
%
HN
O5-
0
[
H2
H",'S-Enz
H
rlbou
I
.i~~~.~
O
S-Enz
I
PABA~'flng~
Proposed chemical mechanism for TS. Reproduced with
permission from The FASEB Journal (34).
Fig. 3
.~
HN~
.
rlbose
~N H Pterin ring
~N~
~---N
H."oO~',,,,...,~6N~--..':
" ~ H
H
H2
" o"~iI I~(Jribcys°se198enzyme~
?~--~ i4~folate
:~ N~::n-
z ".i~iBase
"
1
rlbose
o
rlbose
quinazoline ring of the inhibitor, capping the active site and
sequestering the bound ligands from bulk solvent. These
changes are due mainly to the binding of the folate and not to
dUMP (26, 31); they involve segmental accommodation of
several helices, [3 strands, and loops that move as units against
the [3 sheet interface between monomers. After CHzTHF binds,
its imidazolidine ring opens, and a covalent bond is formed
between its N-5 methylene group and C-5 of dUMP (27). The
steady state intermediate breaks down with a hydride transfer
from C-6 of the cofactor to the transferred methylene group on
dUMP, thus forming dTMP and releasing dihydrofolate (Fig. 3).
This reaction process has been studied also in the presence of
FdUMP or folate analogues (26, 28). In the presence of the
fluorinated dUMP analogue FdUMP, a stable covalent complex
forms between FdUMP, TS, and folate, and a hydride shift
cannot occur; this results in enzyme inactivation. The fluoride of
FdUMP cannot be extracted by TS to force collapse of the
ternary complex that leads to the reaction products. With the
folate analogue CB3717, the formation of a covalent bond
between TS and dUMP is still induced. However, CB3717
cannot form a covalent bond with dUMP, as is the case with
folate and dUMP, and a methylene group transfer cannot occur.
Details of these processes are discussed extensively elsewhere
(26, 27, 34).
I II
I
rlbose
rlbose
D e v e l o p m e n t of TS Inhibitors
CB3717
Extensive analysis of TS inhibition at the molecular level
prompted the planning, synthesis, and development of an antifolate compound, CB3717 (Nl°-propargyl-5 - 8-dideazafolic
acid; Zeneca; Fig. 2).
Preclinical Data. In Vitro Studies. CB3717 is a 2amino-4-hydroxy quinazoline carrying a propargyl group
(-CHz-C-~CH) on N 1° that increases the affinity of this antifolate for the catalytic site of TS greatly (41). In vitro studies with
isolated murine (L 1210) and human (W l-L2) TS demonstrated
that CB3717 was the tightest binding, monoglutamate, folatebased TS inhibitor at the time of its discovery, with a K i of 2.7
nM (41, 42). CB3717 inhibits TS, competing with CHzTHF for
the same site on the enzyme, and has affinity for DHFR in
enzyme assays. However, cell culture studies and clinical trials
indicated that the latter finding was not significant, because the
inhibition of TS was far more potent than that of DHFR (41, 43).
CB3717 does not use the RFC for cellular entry but undergoes
extensive polyglutamation by FPGS. Maximal potentiation of
TS inhibition (114-fold) was achieved by the triglutamate form
of CB3717 (43). The cytotoxicity was completely reversible
with the addition of thymidine to the culture medium but was
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
232 Thymidylate Synthase Inhibitors
only partially reversible with folinic acid, a finding corroborating
prior data showing potent TS inhibition to be the sole cytotoxic
action (41, 44, 45). CB3717 caused a reduction in intracellular
thymine nucleotide pools and an elevation of dUMP levels.
Moreover, CB3717 did not induce significant overproduction of
DHFR in tumor cells, and cells resistant to MTX as a result of
raised DHFR levels were not cross-resistant to CB3717. Accordingly, CB3717 was a potent growth inhibitor in both MTXsensitive and -resistant cell lines (41).
Animal Studies. L1210 leukemia-bearing mice administered CB3717 achieved a long-term survival rate of 90% without significant toxic effects, whereas optimal doses of MTX
elicited a long-term survival rate of only 20% (41). A daily × 5
dose schedule of CB3717 produced dose-related increases in
mean survival time. CB3717 caused elevated deoxyuridine and
depleted thymidine levels in plasma (45). Biliary excretion was
the major route of drug elimination. In mice, the DLT was renal,
with drug accumulation and retention in the kidneys (46). Precipitation within the renal tubule resulting from the poor solubility of CB3717 in normal pH urine may account for its
nephrotoxicity (42, 47).
Clinical Studies. Phase I Studies. Because of the variable incidence of side effects, the MTD of CB3717 was difficult
to determine with precision (48). The DLT of a 1-h infusion was
nephrotoxicity. In >50% of patients, significant reductions in
glomerular filtration rates occurred at doses >400 mg/m 2, although milder reductions were observed at lower dose levels
(48). Malaise, associated with elevated liver enzymes, resulted
in weakness, lethargy, arthralgia, and occasional fever. Only
mild hematological side effects were observed. A subsequent
Phase I trial found renal toxicity to be severe and unpredictable
(49); another trial demonstrated that urine alkalinization decreased the renal toxic effects but noted that profound malaise
was present at dose levels as low as 150 mg/m 2 (50). In these
trials, the drug demonstrated antitumor activity in ovarian,
breast, and lung cancer and mesothelioma.
Phase II Studies. A Phase II study showed the activity of
CB3717 in advanced breast cancer, but severe renal failure
occurred in 17% of patients (51); urine alkalinization was not
used during this study. Other trials described the activity of
CB3717 in cisplatin-refractory ovarian cancer (resolution of
malignant ascites in 2 and a decrease of CA-125 levels in 1 of
8 patients; Ref. 50) and hepatocellular cancer (6 patients with
decreases in tumor sizes and >50% fall in serum a-fetoprotein
levels, classified as partial remissions, and 1 patient with stable
disease among 14 chemotherapy-naive patients; Ref. 52).
However, because severe renal toxic effects were unpredictable, and profound malaise was noted even at lower doses,
further development of CB3717 was abandoned. Nevertheless,
this drug served as a prototype for studies of TS inhibition and
was the first compound to be developed rationally to inhibit TS
selectively.
ZD1694 (Tomudex)
Available preclinical and clinical data indicated that a less
toxic analogue of CB3717 would be useful in cancer treatment.
Because the renal and hepatic toxic effects of CB3717 appeared
due to its poor aqueous solubility (46, 53, 54), further research
focused on the synthesis of water-soluble analogues. This led to
the development of quinazoline compounds, in which the benzene ring of the p-aminobenzoate residue (see Fig. 2) has been
replaced with various ring structures, including pyridine, thiophene, or thiazole (24, 54). After extensive biological in vitro
and in vivo evaluation of such analogues, the Nl°-methylthio phene analogue ZD1694 (Tomudex; Zeneca; Fig. 2) was selected for further development (54). This new quinazoline folate
analogue inhibits TS selectively. Similar to CB3717, ZD 1694
results in decreased TMP production, which leads to inhibition
of DNA synthesis, resulting in cell death. Because Phase III
trials of this agent have been completed, its properties and
development are discussed in detail below.
Biochemistry and in Vitro Studies. ZD1694, or N-(5[N-(3,4-dihydro-2
methyl-4-oxoquinazolin-6-ylmethyl)-N-methyltk; 1amino]-2-thenoyl)-L-glutamic acid, is a yellow-brown to dark
green granular powder that is water soluble at pH 7. ZD1694
behaves as a mixed noncompetitive TS inhibitor with respect to
tetrahydrofolate (42). As expected of a pure TS inhibitor and as
noted previously with CB3717, the addition of thymidine prevents
the in vitro cytotoxic action of ZD1694 (55). In contrast to CB3717,
ZD1694 uses the RFC for cellular entry effectively, and thus,
higher intracellular levels are available rapidly for polyglutamation
by FPGS (42). ZD1694 is an excellent substrate for FPGS, with an
affinity 30 times higher than that of CB3717 (24, 42). In cell
cultures, 95% of the drug is present intracellularly in the polyglutamated form within 4 h of ZD1694 exposure, resulting in more
potent and prolonged TS inhibition (24, 56). Because of its effective use of the RFC and FPGS, this analogue is 500-fold more
active in inhibiting cell growth than CB3717, despite being 20
times less potent as a TS inhibitor in enzyme assays (Ki, 60 nM;
Ref. 42). ZD1694 also inhibits DHFR via polyglutamation but is
--100-fold more specific for TS than for DHFR (56). Because the
activity of ZD1694 is inhibited completely by thymidine (42), TS
inhibition is responsible for limiting the cell growth rate. Folinic
acid antagonizes this growth inhibition in tumor cell lines in a
competitive fashion. In vitro data suggest that folinic acid competes
with ZD1694 for both cellular uptake via the RFC and intracellular
polyglutamation.
Activity. ZD1694 alone was 1800 times more cytotoxic
to MGH-U1 bladder cancer cells after a 24-h exposure than was
5-FU plus LV (57). Progress through the cell cycle was delayed
in a dose-dependent manner in HCT-8 ileocecal human carcinoma cells exposed to ZD1694 (58), and further studies showed
its significant activity in cisplatin-resistant (59) and ileocecal
cancer cells (60). The cell cycle specificity of ZD 1694-induced
DNA damage was analyzed in HCT-8 cells. Commitment to
DNA replication was a prerequisite for damage, observed only
in the early to middle S-phase (61).
Animal Pharmacology. Experiments in mice bearing a
variant lymphoma-L5178Y tumor line showed that a single dose
of 10 mg/kg ZD1694 cured the animals, whereas CB3717 exhibited poor activity at the MTD of 200 mg/kg (62). The
rationale for a single-dose schedule is the rapid cellular transport
of ZD1694 and its metabolism to polyglutamates. ZD1694 did
not demonstrate renal and hepatic toxic effects at doses of 500
mg/kg, as observed with CB3717 at 100 mg/kg (63). Human
tumor xenograft studies showed ZD1694 to be superior to
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Clinical Cancer Research 233
CB3717, 5-FU, and MTX with respect to antitumor activity and
therapeutic margin (64).
Animal Toxicology. Murine toxic reactions consisted of
leukopenia, thrombocytopenia, and damage to the small intestinal mucosa. Unlike the renal and hepatic toxic effects of
CB3717, the hematological and gastrointestinal toxic effects of
ZD1694 could be prevented by synchronous thymidine administration, suggesting that these effects result from the antiproliferative activity of ZD 1694 (42) and not from other physical or
chemical properties. Moreover, folinic acid administration conferred some improvement in neutrophil and platelet counts as
well as in gastrointestinal toxic reactions in ZD1694-treated
BALB/c mice (65, 66), suggesting possible "rescue" activity of
thymidine or folinic acid in patients with severe toxic reactions
to ZD 1694.
In dogs treated with the daily × 5 schedules of ZD1694
(0.5 and 1 mg/mZ/day), myelosuppression occurred 4 days after
the last dose and had resolved by day 8. At the same dose
schedules, reversible histopathological changes in the epididymis, testis, and thymus were observed. These changes included
the maturation arrest of spermatogenesis, absence of or reduced
spermatozoa, and exfoliated seminiferous epithelial cells in the
testis and epididymis. Thymic lymphocytosis and atrophy were
noted (67). In genetic toxicity assays, ZD1694 is not mutagenic
but causes DNA strand breaks through its antimetabolic activity.
ZD1694 (25 mg/m 2) caused a reduction in canine fetal body
weight and an increase in postimplantation fetal loss. This dose
level was also associated with an increased incidence of major
fetal soft-tissue and skeletal abnormalities; therefore, ZD1694 is
contraindicated in pregnant women (67).
Animal Pharmacokinetics. After the i.v. administration
of ZD1694 to rats and dogs, the major and probably only
remaining circulatory compound was unchanged drug. Biliary
excretion predominates in the rat, whereas renal and biliary
routes of elimination are equal in the dog. Rapid drug clearance
was noted in both the rat and dog (t,/:, 0.6 h). The drug disposition was triphasic, with short initial phases and a relatively
slow ~/phase in both species (t,/2"y, 22-56 and 14-29 h in the rat
and dog, respectively). The long terminal phase is probably due
to the slow return of ZD1694 to the plasma from a deep tissue
compartment or to the release of polyglutamate-containing RBC
from the marrow into the circulation. The latter has been observed at 2 - 4 weeks in humans. Significant ZD1694 accumulation was not observed with repeated daily administration (63,
68).
Polyglutamates were detected in liver, kidney, and intestinal tissue from mice injected with 5 mg/kg [5-3H]ZD1694 and
accounted for at least 75% of the total drug concentration.
Polyglutamated forms were retained in tissues even when most
of the drug had been cleared from the plasma (69), supporting
the use of the infrequent-dose schedule implemented subsequently in clinical trials.
Clinical Studies. Phase I Studies. The first Phase I trial
of ZD1694 began in Europe in February 1991 and included 61
patients with solid tumors (colorectal, ovarian, head and neck,
upper gastrointestinal, and others), most of whom had received
prior chemotherapy (70, 71). After single doses of ZD1694,
polyglutamation resulted in prolonged TS inhibition in mouse
tumors (69); therefore, patients were treated with a single 15-
min ZD1694 infusion every 3 weeks at doses ranging from 0.1
to 3.5 mg/m 2. Pharmacokinetic studies revealed interpatient
variability but little intrapatient variability with repeated dosing.
The plasma concentration-versus-time profile for ZD1694
showed a triphasic decline following infusion and a prolonged
t,/2y (50-100 h), as observed in the rat and dog (71).
In this trial, the DLTs for ZD1694 were gastrointestinal,
hematological, and malaise or asthenia at an MTD of 3.5 mg/m 2.
No correlation was observed between the pharmacokinetic parameters and the increases in liver enzymes. However, the long
t,/2y of the drug may be responsible for prolonged hematopoietic
stem cell inhibition or gastrointestinal toxic effects. There was
no statistically significant difference in the pharmacokinetic
parameters (plasma concentration-versus-time profiles, peak
plasma concentration, and terminal phase tv2) or toxic effects
between patients with normal versus mild to moderate hepatic
dysfunction (bilirubin, 1.25-3 times the upper limit of normal;
aspartate aminotransferase or alanine aminotransferase, 3-10
times the upper limit of normal). No dose reduction is thus
recommended for patients with hepatic dysfunction. Contrary to
this, patients with mild to moderate renal impairment (defined as
creatinine clearance <65 ml/min) had statistically significantly
higher pharmacokinetic parameters than did patients with normal renal function. The drug manufacturer recommends that
patients with renal impairment receive reduced doses of this
drug. Among the 28 patients in this trial who received ZD1694
doses of 3.0 and 3.5 mg/m 2, 43% developed asthenia or malaise,
32% had diarrhea, 32% had grade 3 or 4 reversible elevations of
liver transaminase levels, and 21% had grade 3 or 4 leukopenia.
Four patients died of complications related to drug exposure at
dose levels of 3.0 and 3.5 mg/m2; 3 of these 4 had grade 4
diarrhea. Death was attributed to disease progression in 1 patient, to cardiac decompensation in another who had a prior
myocardial infarction, to dehydration in the third patient, and to
pulmonary hemorrhage associated with grade 4 thrombocytopenia in the fourth patient (71-74). Three objective PRs were
reported, one each in ovarian cancer, breast cancer, and adenocarcinoma of unknown origin. All patients had received prior
chemotherapy (71-74). Because patients had poor tolerance of
3.5 mg/m / in this Phase I trial, the recommended Phase II dose
was 3.0 mg/m 2.
A U.S. Phase I trial of ZD1694 conducted at the National
Cancer Institute included 50 patients; 76% had colorectal cancer
treated previously with 5-FU-based regimens, and the others had
lung cancer, sarcoma, or hepatoma. ZD1694 was administered
as a 15-rain infusion every 3 weeks at dose levels between 0.6
and 4.5 mg/m 2 (75, 76). In this trial, the DLTs for the drug, first
seen at 2.8 mg/m 2, were grade 3 fatigue and malaise that lasted
for several days and increased in severity or duration with
repeated dosing. The only other DLT was neutropenia. In contrast to the European Phase I trial results, in this U.S. trial, the
MTD was 4.5 mg/m 2, gastrointestinal and hematological toxic
effects occurred less frequently, and no treatment-related deaths
were reported. No complete responses or PRs were observed in
this trial, but two minor responses were reported (one in a
patient with colon cancer and one in another with sarcoma).
Based on results of this U.S. trial, the recommended ZD1694
dose for Phase II studies was 4.0 mg/m 2 (75, 76).
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
234 Thymidylate Synthase Inhibitors
Phase H Studies. Various completed international clinical trials (67, 77-83) together accrued 439 patients with eight
different tumor types, including 177 patients with colorectal
cancer, 46 with breast cancer, 33 with hepatocellular cancer, 31
with ovarian cancer, 41 with non-small cell lung cancer, 74 with
gastric or pancreatic cancer, and 21 with small cell lung cancer.
In all Phase II studies, patients received ZD1694 at 3 mg/m 2.
Based on the recommendation of the National Cancer Institute
Phase I trial and on the observed lack of toxicity with 3.0
mg/m 2, 19 patients with non-small cell lung cancer received 4.0
mg/m 2. The toxicity reported with the higher dose was comparable to the 3.0-mg/m 2 dose (67).
The most frequently observed adverse events or laboratory
abnormalities in Phase II studies were asthenia, diarrhea, nausea
and vomiting, leukopenia, and elevations in liver transaminase
levels. Twelve percent of patients experienced severe asthenia
or malaise. Overall, severe toxic effects (WHO grade 3 or 4)
were observed as anemia in 6%, neutropenia in 14%, elevated
transaminase levels in 18%, and diarrhea in 8%. Grade 3 or 4
nausea and vomiting were seen in 12% but were controlled
easily with antiemetics. Nonspecific cutaneous effects were
noted in 14% as maculopapular rashes. Five patients died of
severe drug-related hematological suppression and sepsis combined with severe gastrointestinal toxic reactions.
In Phase II trials, objective response rates were noted in
6.5% of patients with platinum-resistant ovarian cancer, 9%
with chemotherapy-naive, non-small cell lung cancer, 25% with
advanced breast cancer who had received no prior chemotherapy, and 26% with advanced colorectal cancer who had received
no prior chemotherapy (67, 77-80).
The Phase II trial of ZD1694 (3.0 mg/m 2 every 3 weeks) in
22 patients with previously untreated advanced pancreatic cancer reported PRs in 14%, all of whom continued to respond for
4-5 months (81). The ZD1694 Phase II trial in advanced colorectal cancer involved 177 patients, >80% of whom had hepatic
metastases (80, 84) and only 5% of whom had received adjuvant
chemotherapy. All received 3 mg/m 2 ZD1694, which was administered without dose reduction or delay in 82% of the patients (67). Almost 50% of these 177 patients received five
courses of treatment, and 20% received more than six cycles.
Objective responses were noted in 26%, with an average response duration of 6-7 months. In an additional 26%, however,
signs of antitumor activity (minor tumor response or decrease in
tumor marker levels) were noted.
Grade 3 or 4 toxic effects included asthenia in 12% and
nausea or vomiting in 10%. Grade 4 neutropenia occurred in
3%. In 4% of patients, lower extremity cellulitis that began
frequently in one leg and subsequently involved both legs was
observed. This problem responded to antibiotic treatment, although microorganisms were not cultured from the areas of
inflammation in any of the cases. Most patients who developed
cellulitis had history of diabetes, deep venous thrombosis, or
concurrent neutropenia. Two patients died of severe diarrhea,
mucositis, and hematological toxic effects; one of these had
received prior radiation therapy for non-Hodgkin's lymphoma.
An additional patient died; however, he did not receive aggressive treatment for diarrhea and dehydration (67). These trials
stressed the need for early hospitalization and vigorous support
of patients with severe gastrointestinal toxic effects, especially
in association with myelosuppression. Moreover, folinic acid
may ameliorate severe, established, ZD1694-induced toxic reactions (66).
Based on its antitumor activity and safety profile in colorectal cancer, ZD1694 seemed to be a promising candidate for
comparative Phase III trials. Preclinical data in colon cancer cell
lines suggested that ZD1694 may not follow the resistance
patterns of 5-FU and thus could prove useful against 5-FUresistant clones (64). The objective response rate of 26% obtained with 3 mg/m 2 ZD 1694 compares well with response rates
recently reported in a meta-analysis of data from advanced
colorectal cancer patients treated with 5-FU plus LV (85). The
incidence of severe toxicity at this dose of ZD1694 also compares favorably with North Central Cancer Treatment Group
data for 5-FU plus folinic acid (86). Contrary to 5-FU, which is
extensively metabolized, ZD 1694 is eliminated primarily by the
kidneys as an intact drug, and its clearance can be predicted by
simple studies of renal function. Moreover, ZD1694 is administered easily as a single i.v. dose every 3 weeks, whereas 5-FU
plus LV is often given as a weekly or 5-day i.v. regimen.
Phase III Studies. A European Phase III trial comparing
3.0 mg/m 2 ZD1694 with 5-FU plus LV in 437 patients with
advanced or recurrent colorectal cancer was completed recently;
preliminary data (with a median follow-up of 5.3 months) show
response rates of 20 and 13% for Tomudex and 5-FU, respectively. In addition, 9.4% of patients who received Tomudex and
3% of those in the 5-FU plus LV group had a 40-50% reduction
in measurable lesions. Mucositis and WHO grade 3 and 4
neutropenia were lower in the Tomudex group (P < 0.001). 3
The North American Phase III trial opened to accrual in March
1994 and compared 3 mg/m 2 ZD1694 with 5-FU plus LV in
advanced colorectal cancer. Initially, this trial also included a
4-mg/m 2 ZD 1694 arm, but unexpected severe toxic effects and
concern about the safety profile led to early closing of that dose
arm. The trial continued as a two-arm study and closed to
accrual on June 30, 1995. Results from this study are pending.
Tomudex was approved in the United Kingdom for treatment of
advanced coiorectal cancer in August 1995.
Newer TS Inhibitory Agents
In an effort to deal with the various mechanisms of tumor
resistance and to increase the activity of TS inhibition, new
compounds have been synthesized (see Fig. 2 and Table 1).
ZD9331
Antifolates that are potent TS inhibitors but do not require
extensive polyglutamation to exert adequate cytotoxicity are
presently under development; such agents can counteract reduced polyglutamation in tumors that express low or defective
FPGS (resulting in less potent TS binding and increased efflux
of the monoglutamate from the cell). Such an antifolate is
ZD9331 (Zeneca; Fig. 2), a water-soluble quinazoline TS inhibitor that, like ZD1694, uses RFC for transport and enters cells
readily but, unlike it, is not a substrate for FPGS as a result of
3D. Cunningham, personal communication.
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Clinical Cancer Research 235
Table 1 TS inhibitors currently under development
ZD1694
(Tomudex)
ZD9331
AG331
AG337
Refs.
42, 73, 84
87-89
36, 91, 94
99, 101, 109
100, 104, 108
Manufacturer
Zeneca
Zeneca,
Glaxo-Wellcome
Agouron
Agouron
Use of RFC
Yes
Yes
No
No
No
Polyglutamation
Yes
No
Yes (see comment)
No
No
Phase I trials
Phase I trials
Phase II trials
Compound
Current status
Comments
Phase III trial vs.
5-FU and LV in
colorectal cancer
completed
1843U89
Preclinical trials
One-step polyglutamation to
diglutamate only; increases
intracellular retention, not
potency of TS inhibition
a ~-tetrazole moiety that inhibits ~ polyglutamation. ZD9331
has a K i of 0.4 nM against isolated TS. The cell growth ICso of
ZD9331 is 25 nM in L1210 cells and 7 nM in W1L2 cells. These
values increase to >4000 nM in the presence of thymidine,
confirming the TS locus as the site of action of ZD9331. As
expected, this activity of the antifolate is retained against the
L1210:RD1694 cell line, which cannot polyglutamate antifolates (87).
Pharmacokinetic studies after i.v. bolus injection of
ZD9331 in mice showed a t'/:~t of 4 - 6 h (in contrast to 100 h for
ZD1694; Ref. 88). Because ZD9331 is not retained in cells by
polyglutamation, a prolonged infusion (3 mg/kg over 24 h) is
required to exert a curative effect on L5178Y T K - / - tumors.
The new compound has a therapeutic ratio of - 8 compared with
1.5 for ZD1694. Compared with antitumor doses of ZD1694,
which produced toxic effects to the bone marrow and small
intestine, antitumor doses of ZD9331 produced only hematological toxicity. Murine experiments showed the activity of
ZD9331 against a panel of human tumor xenografts, including
ovarian, colorectal, gastric, and small cell lung cancers (89).
Currently, this compound is in a preclinical stage of development.
1843U89
1843U89 is a novel benzoquinazoline folate analogue (Fig.
2) in which the pteridine nucleus of the folate molecule is
replaced by a lipophilic benzoquinazoline moiety. This compound lacks any structural feature corresponding to the p-aminobenzoyl glutamate moiety of folates (90). 1843U89 is an
extremely potent, noncompetitive TS inhibitor in enzyme assays
(Ki, 90 pM), with kinetics suggesting binding to TS at a site
independent of the substrate-binding site. Growth inhibition can
be reversed by thymidine alone but not by folinic acid, indicating that TS is its exclusive site of action (91). 1843U89 enters
the cells via the RFC and, although an excellent substrate for
FPGS, is metabolized only one step to a diglutamate form. The
monoglutamated form is as potent a TS inhibitor in vitro as the
polyglutamated derivatives of ZD1694 (91). In contrast to other
Good p.o. bioavailability
antifolates, increasing the number of glutamate residues of
1843U89 enhances the TS binding and inhibitory actions of this
compound only slightly. However, metabolism to the diglutamate form increases 1843U89 intracellular accumulation and
retention markedly (92).
Experiments with the human TK-deficient GC3TK cell
line, used to circumvent problems associated with murine RFC
transport and the high circulating thymidine levels that normally
counteract the action of the drug in mice, indicate that 1843U89
has marked in vivo antitumor activity (91). Further studies
showed its activity in human colonic WiDr adenocarcinoma
multicellular tumor spheroids (93) and in xenografts of human
ovarian SKOV-3 and colonic DLD-1 cancer in CD-1 athymic
mice (90, 94). The first Phase I study with this agent is currently
underway.
Computer-assisted Drug Discovery
Historically, anticancer drug discovery relied on screening
natural or synthetic compounds using receptor- or cell-based
assays and on developing antimetabolites based on key biochemical pathways and chemical formulas of involved molecules (95). These compounds are then modified to improve their
activity and toxicity profiles. X-ray crystallographic analysis of
molecular structures achieves resolution that enables construction of the three-dimensional structure of a protein, ligand, or
receptor-ligand complex. Studies of the binding of inhibitors to
their targets and of receptor-ligand interactions provide information that then may be used in the de novo drug design. The
structure of a receptor-ligand complex can be used in computerassisted graphics and molecular modeling for the design process
of the ideal ligand (29). This process uses computer-predicted
interaction energies between a protein surface of a known structure and a functional group probe (e.g., hydroxyl, amino, or
methyl; Ref. 96). These methods are changing the process of
drug discovery and development.
AG337 and AG331. Using the above approach for drug
discovery, TS was a target for the computer-assisted, structurebased design of inhibitors using high-resolution, X-ray crystal-
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
236 Thymidylate Synthase Inhibitors
lography and molecular mechanics to analyze the E. coli TS
structure (29, 97-99) and to investigate its interaction with
inhibitory ligands, including 5-FU and a classic glutamatecontaining folic acid analogue. With computer programming,
molecules were then selected that would occupy the maximum
space at the TS-active site and use electrostatic forces or hydrogen bonding optimally to stabilize the enzyme-inhibitor complex. The newly synthesized compounds are lipophilic, lack a
negatively charged glutamate side chain, and are extremely
potent TS inhibitors (ICsos in the nanomolar range). These
properties imply that these drugs can enter cells readily without
the RFC and thus have activity in tumor clones deficient in this
carder protein. Drug potency is not dependent on polyglutamation. These drugs may exert effective TS inhibition on FPGSdeficient cells; however, the prolonged intracellular retention of
the new compounds, conferred normally by polyglutamation
and causing prolonged TS inhibition, is lost.
The new compounds, AG337 and AG331 (Agouron, La
Jolla, CA; Fig. 2), are potent TS inhibitors with purified human
TS Kis of 16 tXM (100) and 2 nM (99), respectively. Both
compounds have minor structural similarity to the natural folate
cofactor, and both inhibit the growth of a variety of tumor cell
lines; the IC5o for L1210 in vitro ranged from 0.18 to 3.5 IxU
(101). The addition of thymidine reversed both growth inhibition and cell cycle arrest in the early S-phase, findings consistent
with TS as the primary site of action (100-102). Moreover, both
AG337 and AG331 were active in vitro against multidrugresistant cell lines (102).
AG337. Animal Pharmacokinetics o f AG33Z AG337
had excellent p.o. bioavailability (96). p.o. absorption of AG337
was rapid, with peak plasma levels as measured by high-performance liquid chromatography achieved in < 1 h. Comparison of
the areas under the curve after administration of i.v. or p.o.
AG337 at 75 mg/m 2 demonstrated the drug to have p.o. bioavailabilities of 100% in mice and >80% in dogs.
Animal Pharmacology and Toxicology. p.o. AG337
demonstrated 100% curative activity against the i.p.- or i.m.implanted L5178Y/TK murine lymphoma and produced long
growth delays in the GC3 M/TK human colon carcinoma i.p.
xenograft. The murine antitumor activity of AG337 was elicited
at dose levels that were well tolerated, even on a repeated-dose
schedule; high dose levels also were tolerated in dogs (100).
Five-day infusion schedules of AG337 in mice were well tolerated and induced substantial growth retardation in 90% of
tumors, with a median delay of 14 days (103). These data
corroborate in vitro AG337 studies demonstrating that a 24-h
exposure to this agent was not sufficient to induce a significant
rate of cell death but that a 72- to 120-h exposure produced
concentration-dependent cytotoxicity (102).
Clinical Studies o f p.o. AG33Z Preliminary data from an
ongoing Phase I trial demonstrate that p.o. AG337 has a bioavailability of >80%, with peak levels achieved within 1 h and
the drug still detectable at 6 h. Mild nausea but no myelosuppression was observed at 360 mg/m 2 (104).
Clinical Studies o f i.v. AG33Z In a Phase I study of
AG337 administered as a 24-h infusion, plasma deoxyuridine
levels increased to 60-390% of pretreatment levels (an event
that suggests significant TS inhibition) but normalized rapidly
after the infusion ended. No tumor antiproliferative effects were
observed in that trial (102, 103, 105). These observations and
murine data on prolonged infusion schedules suggest that prolonged infusions are necessary to optimize antiproliferative effects.
Phase I studies of AG337 in a 5-day, continuous-infusion
schedule were completed recently in the United States and
United Kingdom (103, 105, 106). In these trials, the t,/2 of the
drug was <2 h. Drug clearance decreased from 190 ml/min/m2
for the lowest dose to 85 ml/min/m2 for the highest dose,
indicating the saturable elimination and nonlinear pharmacokinetics of this agent (107). Myelosuppression and mucositis were
the DLTs; radiographic and biochemical evidence of antitumor
activity also was noted. Based on these trials, the recommended
Phase II dose was 1000 mg/m2/day (108). Phase II trials in
malignant tumors of the head and neck, lung, pancreas, prostate,
liver, and colon were initiated at multiple clinical centers in the
United States in October 1994 and are currently ongoing.
AG331. Treatment of L1210 cells with 4-10 IXMAG331
in vitro elicits a >85% reduction in TS activity. AG331 was
active against leukemia and colon cancer cell lines, and its
antitumor activity was observed in vivo against the i.p.-implanted murine L5178Y lymphoma (102). In animal studies,
plasma AG331 concentrations of >20 ~M were tolerated without irreversible toxic effects. The toxic effects seen most frequently in preliminary animal investigations are mild to moderate grades of local vein irritation, transient weight loss, and
histamine release resulting in flushing or swelling (102).
AG331 is currently being evaluated in Phase I trials. A
study of AG331 administered as a 10-min i.v. infusion to 18
patients with refractory tumors has been completed (102). The
tl/2 of the drug was found to be - 2 0 h; with each dose increase,
a steady increase in the area under the curve and a dosedependent decrease in drug clearance were noted, indicating the
saturable elimination kinetics of AG331 (88). Mild to moderate
nausea and vomiting and mild flushing were observed at 130
and 225 mg/m 2, respectively, and may be attributed to histamine
release (102). The MTD has not yet been reached, and thus far,
objective tumor responses have not been observed in the ongoing Phase I trial of AG331 (109).
Recent preclinical data on AG331 in H35 rat and HEPG2
human hepatoma cells revealed that at higher doses of this
antifolate, a loss of the TS inhibitory effect occurred, yet cytotoxic effects were preserved. This suggests an alternative mode
of action for AG331 and the need to investigate the possibility
that in these hepatoma cells, this drug undergoes biotransformation into other, as yet unidentified, toxic metabolites (110).
Resistance to TS Inhibition
Multiple mechanisms of resistance to the new selective TS
inhibitors have been described, with many of the studies using
ZD 1694 as their prototype. The active transport of ZD 1694 via
the RFC and subsequent polyglutamation by FPGS, resulting in
increased TS affinity and intracellular polyglutamate retention,
are responsible for the potent TS inhibition and antitumor activity of the drug in vitro and in vivo. Decreased uptake via the
RFC, failure to polyglutamate ZD1694, and elevation of intracellular TS levels by TS gene amplification have been described
in studies of ZD1694-resistant cell lines (111, 112) and are
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Clinical Cancer Research 237
similar to observed mechanisms of resistance to 5-FU (113) or
MTX (114-116). Some issues have been addressed in developing new folate analogues that are more potent TS inhibitors than
ZD1694. LY231514 (Eli Lilly Research Labs, Indianapolis, IN),
with a Ki of 3.4 riM, also uses the RFC and polyglutamation to
inhibit selectively TS (117, 118). A Phase I trial of this drug has
been completed. Neutropenia was the DLT, and nonhematological toxicities included mild fatigue, anorexia, and nausea. No
antitumor responses were observed (119). Other drug development strategies led to compounds such as ZD9331 (which does
not require polyglutamation; Refs. 87-89), 1843U89 (which
requires only one-step polyglutamation; Refs. 36, 91), and
AG331 (99, 109) and AG337 (which require neither transport by
the RFC nor polyglutamation to exert their cytotoxic action;
Refs. 108, 120).
TS Induction. Induction of TS leading to increased TS
activity levels as a result of TS protein overexpression has been
noted as a resistance mechanism to 5-FU (18). Gene amplification is the primary mechanism by which DHFR levels increase
after cell exposure to MTX, resulting in MTX resistance, and
this has been described also with TS in cell lines resistant to
ZD1694 (112). In addition, overexpression of TS protein as a
result of deregulation of TS mRNA translation during treatment
with a TS inhibitor is another mechanism of TS induction.
Translation of human TS mRNA is controlled by its own
end product (TS) in a negative autoregulatory manner (121,
122). TS protein inhibits TS mRNA by binding of the protein to
specific TS mRNA sequences critical for the initiation of translation. TS protein can regulate its own mRNA translation. This
TS-specific process does not affect translation of unrelated
mRNA transcripts. The intracellular level of TS protein is thus
critical in the regulation of TS mRNA translation. This model
could explain in vitro, in vivo, and clinical observations describing TS level increases within cancer cells following acute exposures to 5-FU (18, 123-125). FdUMP, dUMP, and selective
TS inhibitors (ZD1694) may bind to TS protein, producing a
conformational change that inhibits its binding to TS mRNA.
Translation of TS mRNA then proceeds uncontrolled, resulting
in TS accumulation and drug resistance (122, 126). Coadministration of a translational (but not a transcriptional) inhibitor
overcame TS protein accumulation. In addition, TS protein
accumulation induced by ZD1694 was not reversed by thymidine coadministration despite a complete reversal of cytotoxicity. This explains observations of increases in TS levels of up to
40-fold in normal breast epithelial cells and up to 10-fold in
human breast cancer cells after ZD1694 exposure, whereas TS
mRNA levels remain unchanged (126). In these synchronized
cells, TS protein induced normally during the S-phase and
decreasing subsequently during G~ was found to be expressed
constitutively throughout the entire cell cycle after ZD1694
treatment. No overexpression of TS mRNA could be demonstrated. Once accumulated by ZD1694, TS was not induced in
the S-phase, nor did it decrease in G2, and it remained expressed
throughout the cell cycle. Thus, TS accumulation was potentiated by TS expression throughout the entire cycle after ZD 1694
treatment.
These effects were attributed to a loss of inhibition of TS
mRNA translation, whereas TS gene transcription remained
unchanged. Subsequent studies of human manamary epithelial
cells treated with 1843U89 or AG331 and LY231514 demonstrated that it is possible to achieve higher rates of TS protein
synthesis and resistance by the same mechanism described for
ZD 1694 (127). These in vitro data obtained using synchronized
cells suggest that TS induction may develop in such cell populations during treatment with most, if not all, TS inhibitors.
Accumulation of TS protein may result in clinical drug resistance in patients treated with 5-FU or folate analogues, and these
data may explain in part the low response rates to these drugs in
the clinical setting.
TS Interaction with Cancer-related Genes. Normal or
abnormal expression of certain genes, including p53 and bcl-2,
can affect the ultimate response of tumors to cytotoxic drugs
(128-132). TS may affect these genes specifically. In vitro,
translation of p53 mRNA was repressed specifically with the
addition of exogenous human TS in human colon cancer H630
cells, and TS was demonstrated to complex with p53 and c-myc
mRNAs (133, 134). The role of this mRNA-protein interaction,
although not yet clear, suggests the possibility of a regulatory
role of TS in p53 and c-myc cellular expression. In addition,
c-myc protein decreased and p53 and Rb proteins increased after
exposure of HCT-8 cells to ZD1694 (135). Although preliminary, these data are intriguing, because such interactions may
have a critical role in retarding cell progression through the
S-phase and in initiating apoptosis after drug exposure. If the
cytotoxic activity of TS inhibitors is mediated ultimately by the
induction of apoptosis, then mutations in the genes encoding
these proteins or interference with their activity could decrease
the expected cytotoxicity. Studies of bcl-2 expression in human
lymphoma cells demonstrated that this is possible in vitro.
Following a 36-h exposure to cytostatic drugs, including FdUrd,
cells transfected with a vector alone underwent apoptosis
readily. In contrast, cells transfected with a bcl-2 vector and
expressing this protein showed markedly decreased levels of
apoptosis (8 versus 67%) independent of TS levels and TS
enzymatic activity that were unaffected by bcl-2 expression
(136). Preliminary reports from studies of p53 function in patients with advanced colorectal cancer suggest that patients with
point mutations in p53 may not respond to chemotherapy with
5-FU and LV (137). Taken together, these data emphasize the
increasing importance of a molecular understanding of intrinsic
insensitivity to TS inhibitors as well as of TS interaction with
cell cycle regulatory genes.
Pretreatment TS Levels. Pretreatment TS protein levels
and TS gene expression predicted for responses of metastatic
colorectal and primary gastric cancer to treatment with a combination of 5-FU and LV and a combination of cisplatin, 5-FU,
and LV, respectively (15). Tumors with high levels of TS
protein (measured by Western blot using the TS 106 monoclonal
antibody and densitometry scanning) and TS gene expression
(quantitated by reverse transcription PCR and expressed as a
TS:[3-actin mRNA ratio) showed poor responses to therapy,
whereas tumors with low TS protein and gene expression had
more responsive disease. These data are preliminary, are based
on small numbers, and will require validation in larger clinical
trials. However, they do suggest that, in the future, clinicians
may be able to predict responses to 5-FU-containing regimens
based on pretreatment TS protein levels or TS gene expression.
Together with the data from TS induction after exposure to TS
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
238 Thymidylate Synthase Inhibitors
inhibitors before and after therapy, quantitation of TS levels
may help in further defining of the role of TS regulation in drug
resistance. These correlations will need to be investigated for
applicability with the newer TS inhibitors.
The role of each of the numerous and diverse mechanisms
of TS regulation and resistance to TS inhibition remains to be
defined. It is not yet clear which factors predispose cells to
develop a certain resistance mechanism or which mechanism(s)
may at least in part account for the relatively low response rates
seen with ZD1694. However, the data presented above suggest
that TS inhibition alone may not be sufficient to result in
clinically significant cytotoxicity. A limited number of strategies (currently in preclinical development) attempting to improve the efficacy of TS inhibitors are presented briefly below.
Moreover, elucidation of intrinsic tumor properties pertinent to
altered signal transduction and metastatic potential (including
tumor-induced angiogenesis) may lead to new therapeutic strategies.
Improving Drug Efficacy. To counteract TS induction,
the development of an antisense RNA that targets the TS mRNA
sequences responsible for TS translation has been suggested
(126). In another approach using gene therapy, W1L2:R179
cells resistant to TS inhibitors through a 30-fold increase in TS
activity over that of their parental W1L2 cell line were transfected with the TS ribozyme using an EBV-based vector. This
hammerhead ribozyme cleaves the CUC sequences in a triple,
tandemly repeated sequence located in the 5' untranslated region of TS mRNA. Thus, the transfected cells became sensitive
to TS inhibitors (138). IFN-~/was shown to enhance the sensitivity of colon cancer ceils to 5-FU by interfering with acute TS
induction associated with 5-FU exposure and thus may prove to
have a role in dealing with this problem (123). Whether these
interventions will prove clinically useful in efforts to overcome
the increased TS mRNA translation noted with TS inhibition
requires further investigation. Alternatively, a 40-fold increase
in TS levels in normal cells as mentioned above could render
them theoretically more resistant to the TS inhibitor, thus resuiting in a host-protective effect, offering the possibility for
cell-selective treatment strategies.
Combining the inhibition of de novo and salvage pathways
of thymidylate synthesis can provide a synergistic effect. The
activity of salvage enzymes can be markedly higher than that of
the rate-limiting enzymes of de novo biosynthesis (139). AZT
inhibits TK, an enzyme that is up-regulated and involved in
salvage pathways of TS inhibition, effectively. Although AZT
alone did not inhibit TS, studies combining ZD1694 with AZT
in MGH-U1 human bladder cancer cells showed the combination to be more cytotoxic (140). Up-regulation of nucleoside
transporter may lead to increased uptake of preformed deoxythymidine or its analogue IdUrd in vitro (141). IdUrd alone did
not inhibit TS activity in MGH-U1 and HCT-8 cells. DNA
incorporation of this nucleoside analogue increased with administration of ZD1694 due to up-regulation of nucleoside transporter. IdUrd did not increase the TS inhibitory activity of
ZD1694, but its DNA incorporation resulted in an increase in
DNA single-strand breaks that paralleled cytotoxicity. Moreover, the therapeutic index was greater for the combination than
for either agent alone (141). Sequential combinations of 5-FU
and ZD1694 also have been tested for inhibition of salvage
pathways. Pretreatment of HCT-8 colon carcinoma cells with
ZD1694 was reported to enhance the cytotoxicity of 5-FU by
potentiating the efficacy of TS inhibition (142). Following cell
treatment with ZD1694, a strong TS inhibition leads to an
altered balance of dUMP and dTTP pools and allows for an
increased incorporation of 5-FU into RNA (2.5-3.0-fold that of
cells not exposed to ZD1694). This event has an immediate
effect on short-lived mRNAs (such as that of TK), leading to
cell death, and this approach potentiated the effect of ZD1694
on sensitive cell lines markedly (143). Plans are in development
to test this sequence-dependent synergistic combination in the
clinic. 4
Other strategies have focused simply on potentiating TS
inhibition or using agents synergistic with TS inhibitors. Because folate analogues bind to TS at a site different from that of
FdUMP, combining 5-FU with selective TS inhibitors could
potentiate the action of these agents. TS inhibition may be
enhanced by using both a dUMP and a folate analogue to
stabilize the TS-cofactor-substrate ternary complex. When
AG331 or polyglutamated ZD1694 was combined with 5-FU,
enhanced FdUMP binding to TS was observed. The ternary
complex consisting of TS, FdUMP, and AG337 or ZD1694 was
stable for at least 2 h. This led to potentiation of the growthinhibitory effect of 5-FU, AG337, or ZD1694 on colon cancer
cell lines (144).
In agreement with the above studies, a Phase I trial of
Tomudex in combination with 5-FU, folinic acid, and IFN-a for
recurrent adult solid tumors is currently underway (145).
Conclusion
Inhibition of TS results in a decrease of the de novo
thymidylate synthesis that is necessary for DNA synthesis and
repair. The development of ZD1694 is an example of a lengthy,
targeted approach to the design of new cancer chemotherapeutic
agents; ZD1694, a potent, selective TS inhibitor, has demonstrated antitumor effects in both preclinical and Phase II clinical
trials and is undergoing Phase III evaluation currently in the
United States. More detailed data from the European Phase III
trial in colorectal cancer will be available for critical review
soon. The outcome of these studies may contribute to more
convenient and less toxic alternatives to the currently available
chemotherapy for colorectal cancer. Newer antifolate compounds with diverse structures and properties designed and
developed by computer-assisted techniques are also undergoing
preclinical and clinical testing. However, given the limitations
posed by the variety of mechanisms through which cells bypass
TS inhibition, it is questionable whether each of these drugs will
be more successful than single-agent 5-FU or MTX. Combining
TS inhibitors with other cytotoxic agents, agents that interfere
with TS gene and mRNA regulation, or agents that inhibit
salvage mechanisms following thymidylate depletion may provide greater clinical utility of these new compounds.
4j. R. Bertino, personal communication.
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Clinical Cancer Research 239
Acknowledgments
We thank Diane Rivera for her assistance in preparing the manuscript and Y. Ishida for her assistance with the illustrations.
References
1. Ayusawa, D., Arai, H., Wataya, Y., and Sento, T. A specialized form
of chromosomal DNA degradation induced by thymidylate stress in
mouse FM3A cells. Mutat. Res., 200: 221-230, 1988.
2. Grem, J. L. Fluorinated pyrimidines. In: B. A. Chabner and J. M.
Collins (eds.), Cancer Chemotherapy: Principles and Practice, pp. 180224. Philadelphia: J. B. Lippincott Company, 1990.
3. Harrap, K. R., Jackman, A. L., Newell, D. R., Taylor, G. A., Hughes,
L. R., and Calvert, A. H. Thymidylate synthase: a target for anticancer
drug design. Adv. Enzyme Regul., 29: 161-179, 1989.
4. Roth, B., and Cheng, C. C. Recent progress in the medicinal chemistry of 2,4-diaminopyridines. Prog. Med. Chem., 19: 269-331, 1982.
5. Sirotnak, F. M., Burchall, J. J., Ensminer, W. D., and Montgomery,
J. A. Folate Antagonists as Therapeutic Agents, Vol. 1. Cambridge:
Academic Press, 1984.
6. Fischer, G. A. Defective transport of amethopterin (methotrexate) as
a mechanism of resistance to antimetabolites in L5178Y cells. Biochem.
Pharmacol., 11: 1233-1234, 1962.
7. Harrap, K. R., Hill, B. T., Furness, M. E., and Hart, L. I. Sites of
action of amethopterin in intrinsic and acquired drug resistance. Ann.
NY Acad. Sci., 186: 312-324, 1971.
8. Kessel, D., Hall, T. C., and Roberts, D. Modes of uptake of methotrexate by normal and leukemic human leukocytes in vitro and their
relation to drug response. Cancer Res. 28: 564-570, 1968.
9. Bertino, J. R., and Romanini, A. Chemotherapeutic agents: folate
antagonists. In: J. F. Holland, E. Frei III, R. C. Bast, Jr., D. W. Dufe, D.
Morton, and R. Weichselbaum (eds.), Cancer Medicine, Vol. 1, pp.
698-711. Philadelphia: Lea & Febiger, 1993.
10. Heidelberger, C. Fluorinated pyrimidines. Prog. Nucleic Acid Res.,
4: 1-50, 1965.
11. Heidelberger, C. Chemical carcinogenesis, chemotherapy: cancer's
continuing core challenges--G. H. A. Clowes Memorial Lecture. Cancer Res., 30: 1549-1569, 1970.
12. Schuetz, J. D., Wallace, H. J., and Diasui, R. B. 5-Fluorouracil
incorporation into DNA of CF- 1 mouse bone marrow cells as a possible
mechanism of toxicity. Cancer Res., 44: 1358-1363, 1984.
13. Peters, J. G., van Groeningen, C. J., Van der Wilt, C., Meijer, S.,
Smid, K., Laurensse, E., and Pinedo, H. M. Time course of inhibition of
thymidylate synthase in patients treated with fluorouracil and leucovorin. Semin. Oncol., 19 (2 Suppl. 3): 26-35, 1992.
14. Keyomarsi, K., and Moran, R. G. Folinic acid augmentation of the
effects of fluoropyrimidines on murine and human leukemic cells.
Cancer Res., 46: 5229-5235, 1986.
15. Johnston, P. G., Lenz, H. J., Leichman, C. G., Danenberg, K.,
Allegra, C. J., Danenberg, P., and Leichman, L. Thymidylate synthase
gene and protein expression correlate and are associated with response
to 5-fluorouracil in human colorectal and gastric tumors. Cancer Res.,
55: 1407-1412, 1995.
16. Johnston, P. G., Drake, J. C., Trepel, J., and Allegra, C. J. The
immunological quantitation of thymidylate synthase using the monoclonal antibody TS106 in 5-FU-sensitive and -resistant human cancer cell
lines. Cancer Res., 52: 4302-4312, 1992.
17. Peters, G. J., van der Wilt, C. L., van Groeningen, C. J., Smid, K.,
Meijer, S., and Pinedo, H. M. Thymidylate synthase inhibition after
administration of fluorouracil with or without leucovorin in colon cancer
patients: implications for treatment with fluorouracil. J. Clin. Oncol.,
12: 2035-2042, 1994.
18. Swain, S. M., Lippman, M. E., Egan, E. F., Drake, J. C., Steinberg,
S. M., and Allegra, C. J. Fluorouracil and high-dose leucovorin in
previously treated patients with metastatic breast cancer. J. Clin. Oncol.,
7: 890-899, 1989.
19. Johnston, P. G., Fisher, E. R., Rockette, H. E., Fisher, B., Wolmark,
N., Drake, J. C., Chabner, B. A., and Allegra, C. The role of thymidylate
synthase expression in prognosis and outcome of adjuvant chemotherapy in patients with rectal cancer. J. Clin. Oncol., 12: 2640-2647, 1994.
20. Jansen, G., Westerhof, G. R., Jarmuszewski, M. J., Kathmann, I.,
Rijksen, G., and Schornagel, J. H. Methotrexate transport in variant
human ccrf-cem leukemia cells with elevated levels of the reduced
folate carrier. Selective effect on carrier-mediated transport of physiological concentrations of reduced folates. J. Biol. Chem., 265: 1827218277, 1990.
21. Balinska, M., Galivan, J., and Coward, J. K. Effiux of methotrexate
and its polyglutamate derivatives from hepatic cells in vitro. Cancer
Res., 41: 2751-2756, 1981.
22. Hoffbrand, A. V., Tripp, E., Houlihan, C. M., and Scott, J. M.
Studies on the uptake of synthetic conjugated folates by human marrow
cells. Blood., 42: 141-146, 1973.
23. Calabresi, P., and Chabner, B. A. Antineoplastic agents. In: A.
Goodman Gilman, T. W. Rall, A. S. Nies, and P. Taylor (eds.), Goodman and Gilman's The Pharmacologic Basis of Therapeutics, pp. 12231227. New York: Pergamon Press, 1990.
24. Jackman, A. L., Marsham, P. R., Moran, R. G., Kimbell, R.,
O'Connor, B. M., Hughes, L. R., and Calvert, A. H. Thymidylate
synthase inhibitors: the in vitro activity of a series of heterocyclic
benzoyl ring modified 2-desamino-2-methyl-Nl°-substituted-5,8-didea zafolates. Adv. Enzyme Regul., 31: 13-27, 1991.
25. Hardy, L. W., Finer-Moore, J. S., Montfort, W. R., Jones, M. O.,
Santi, D. V., and Stroud, R. M. Atomic structure of thymidylate synthase: target for rational drug design. Science (Washington DC), 235:
448-455, 1987.
26. Matthews, D. A., Villafranca, J. E., Janson, C. A., Smith, W. W.,
Welsh, K., and Freer, S. Stereochemical mechanism of action for
thymidylate synthase based on the X-ray structure of the covalent
inhibitory ternary complex with 5-fluoro-2'-deoxyuridylate and 5,10methylenetetrahydrofolate. J. Mol. Biol., 214: 937-948, 1990.
27. Montfort, W. R., Perry, K. M., Fauman, E. C., Finer-Moore, J. S.,
Maley, G. F., Hardy, L., Maley, F., and Stroud, R. M. Structure, multiple
site binding, and segmental accommodation in thymidylate synthase on
binding dUMP and an anti-folate. Biochemistry, 29: 6964-6977, 1990.
28. Matthews, D. A., Appelt, K., Oatley, S. J., and Xuong, N. H. Crystal
structure of Escherichia coli thymidylate synthase containing bound
5-fluoro-2'-deoxyuridylate and 10-propargyl-5,8-dideazafotate. J. Mol.
Biol., 214: 923-936, 1990.
29. Appelt, K., Bacquet, F. J., Bartlett, C. A., Booth, C. L. J., and Freer,
S. T. Design of enzyme inhibitors using iterative protein crystallographic analysis. J. Med. Chem., 34: 1925-1934, 1991.
30. Kamb, A., Finer-Moore, J., Calvert, H., and Stroud, R. Structural
basis for recognition of polyglutamyl folates by thymidylate synthase.
Biochemistry, 31: 9883-9890, 1992.
31. Kamb, A., Finer-Moore, J. S., and Stroud, R. Cofactor triggers the
conformational change in thymidylate synthase: implications for an
ordered binding mechanism. Biochemistry, 31: 12876-12884, 1992.
32. Matthews, D. A., Appelt, K., and Oatley, S. J. Stacked [3-bulges in
thymidylate synthase account for a novel fight-handed rotation between
opposing [3 sheets. J. Mol. Biol., 205: 449-454, 1989.
33. Danenberg, K. D., and Danenberg, P. V. Evidence for a sequential
interaction of the subunits of thymidylate synthetase. J Biol Chem., 254:
4335-4348, 1979.
34. Stroud, R. M., and Finer-Moore, J. S. Stereochemistry of a multistep/bipartite methyl transfer reaction: thymidylate synthase. FASEB J.,
7: 671-677, 1993.
35. Dev, I. K., Dallas, W. S., Ferone, R., Hanlon, M., McKee, D. D.,
and Yates, B. B. Mode of binding of folate analogs to thymidylate
synthase. Evidence of two asymmetric but interactive substrate binding
sites. J. Biol. Chem., 269: 1873-1882, 1994.
36. Weichsel, A., Montfort, W., Ciesla, J., and Maley, F. Promotion of
purine nucleotide binding to thymidylate synthase by a potent folate
analogue inhibitor, 1843U89. Proc. Natl. Acad. Sci. USA, 92: 34933497, 1995.
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
240 Thymidylate Synthase Inhibitors
37. Pogolotti, A. L. J., Danenberg, P. V., and Santi, D. V. Kinetics and
mechanism of interaction of 10-propargyl-5,8-dideazafolate with thymidylate synthase. J. Med. Chem., 29: 478-482, 1986.
38. Santi, D. V., McHenry, C. S., Raines, R. T., and Ivanetich, K. M.
Kinetics and thermodynamics of the interaction of 5-fluoro-2'-deoxyuridylate with thymidylate synthase. Biochemistry, 26: 8606-8613, 1987.
39. Sikora, E., Newell, D. R., Jackman, A. J., Simmons, A. J., Jones,
T. R., and Calvert, A. H. Formation and retention and biological activity
of Nm-propargyl-5,8-dideazafolic acid (CB3717) polyglutamates in
L1210 cells in vitro. Biochem. Pharmacol., 37: 4047-4054, 1988.
40. Lu, Y-Z., Aiello, P. D., and Matthews, R. G. Studies on the
polyglutamate specificity of thymidylate synthase from fetal pig liver.
Biochemistry, 23: 6870-6876, 1984.
41. Jones, T. R., Calvert, A. H., Jackman, A. L., Brown, S. J., Jones, M.,
and Harrap, K. R. A potent antitumour quinazoline inhibitor of thymidylate synthase: synthesis, biological properties and therapeutic results
in mice. Eur. J. Cancer, 17: 11-19, 1981.
42. Jackman, A. L., Jodrell, D. I., Gibson, W., and Stephens, T. C. ICI
D1694, an inhibitor of thymidylate synthase for clinical study. In: R. A.
Harkness, G. B. Elion, and N. Zollner (eds.), Purine and Pyrimidine
Metabolism in Man, Vol. VII, Part A, pp. 19-23. New York: Plenum
Press, 1991.
43. Calvert, A. H., Newell, D. R., Jackman, A. L., Gumbrell, L. A.,
Sikora, E., Grzelakowska-Sztabert, B., Bishop, J. A. M., Judson, I. R.,
Harland, S., and Harrap, K. R. Recent preclinical and clinical studies
with the thymidylate synthase inhibitor Nl°-propargyl-5,8-dideazafolic
Acid (CB 3717). Natl. Cancer Inst. Monogr., 5: 213-218, 1987.
44. Jackson, R. C., Jackman, A. L., and Calvert, A. H. Biochemical
effects of a quinazoline inhibitor of thymidylate synthetase, CB3717, on
human lymphoblastoid cells. Biochem. Pharmacol., 32: 3783-3790,
1983.
45. Jackman, A. L., Taylor, G. A., Calvert, A. H., and Harrap, K. R.
Modulation of antimetabolite effects: effects of thymidine on the efficacy of the quinazoline-based thymidylate synthetase inhibitor, CB
3717. Biochem. Pharmacol., 33: 3269-3275, 1984.
46. Newell, D. R., Alison, D. L., Calvert, A. H., Harrap, K. R., Jarman,
M. J., Jones, T. R., Manteuffel-Cymborowska, M., and O'Connor P.
Pharmacokinetics of the thymidylate synthase inhibitor Nl°-propargyl 5,8-dideazafolic acid (CB3717) in the mouse. Cancer Treat. Rep., 70:
971-979, 1986.
47. Jodrell, D. I., Newell, D. R., Morgan, S. E., Clinton, S., Bensted,
J. P. M., Hughes, L. R., and Calvert, A. H. The renal effects of
Nl°propargyl-5,8-dideazafolic acid (CB3717) and a non-nephrotoxic
analogue, ICI D1694, in mice. Br. J. Cancer, 64: 833-838, 1991.
48. Calvert, A. H., Alison, D. L., Harland, S. J., Robinson, B. A.,
Jackman, A. L., Jones, T. R., Newell, D. R., Siddik, Z. H., Wiltshaw, E.,
McElwain, T., Smith, I., and Harrap, K. A Phase I evaluation of the
quinazoline antifolate thymidylate synthase inhibitor, Nl°-propargyl 5,8-dideazafolic acid, CB 3717. J. Clin. Oncol., 4: 1245-1252, 1986.
49. Vest, S., Bork, E., and Hansen, H. H. A Phase I evaluation of
Nm-propargyl 5,8-dideazafolic acid. Eur. J. Cancer & Clin. Oncol., 24:
201-204, 1988.
50. Sessa, C., Zucchetti, M., Ginier, M., Willems, Y., D'Incalci, M.,
and Cavalli, F. Phase I study of the antifolate Nm-propargyl-5,8-didea zafolic acid, CB3717. Eur. J. Cancer & Clin. Oncol., 24: 769-775,
1988.
51. Cantwell, B. M. J., Macaulay, V., Harris, A. L., Kaye, S. B., Smith,
I. E., Milsted, R. A., and Calvert, A. H. Phase II study of the antifolate
Nm-propargyl-5,8-dideazafolic acid (CB3717) in advanced breast cancer. Eur. J. Cancer & Clin. Oncol., 24: 733-736, 1988.
52. Bassendine, M. F., Curtin, N. J., Loose, H., Harris, A. L., and
James, O. F. Induction of remission in hepatocellular carcinoma with a
new thymidylate synthase inhibitor CB 3717: a Phase II study. J.
Hepatol., 4: 349-356, 1987.
53. Newell, D. R., Siddik, Z. H., Calvert, A. H., Jackman, A. L., Alison,
D. L., McGhee, G. K., and Harrap, K. R. Pharmacokinetics and toxicity
studies with CB3717. Proc. Am. Assoc. Cancer Res., 23: 181, 1982.
54. Marsham, P. R., Hughes, L. R., Jackman, A. L., Hayter, A. J.,
Oldfield, J., Wardleworth, J. M., Bishop, J. A. M., O'Connor, B. M., and
Calvert, A. H. Quinazoline antifolate thymidylate synthase inhibitors:
heterocyclic benzoyl ring modifications. J. Med. Chem., 34: 15941605, 1991.
55. Jackman, A. L., Taylor, G. A., Bishop, J. A., O'Connor, B. M.,
Bisset, G., Hughes, L. R., Moran, R. G., and Calvert, A. Biochemical
aspects of a new thymidylate synthase inhibitor, D1694. Proc. Am.
Assoc. Cancer Res., 31: 342, 1990.
56. Jackman, A. L., Taylor, G. A., Gibson, W., Kimbell, R., Brown, M.,
Calvert, A. H., Judson, I. R., and Hughes, L. R. ICI D1694, a quinazoline antifolate thymidylate synthase inhibitor that is a potent inhibitor of
L 1210 tumor cell growth in vitro and in vivo: a new agent for clinical
study. Cancer Res., 51: 5579-5586, 1991.
57. Erlichman, C., and Mitrovski, B. Biochemical effects of D1694
inhibition of thymidylate synthase in MGH-UI bladder cancer cells.
Proc. Am. Assoc. Cancer Res., 33: 507, 1992.
58. A_rredondo, M. A., Guimaraes, M. A., Yin, M. B., Slocum, H. K.,
and Rustum, Y. M. Prolonged cell cycle phase perturbation induced by
the quinazoline antifolate thymidylate synthase inhibitor ICI D1694.
Proc. Am. Assoc. Cancer Res., 33: 428, 1992.
59. Kelland, L. R., Abel, G., Brown, M., and Jackman, A. L. Cytotoxicity of ICI D 1694 and cisplatin in sensitive and acquired resistant
tumor cell lines. Br. J. Cancer, 65 (Suppl. 16): 64, 1992.
60. Zhang, Z. G., Yin, M. B., and Rustum, Y. M. Cytotoxicity, DNA
strand breaks, thymidylate synthase inhibition and methylenetetrahydrofolate pool decrease induced by ICI D 1694. Proc. Am. Assoc. Cancer
Res., 33: 410, 1992.
61. Matsui, S., Lu, K., Wrzosek, C., and Rustum, Y. Double-strand
DNA damage induced by thymidylate synthase (TS) inhibitor, ZD1694,
in human colon carcinoma cell, HCT-8, requires DNA replication. Proc.
Am. Assoc. Cancer Res., 36: 378, 1995.
62. Stephens, T. C., Calvete, J. A., Janes, D., Waterman, S. E., Valcaccia, B. E., Hughes, L. R., and Calvert, A. H. Antitumor activity of a
new thymidylate synthase (TS) inhibitor, D1694. Proc. Am. Assoc.
Cancer Res., 31: 342, 1990.
63. Jodrell, D. I., Newell, D. R., Calvete, J. A., Stephens, T. C., and
Calvert, A. H. Pharmacokinetic and toxicity studies with the novel
quinazoline thymidylate synthase (TS) inhibitor, D1694. Proc. Am.
Assoc. Cancer Res., 31: 341, 1990.
64. Stephens, T. C., Valcaccia, B. E., Sheader, M. L., Hughes, L., and
Jackman, A. L. The thymidylate synthase (TS) inhibitor ICI D 1694 is
superior to CB3717, 5-fluorouracil (5-FU) and methotrexate (MTX)
against a panel of human tumor xenografts. Proc. Am. Assoc. Cancer
Res., 32: 328, 1991.
65. Jackman, A. L., Farrugia, D. C., Clarke, S. J., Aherne, G. W., Boyle,
F. T., Seymour, L., Azab, M., and Kennealey, G. Delayed rescue of
ZD1694 toxicity in BALB/c mice with thymidine (dThd) or leucovorin
(LV). Proc. Am. Assoc. Cancer Res., 36: 377, 1995.
66. Aherne, G. W., Farrugia, D. C., Ward, E., Sutcliffe, F., and Jackman, A. L. ZD1694 (Tomudex) and polyglutamate levels in mouse
plasma and tissues measured by radioimmunoassay (RIA) and the effect
of leucovorin (LV). Proc. Am. Assoc. Cancer Res., 36: 376, 1995.
67. The International Medical Function. Tomudex (ZD1694), a Thymidylate Synthase Inhibitor: Clinical Investigator's Manual. Macclesfield,
United Kingdom: Zeneca Pharmaceuticals, 1994.
68. Jodrell, D. I., Newell, D. R., Gibson, W., Hughes, L. R., and
Calvert, A. H. The pharmacokinetics of the quinazoline antifolate ICI D
1694 in mice and rats. Cancer Chemother. Pharmacol., 28: 331-338,
1991.
69. Jackman, A. L., and Gibson, W. Polyglutamation of the thymidylate
synthase (TS) inhibitor, ZD1694 (Tomudex), in normal mouse tissues.
Proc. Am. Assoc. Cancer Res., 36: 377, 1995.
70. Judson, I., Clarke, S., Ward, J., Sutcliffe, F., Planting, A., Spiers, J.,
Smith, R., Verweij, J., and Judson, I. Pharmacokinetics of ICI D1694
following a 15-minute infusion in patients with advanced cancer. Proc.
Am. Soc. Clin. Oncol. Annu. Meet., 11: 117, 1992.
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Clinical Cancer Research 241
71. Clarke, S. J., Ward, J., Tierney, K., Walker, M., Sutcliffe, F.,
Planting, A., Verweij, J., Spiers, J., Smith, R., and Judson, I. Phase I and
pharmacokinetic study of ICI D1694: a folate-based thymidylate synthase (TS) inhibitor. Ann. Oncol., 3 (Suppl. 1): 135, 1992.
72. Clarke, S. J., Ward, J., Planting, A., Spiers, J., Smith, R., Verweij,
J., and Judson, I. Phase I trial of ICI D 1694: a novel thymidylate
synthase inhibitor. Proc. Am. Assoc. Cancer Res., 33: 406, 1992.
73. Clarke, S. J., Jackman, A. L., and Judson, I. R. The toxicity of ICI
D1694 in man and mouse. Adv. Exp. Med. Biol., 338: 601-604, 1993.
74. Clarke, S. J., Ward, J., De Boer, M., Planting, A., Verweij, J.,
Sutcliffe, F., Azab, M., and Judson, I. Phase I study of the new
thymidylate synthase inhibitor "Tomudex" (ZD1694) in patients with
advanced malignancy. Ann. Oncol., 5 (Suppl. 5): 132, 1994.
75. Sorensen, J. M., Jordan, D., Grem, J. L., Hamilton, J. M., Arbuck,
S. G., Johnson, P., Kohler, D. R., Goldspiel, B. R., and Allegra, C. J.
Phase I trial of D1694, a pure thymidylate synthase inhibitor. Proc. Am.
Soc. Clin. Oncol., 12: 158, 1993.
76. Sorensen, J. M., Jordan, E., Grem, J. L., Arbuck, S. G., Chen, A. P.,
Hamilton, J. M., Johnson, P., Kohler, D., Goldspiel, B., and Allegra, C.
Phase I trial of ZD1694 ("Tomudex") a direct inhibitor of thymidylate
synthase. Ann. Oncol., 5 (Suppl. 5): 132, 1994.
77. Gore, M., Earl, H., Cassidy, J., Tattersal, M., Mansi, J., and Azab,
M. Phase II study of "Tomudex" (ZD1694), a new thymidylate synthase inhibitor with antitumour activity in breast cancer. Ann. Oncol., 5
(Suppl. 5): 132, 1994.
78. Smith, I. E., Spielmann, M., Bonneterre, J., Namer, M., Green, M.,
Wander, H. E., Toussaint, C., and Azab, M. "Tomudex" (ZD1694), a
new thymidylate synthase inhibitor ZD1694 in advanced breast cancer.
Ann. Oncol., 5 (Suppl. 5): 132, 1994.
79. Smith, I. E., Spielmann, M., Namer, M., Bonneterre, J., Wander,
H. E., Green, M., Lowery, K., and Azab, M. Antitumour activity of a
new thymidylate synthase inhibitor ZD1694 in advanced breast cancer.
Breast Cancer Res. Treat., 27: 149, 1993.
80. Zalcberg, J., Cunningham, D., Banc Custsem, E., Francois, J. E.,
Schornagel, J. H., Adenis, A., Green, M., Starkhammer, H., and Azab,
M. Good antitumour activity of the new thymidylate synthase inhibitor
"Tomudex" (ZD1694) in colorectal cancer. Ann. Oncol., 5 (Suppl. 5):
133, 1994.
81. Pazdur, R., Casper, E. S., Meropol, N. J., Fuchs, C., and Kennealey,
G. T. Phase II trial of "Tomudex" (ZD1694), a thymidylate synthase
inhibitor in advanced pancreatic cancer. Proc. Am. Soc. Clin. Oncol. 13:
207, 1994.
82. Gore, M., Earl, H., Cassidy, J., Tattersal, M., Mansi, J., and Azab,
M. Phase II study of Tomudex (ZD1694) in refractory ovarian cancer
Ann. Oncol., 5 (Suppl. 5): 133, 1994.
83. Burris, H. I., Von Hoff, D., Bowen, K., Heaven, R., Rinaldi, D.,
Eckardt, J., Campbell, L., Robert, F., Patton, S., and Kennealey, G. A
Phase II trial of ZD1694, a novel thymidylate synthase inhibitor, in
patients with advanced non-small cell lung cancer. Ann. Oncol., 5
(Suppl. 5): 133, 1994.
84. Cunningham, D., Zalcberg, J., Francois, E., Van Cutsem, J. H.,
Ellis, P., and Azab, M. Tomudex (ZD1694), a new thymidylate synthase
inhibitor with good antitumor activity in advanced colorectal cancer
(ACC). Proc. Am. Soc. Clin. Oncol., 13: 199, 1994.
85. Piedbois, P., Buyse, M., Rustum, Y., Machover, D., Erlichman, C.,
Carlson, R. W., Valone, F., Labianca, R., Doroshow, J. H., and Petrelli,
N. for the Advanced Colorectal Cancer Meta-Analysis Project. Modulation of fluorouracil by leucovorin in patients with advanced colorectal
cancer: evidence in terms of response rate. J. Clin. Oncol., 10: 896-903,
1992.
86. Poon, M. A., O'Connel, J. H., Wieland, H. S., Krook, J. E.,
Gerstner, J. B., Tschetter, L. K., Levitt, R., Kardinal, C. G., and
Maillard, J. A. Biochemical modulation of fluorouracil with leucovorin:
confirmatory evidence of improved therapeutic efficacy in advanced
colorectal cancer. J. Clin. Oncol., 9: 1967-1972, 1991.
87. Jackman, A. L., Aherne, G., Kimbell, R., Brunton, L., Hardcastle,
A., Wardleworth, J. W., Stephens, T. C., and Boyle, F. ZD9331, a
non-polyglutamatable quinazoline thymidylate synthase (TS) inhibitor.
Proc. Am. Assoc. Cancer Res., 35: 301, 1994.
88. Walton, M. I., Gibson, W., Aherne, L., Lawrence, N., Stephens, T.,
Smith, M., and Jackman, A. Pharmacokinetics of the potent non-polyglutamatable thymidylate synthase inhibitors CB30900 and ZD9331 in
mice. Proc. Am. Assoc. Cancer Res., 35: 301, 1994.
89. Stephens, T. C., Smith, M. N., McClockey, M. L., and Boyle, F. T.
ZD9331, a novel non-polyglutamated thymidylate synthase (TS) inhibitor: in vivo antitumor efficacy and toxicity to normal murine tissues.
Proc. Am. Assoc. Cancer Res., 35: 305, 1994.
90. Pendergast, W., Dickerson, S. H., Johnson, J. V., Dev, I. K., Ferone,
R., Duch, D. S., Hall, W. R., Humphreys, J., Kelly, I. M., and Wilson,
D. C. Benzoquinazoline inhibitors of thymidylate synthase: enzyme
inhibitory activity and cytotoxicity of some 3-amino and 3-methylbenzo[f]quinazolin-l(2H)-ones. J. Med. Chem., 36: 2279-2291, 1993.
91. Duch, D. S., Banks, S., Dev, I. K., Dickerson, S. H., Ferone, R.,
Heath, L. S., Humphreys, J., Knick, V., Pendergast, W., Singer, S.,
Smith, G., Waters, K., and Wilson, R. Biochemical and cellular pharmacology of 1849U89, a novel benzoquinazoline inhibitor of thymidylate synthase. Cancer Res., 53: 810-818, 1993.
92. Ferone, R., Hanlon, M. H., Waters, K. A., and Dev, I. K. Influence
of intracellular polyglutamation on the cytotoxicity of the thymidylate
synthase inhibitor 1843U89. Proc. Am. Assoc. Cancer Res., 34: 274,
1993.
93. Banks, S. D., Waters, K. A., Barrett, L. L., Dickerson, S., Pendergast, W., and Smith, G. K. Destruction of WiDr multicellular tumor
spheroids with the novel thymidylate synthase inhibitor 1843U89. Cancer Chemother. Pharmacol., 36: 455-459, 1994.
94. Wilson, H. R., Heath, L. S., Knick, V. C., Kszalka, G. W., and
Ferone, R. In vivo antitumor activity of 1843U89, a new antifolate
thymidylate synthase inhibitor. Proc. Am. Assoc. Cancer Res., 33: 407,
1992.
95. Boyd, M. R., and Paull, K. D. Some practical considerations and
applications of the National Cancer Institute in vitro anticancer drug
discovery screen. Drug Dev. Res., 34: 91-109, 1995.
96. Jackson, R. C., Johnston, A. L., Shetty, B. V., Varney, M. D.,
and Webber, S. E. Molecular design of thymidylate synthase inhibitors.
Proc. Am. Assoc. Cancer Res., 34: 566-567, 1993.
97. Varney, M. D., Marzone, G. H. P., Palmer, C. L., Reddy, M. R.,
Tatlock, J., Romines, W. H., Wu, B. W., and Musick, L. Crystalstructure-based design and synthesis of benz[od]indole-containing inhibitors of thymidylate synthase. J. Med. Chem., 35: 663-676, 1992.
98. Reich, S. H., Fuhry, M. A. M., Nguyen, D., Pint, M. J., Welsh,
K. M., Webber, S., Janson, C. A., Jordan, S. R., Matthews, D. A., Smith,
W., and Bartlett, C. Design and synthesis of novel 6,7-imidazotetrahydroquinoline inhibitors of thymidylate synthase using iterative protein
crystal structure analysis. J. Med. Chem., 35: 847-858, 1992.
99. Webber, S., Shetty, B., Johnston, A., Welsh, K., Varney, M., Deal,
J., Morse, C., and Soda, K. In vitro properties and antitumor activity of
AG-331, a novel lipophilic thymidylate synthase inhibitor. Proc. Am.
Assoc. Cancer Res., 33: 413, 1992.
100. Webber, S., Johnston, A., Shetty, B., Webber, S. E., Welsh, K.,
Hilliard, J., Kosa, M., Morse, C., and Soda, K. Preclinical studies on
AG337, a novel lipophilic thymidylate synthase inhibitor. Proc. Am.
Assoc. Cancer Res., 34: 273, 1993.
101. Boritzki, T. J., Bartlett, C. A., Huffaker, T., Morse, C. A., Webber,
S., Welsh, K., and Jackson, R. C. Biochemical properties of new
lipophilic thymidylate synthase inhibitors designed from the X-ray
structure of the E. coli enzyme. Proc. Am. Assoc. Cancer Res., 33: 33,
1992.
102. Clendeninn, N. J., Peterkin, J. J., Webber, S., Shetty, B. V., Koda,
R. T., Leichman, L., Leichman, C. G., Jeffers, S., Muggia, F., and
O'Dwyer, P. AG-331, a "non-classical" lipophilic thymidylate synthase inhibitor for the treatment of solid tumors Ann. Oncol., 5 (Suppl.
5): 133, 1994.
103. Calvete, J. A., Balmanno, K., Taylor, G. A., Raft, I., Newell, D. R.,
Lind, M. J., Calvert, A. H., Webber, S., and Clendeninn, N. J. Preclinical
and clinical studies of prolonged administration of the novel thymidylate
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
242 Thymidylate Synthase Inhibitors
synthase inhibitor, AG337. Proc. Am. Assoc. Cancer Res., 35: 306,
1994.
104. Calvete, J. A., Balmanno, K., Raft, I., Newell, D. R., Taylor, G. A.,
Boddy, A. V., Lind, M. J., Bailey, N. B., Calvert, A. H., Webber, S., and
Clendeninn, N. J. Preclinical and clinical studies of the novel thymidylate synthase inhibitor AG337, given by oral administration. Proc. Am.
Assoc. Cancer Res., 36: 380, 1995.
105. Raft, I., Taylor, G. A., Balmanno, K., Calvete, J. A., Newell, D. R.,
Lind, M. J., and Calvert, A. H. A Phase I study of the novel antifolate
3,4-dihydro-2-amino-6-methyl-4-oxo-5-(4-pyridylthio)-quinazolone dihydrochloride (AG337) given by a 24 h intravenous continuous infusion. Proc. Am. Assoc. Cancer Res., 35: 306, 1994.
106. Johnson, P. Agouron Initiates Phase II Efficacy Trials of AntiTumor Drug AG337. La Jolla, CA: Agouron Pharmaceuticals, Inc.,
1994.
107. Boddy, A. V., Calvete, J. A., and Raft, I. Non-linear pharmacokinetics in cancer patients of AG337, a rationally-designed thymidylate
synthase (TS) inhibitor. Proc. Am. Assoc. Cancer Res., 36: 236, 1995.
108. Raft, I., Taylor, G. A., Calvete, J. A., Balmanno, K., Boddy, A. V.,
Bailey, N. B., Lind, M. J., Newell, D., Calvert, A. H., Johnston, A., and
Clendeninn, N. J. A Phase I clinical study of the novel antifolate AG337
given by a 5-day continuous infusion. Proc. Am. Assoc. Cancer Res.,
36: 240, 1995.
109. Koda, R. T., Leichman, L., Webber, S., Shetty, B. V., Leichman,
C. G., Jeffers, S., and Muggia, F. M. Pharmacokinetics of AG-331
following single escalating i.v. doses in patients with refractory solid
tumors. Proc. Am. Assoc. Cancer Res., 35: 432, 1994.
110. O'Connor, B. M., Webber, S., Jackson, R. C., Galivan, J., and
Rhee, M. S. Biological activity of a novel rationally designed lipophilic
thymidylate synthase inhibitor. Cancer Chemother. Pharmacol., 34:
225-229, 1994.
111. Jackman, A. L., Kelland, L. R., Brown, M., Gibson, W., Kimbell,
R., Aherne, W., and Judson, I. R. ICI D 1694 resistant cell lines. Proc.
Am. Assoc. Cancer Res., 33: 406, 1992.
112. Freemantle, S. J., Lunec, J., Jackman, A. L., Kelland, L. R.,
Aheme, G. W., and Calvert, A. H. Molecular characterisation of three
cell lines selected for resistance to folate-based thymidylate synthase
inhibitors. Br. J. Cancer, 67 (Suppl. 20): 79, 1993.
113. Berger, S. H., Jenh, C. H., Johnson, L. F., and Berger, F. G.
Thymidylate synthase overproduction and gene amplification in fluorodeoxyuridine-resistant human cells. Mol. Pharmacol., 28: 461-467,
1987.
114. Cowan, K. H., and Jolivet, J. A methotrexate-resistant human
breast cancer cell line with multiple defects including diminished formation of methotrexate polyglutamates. J. Biol. Chem., 259: 107931O8O0, 1984.
115. Rosowsky, A., Wright, J. E., Cucchi, C. A., Lippke, J. A., Tantravahi, R., Ervin, T. J., and Frei, E. III. Phenotypic heterogeneity in
cultured human ~aead and neck squamous cell carcinoma lines with
low-level methotrexate resistance. Cancer Res., 45: 6205-6212, 1985.
116. Pizzorno, G., Mini, E., Coronnello, M., McGuire, J. J., Moroson,
J. B. A., Cashmore, A. R., Dreyer, R. N., Lin, J. T., Mazzei, T., Periti,
P., and Bertino, J. Impaired polyglutamylation of methotrexate as a
cause of resistance in CCRF-CEM cells after short-term, high dose
treatment with this drug. Cancer Res., 48: 2149-2155, 1988.
117. Shih, C., Grindey, G. B., Barnett, C. J., Pearce, H. L., Engelhardt,
J. A., Todd, G. C., Rinzel, S. M., Worzalla, J. F., Gossett, L. S., and
Everson, T. P. Structure-activity relationship studies of novel pyrrolopyrimidine antifolate LY231514. Proc. Am. Assoc. Cancer Res., 33:
411, 1992.
118. Grindey, G. B., Shih, C., Barnett, C. J., Pearce, H. L., Engelhardt,
J. A., Todd, G. C., Rinzel, S. M., Worzalla, J. F., Gossett, L. S., and
Everson, T. P. LY231514, a novel pyrrolopyrimidine antifolate that
inhibits thymidylate synthase (TS). Proc. Am. Assoc. Cancer Res., 33:
411, 1992.
119. Rinaldi, D. A., Burris, H. A., Dorr, F. A., Nelson, J., Fields, S. M.,
Kuhn, J. G., Eckardt, J., Lu, P., Woodworth, J. R., and Corso, S. W. A
Phase I evaluation of the novel thymidylate synthase inhibitor,
LY231514, in patients with advanced solid tumors. Proc. Am. Soc. Clin.
Oncol., 13: 430, 1994.
120. Taylor, G. A., Raft, I., Balmanno, K., Calvete, J. A., Newell, D. R.,
Webber, S., Jackson, R. C., Gumbrell, L., Chapman, F., and Oakey, A.
Preclinical and early clinical studies with the lipophilic thymidylate
synthase inhibitor, AG337. Br. J. Cancer., 67 (Suppl. XX): 17, 1993.
121. Chu, E., Voeller, D., Koeller, D. M., Drake, J. C., Takimoto, C. H.,
Maley, G., Maley, F., and Allegra, C. J. Identification of an RNA
binding site for human thymidylate synthase. Proc. Natl. Acad. Sci.
USA, 90: 517-521, 1993.
122. Chu, E., Koeller, D. M., Casy, L. J., Drake, C. J., Chabner, B. A.,
Elwood, P. C., Zinn, S., and Allegra, C. J. Autoregulation of human
thymidylate synthase messenger RNA translation by thymidylate synthase. Proc. Natl. Acad. Sci. USA, 88: 8977-8981, 1991.
123. Chu, E., Zinn, S., Boarman, D., and Allegra, C. J. The interaction
of interferon-~ and 5-fluorouracil in the H630 human colon carcinoma
cell line. Cancer Res., 50: 5834-5840, 1990.
124. Spears, C. P., Shahinian, A. H., Moran, R. G., Heidelberger, C.,
and Corbett, T. H. In vivo kinetics of thymidylate synthetase inhibition
of 5-fluorouracil-sensitive and resistant murine colon adenocarcinomas.
Cancer Res., 42: 450-456, 1982.
125. Keyomarsi, D., and Moran, R. G. Mechanism of the cytotoxic
synergism of fluoropyrimidines and folinic acid in mouse leukemic
cells. J. Biol. Chem., 263: 14402-14409, 1988.
126. Keyomarsi, K., Samet, J., Molnar, G., and Pardee, A. B. The
thymidylate synthase inhibitor ICI D 1694 overcomes translational
detainment of the enzyme. J. Biol. Chem., 268:15132-15149, 1993.
127. Keyomarsi, K., Molnar, G., and Pardee, A. B. Loss of translational
control of thymidylate synthase (TS) by antifolates results in the accumulation of the TS protein. Proc. Am. Assoc. Cancer Res., 34: 276,
1993.
128. Lowe, S. W., Ruley, H. E., Jacks, T., and Housman, D. E. p53dependent apoptosis modulates the cytotoxicity of anticancer agents.
Cell, 74: 957-967, 1993.
129. Lowe, S. W., Bodis, S., McClathcey, A., Remington, L., Ruley,
H. E., Fisher, D. E., Housman, D. E., and Jacks, T. p53 status and the
efficacy of cancer therapy in vivo. Science (Washington DC), 266:
807-810, 1994.
130. Oltvai, Z. N., and Korsmeyer, S. J. Checkpoints of dueling dimers
foil death wishes. Cell, 79: 189-192, 1994.
131. Starzynska, T., Bromley, M., Ghosh, A., and Stern, P. L. Prognostic significance of p53 overexpression in gastric and colorectal
carcinoma. Br. J. Cancer, 66: 558-562, 1992.
132. Thompson, C. B. Apoptosis in the pathogenesis and treatment of
disease. Science (Washington DC), 267." 1456-1462, 1995.
133. Chu, E., Takechi, T., Jones, K. L., Voeller, D. M., Copur, S. M.,
Maley, G. F., Maley, F., Segal, S., and Allegra, C. J. Thymidylate
synthase binds to c-myc RNA in human colon cancer cells and in vitro.
Mol. Cell. Pharmacol., 15: 179-185, 1995.
134. Chu, E., Copur, S., Jones, K. L., Khleif, S., Voeller, D., Maley,
G. F., Maley, F., and Allegra, C. J. Thymidylate synthase regulates the
translation of p53 mRNA. Proc. Am. Assoc. Cancer Res., 36: 563, 1995.
135. Arredondo, M. A., Yin, M. B., Lu, K., Schrber, C., Slocum, H.,
and Rustum, Y. M. Decreased c-myc protein accompanied by increased
p53 and Rb is associated with thymidylate synthase inhibition and cell
cycle retardation induced by D1694. Proc. Am. Assoc. Cancer Res., 35:
304, 1994.
136. Fisher, T. C., Milner, A. E., Gregory, C. D., Jackman, A. L.,
Aherne, G. W., Hartley, J. A., Dive, C., and Hickman, J. A. bcl-2
modulation of apoptosis induced by anticancer drugs: resistance to
thymidylate stress is independent of classical resistance pathways. Cancer Res., 53: 3321-3326, 1993.
137. Lenz, H. J., Ju, J. F., Danenberg, K. D., Leichman, L., Leichman,
C., Haag, C., and Danenberg, P. V. TS levels and p53 function predict
for response to 5-fluorouracil/leucovorin in patients with advanced
colon cancer. Proc. Am. Soc. Clin. Oncol., 14: 202, 1995.
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Clinical Cancer Research 243
138. Kobayashi, H., Takemura, Y., Miyachi, H., Skelton, L., and Jackman, A. L. The effect of hammerhead ribozyme against thymidylate
synthase on the cytotoxicity of thymidylate synthase inhibitor. Proc.
Am. Assoc. Cancer Res., 36: 342, 1995.
139. Weber, G., and Prajda, N. Targeted and non-targeted actions of
anti-cancer drugs. Adv. Enzyme Regul., 34: 71-89, 1994.
140. Pressacco, J., and Erlichman, C. Combination studies with 3'azido-deoxythymidine (AZT) plus ICI D1694. Cytotoxic and biochemical effects. Biochem. Pharmacol., 46: 1989-1997, 1993.
141. Pressacco, J., Hedley, D. W., and Erlichman, C. ICI D1694 and
idoxuridine: a synergistic antitumor combination. Cancer Res., 54:
3772-3778, 1994.
142. Chang, Y. M., Zielinski, Z., Izzo, J., Porubcin, M., and Bertino,
J. R. Pretreatment of colon carcinoma cells to D1694 (Tomudex) mark-
edly enhances 5-fluorouracil cytotoxicity. Proc. Am. Assoc. Cancer
Res., 35: 330, 1994.
143. Izzo, J., Zielinski, Z., Chang, Y. M., and Bertino, J. R. Molecular
mechanisms of the synergistic sequential administration of D1694 (Tomudex) followed by FUra in colon carcinoma cells. Proc. Am. Assoc.
Cancer Res., 36: 381, 1995.
144. Van der Wilt, C. L., Pinedo, H. M., Kuiper, C. M., Smid, K., and
Peters, G. J. Biochemical basis for the the combined antiproliferative
effect of AG337 or ZD1694 and 5-fluorouracil. Proc. Am. Assoc.
Cancer Res., 36: 379, 1995.
145. National Cancer Institute PDQ. Phase I study of Tomudex in
combination with 5-FU/CF/IFN-A for recurrent adult solid tumors including gastrointestinal, breast, lung, and ovarian carcinomas. Curr.
Clin. Trials Oncol., 2: 749, 1995.
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.
Thymidylate synthase inhibitors.
N Touroutoglou and R Pazdur
Clin Cancer Res 1996;2:227-243.
Updated version
E-mail alerts
Reprints and
Subscriptions
Permissions
Access the most recent version of this article at:
http://clincancerres.aacrjournals.org/content/2/2/227
Sign up to receive free email-alerts related to this article or journal.
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Department at [email protected].
To request permission to re-use all or part of this article, contact the AACR Publications
Department at [email protected].
Downloaded from clincancerres.aacrjournals.org on May 14, 2017. © 1996 American Association for Cancer
Research.