Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
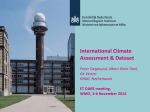
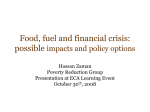
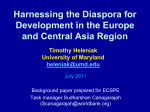
Assessment of the Contribution of the External Carotid Artery to Brain Perfusion in Patients With Internal Carotid Artery Occlusion Peter Jan van Laar, MD, PhD; Jeroen van der Grond, PhD; Jochem P. Bremmer, MD; Catharina J.M. Klijn, MD, PhD; Jeroen Hendrikse, MD, PhD Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 Background and Purpose—The purpose of this study was to prospectively investigate the contribution of the ipsilateral external carotid artery (ECA) to cerebral perfusion in patients with internal carotid artery occlusion. Methods—Institutional Review Board approval and informed consent were obtained. Thirty functionally independent patients (24 men, 6 women; mean age, 63 years) with an angiographically proven unilateral internal carotid artery occlusion and transient or minor disabling ischemic attacks ipsilateral to the side of the internal carotid artery occlusion were included. Grading of ECA collateral flow was performed with intraarterial digital subtraction angiography. The contribution of the ECA to regional cerebral blood flow was assessed with selective arterial spin labeling MRI. Differences in regional cerebral blood flow were analyzed with Student t test. Results—Twenty percent of the patients had ECA Grade 0 collateral flow (no filling of ophthalmic artery), 20% Grade 1 (filling of carotid siphon), and 60% Grade 2 (filling of anterior and/or middle cerebral artery) as demonstrated on digital subtraction angiography. Although in the Grade 1 group, the ECA supplied a smaller region of the brain compared with the Grade 2 group, the mean regional cerebral blood flow of the perfusion territory supplied by the ECA is similar (P⫽0.70) in the Grade 1 group (mean⫾SD 57⫾16 mL/min/100 g) and the Grade 2 group (60⫾12 mL/min/100g). Conclusion—In patients with symptomatic internal carotid artery occlusion, focal brain regions may strongly depend on the contribution to cerebral perfusion of the ECA ipsilateral to the side of the internal carotid artery occlusion, even in patients with limited ECA collateral supply as demonstrated on digital subtraction angiography. (Stroke. 2008;39:3003-3008.) Key Words: carotid artery occlusion 䡲 cerebral hemodynamics 䡲 collateral circulation 䡲 magnetic resonance imaging I n patients with symptomatic internal carotid artery (ICA) occlusion, collateral pathways are used to compensate for diminished blood flow.1 These collaterals include the connections through the circle of Willis, the connections arising from leptomeningeal anastomoses on the brain surface, and the extracranial-to-intracranial collaterals, most often through the ipsilateral external carotid (ECA) artery and the ophthalmic artery.2 The results of several studies in patients with occlusive disease of the ICA have demonstrated that presence of ECA collateral flow may prevent the development of failure of the brain’s blood supply.3,4 In contrast, findings from one study showed no beneficial effect of ECA collateral flow,5 and findings from other studies showed that the presence of collateral circulation through the ECA was associated with hemodynamic impairment.6,7 The actual contribution of the individual collateral pathways is difficult to assess and to quantify. Magnetic reso- nance angiography and transcranial Doppler may show the presence of collateral flow, but they do not show the actual contribution to brain perfusion.3– 6 Intraarterial digital subtraction angiography (DSA) offers more information and shows also the distal arteries of the collateral pathway.7–9 However, to visualize all the collateral pathways, this technique requires an invasive, selective 3-vessel approach (ie, both the common carotid arteries, and the vertebrobasilar arteries [VBA]). Recently, selective arterial spin labeling (ASL) MRI was introduced as a method to assess the contribution of individual arteries to the perfusion of the brain.10 The aim of the present study was to investigate the contribution of the ipsilateral ECA to cerebral perfusion in patients with ICA occlusion. We hypothesized that patients with higher grades of ECA collateral flow on DSA show a larger ECA flow territory and a reduced regional cerebral blood flow (rCBF) with selective ASL MRI. Received January 6, 2008; final revision received March 26, 2008; accepted March 27, 2008. From the Departments of Radiology (P.J.v.L, J.v.d.G., J.H.) and Neurology (J.P.B., C.J.M.K.), University Medical Center Utrecht, Utrecht, The Netherlands; the Department of Radiology (P.J.v.L.), Meander Medical Center Amersfoort, Amersfoort, The Netherlands; and the Department of Radiology (J.v.d.G.), Leiden University Medical Center, Leiden, The Netherlands. Correspondence to Peter Jan van Laar, MD, PhD, University Medical Center Utrecht, Department of Radiology, PO Box 85500, 3508 GA Utrecht, The Netherlands. E-mail [email protected] © 2008 American Heart Association, Inc. Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.108.514265 3003 3004 Stroke November 2008 Figure 1. Intracranial anteroposterior (AP) and lateral (LAT) views of selective angiograms of the common carotid artery on the side of the ICA occlusion in 3 patients, demonstrating the degree of collateral flow from the ipsilateral ECA on the side of the ICA occlusion. ECA Grade 0, no filling of ophthalmic artery; ECA Grade 1, retrograde flow in ophthalmic artery with filling of carotid siphon; ECA Grade 2, to MCA and/or ACA. Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 Methods The ethics committee of our institution approved the study protocol, and written informed consent was obtained from all participants. Patients Thirty consecutive patients (24 men and 6 women; mean age, 63 years ⫾10 SD) who met our study criteria were included between June 2004 and December 2006. All patients had transient or minor disabling ischemic attacks (modified Rankin score 0 to 3) within 6 months before referral ipsilateral to the side of the ICA occlusion. Patients who had experienced a severe stroke in the past that caused major disability (modified Rankin score 3 to 5) were not included.11 All patients had an angiographically proven unilateral proximal ICA occlusion. Intraarterial Digital Substraction Angiography To assess the presence of ECA collateral pathways, biplane (anteroposterior and lateral) DSA intracranial views were examined. After a selective common carotid artery injection on the side of the ICA occlusion, ECA collaterals were recognized on the angiogram by the contrast filling of the ECA, ophthalmic artery, carotid siphon, middle cerebral artery (MCA), or anterior cerebral artery (ACA). The appearance of the ECA collaterals was then graded on a 3-point scale9: 0, slight collateral distribution, often with dilution (eg, no filling of ophthalmic artery); 1, small but definite collateral supply (eg, retrograde flow in ophthalmic artery with filling of carotid siphon); or 2, full collateral filling (eg, to MCA and/or ACA; Figure 1). Grading of ECA obstruction was performed with DSA. The mean degree of stenosis in the ipsilateral ECA was 23% (⫾31% SD). Four (13%) of 30 patients had an ECA stenosis of 70% or greater. MRI MRI was performed using a 1.5-T or 3.0-T whole-body system (Philips Medical Systems, Best, The Netherlands). Thirteen patients were scanned on 1.5 T and 17 patients on 3.0 T. Perfusion territory imaging of the ipsilateral ECA and the other brain feeding arteries (contralateral ICA and VBA) was achieved by using a regional perfusion imaging sequence,10 which is based on a pulsed ASL transfer insensitive labeling technique.12–14 An optimized sequence has been used for selective ASL at 3.0 T, which has shown to have a high labeling efficiency at 3.0 T.15 With regional perfusion imaging, selective labeling is obtained by using the sharp labeling profiles of the transfer insensitive labeling technique pulses16 and by interactively planning the spatially selective inversion slabs to invert the targeted artery only. Subsequent to the labeling pulses, 3 90° saturation pulses followed by strong dephasing gradients were applied on the imaging sections to remove the direct effect of the labeling pulses. Each saturation pulse was followed by a series of strong dephasing gradients in all 3 directions to spoil all remaining transverse magnetization. In the present study, no vascular crushers were used. Planning of the selective labeling volume was performed on the basis of transversal source images of the time-of-flight MR angiography of the brain feeding arteries (Figure 2). Five imaging sections were planned parallel to the orbitomeatal angle and were acquired in the cranial to caudal direction with a delay time of 25 ms between sections. The labeling delay time (inversion time) was set at 1600 ms. For image acquisition, a single-shot echoplanar imaging readout was used. Other MR parameters for regional perfusion imaging were 3000/5.6 repetition time ms/echo time ms (1.5 T); 4000/23 repetition time ms/echo time ms (3.0 T); 62% partial Fourier acquisition; 8-mm slice thickness; 1-mm section gap; 240⫻240-mm field of view; 64⫻64 matrix; zero filling to a 128⫻128 matrix; 30 signals acquired at 1.5 T and 20 signals acquired at 3.0 T; regional perfusion imaging scan time 3 minutes per territory at 1.5 T; and 2 minutes 40 seconds per territory at 3.0 T. Four ASL acquisitions were performed for each patient: selective ASL measurements of the ECA, the contralateral ICA, and the VBA and an acquisition at multiple TI to quantify the rCBF of the ECA. Figure 2. Planning of the selective arterial spin labeling MRI slabs in a patient with a left-sided ICA occlusion for perfusion territory imaging of the left ECA, right nonoccluded ICA, and VBA. The labeling slabs are planned based on the transverse source images of the time-offlight MR angiography of the brainfeeding arteries (TR, 23; TE, 3.5; 18° flip angle). van Laar et al Contribution of ECA to Brain Perfusion 3005 Figure 3. Transverse segmented perfusion territory maps of the ECA ipsilateral to the ICA occlusion, the nonoccluded contralateral unilateral ICA, and VBA in all patients with ICA occlusion. Colors correspond to the color bar, which indicates the percentage of patients who demonstrated perfusion in that region of the brain: 100% (red color) indicates that all subjects demonstrated perfusion in that region; 50% (green color) indicates that half of the subjects demonstrated perfusion in that region; 3.3% (violet color) indicates that one subject demonstrated perfusion in that region; 0% (no overlaid color) indicates the region of the brain that none of the subjects demonstrated perfusion. Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 To quantify the contribution of the ipsilateral ECA to the rCBF (in milliliters per minute per 100 g tissue), a multi-inversion time selective ASL sequence was used. Five imaging sections were planned parallel to the orbitomeatal angle. For selective ASL at multiple inversion times, the detection part of the regional perfusion imaging pulse sequence10 was replaced by a series of 13 excitation pulses (flip angles of 35°) with increasing delay times from 200 ms to 2600 ms with a constant interval of 200 ms followed by single-shot gradient echoplanar imaging readout.17 rate of blood)⫽0.71 s⫺1 (1.5 T) or 0.61 s⫺1 (3.0 T); (brain/blood partition coefficient of water)⫽0.9 mL/g.10,15,22 Statistical Analysis Difference in mean rCBF between the Grade 1 group and the Grade 2 group was analyzed with Student t test. A probability value of ⬍0.05 was considered to indicate a significant difference. For statistical analysis, SPSS for Windows, version 10.0.7 was used. Results Data Processing The postprocessing method (segmentation and registration) has been described and illustrated in detail previously.18 In brief, data were analyzed using MATLAB (Mathworks, Natick, Mass). Perfusionweighted images of the flow territories of the selectively labeled arteries were obtained by subtraction of the labeled from the control images. After visual evaluation of the resulting subtracted images, one of the authors (P.J.v.L.; 5 years of experience) manually outlined and filled the perfusion images. A single experienced user performed the analysis of the extent of the flow territories, thus eliminating any interobserver variability. The segmented images were registered on a standard brain (SPM, Wellcome Department of Cognitive Neurology, Institute of Neurology, London, UK).19 Absence of ECA flow was assessed by the absence of perfusion signal on the selective ASL images of the ECA. This process was performed for all flow territories of all subjects. Because no significant differences in perfusion territories were found between patients with left-sided ICA occlusion and those with right-sided ICA occlusion, all patients with ICA occlusions were pooled. The perfusion territory maps of patients with left-sided ICA occlusion were mirrored in the midline, whereas perfusion territory maps of patients with right-sided symptomatic ICA occlusion remained unchanged. To create groups, the flow territories (registered on the standard brain) from the individual subjects were combined. These combined flow territory maps were color-coded and expressed as probability maps: 100% (region of the brain with red color) indicates that all subjects demonstrated perfusion in that region; and 0% (region of the brain without overlaid color) indicates the region of the brain that no subject demonstrated perfusion. For rCBF quantification, one author (P.J.v.L.) selected regionsof-interest that enclosed the brain perfusion territory of the ECA closely. For region-of-interest selection in patients with ECA Grade 0 collateral flow (eg, no filling of ophthalmic artery on DSA), the entire brain area was used as a “control perfusion mask” to extract rCBF number from the whole brain. For the drawing of the regions-of-interest on the selective ASL images, these images have been windowed at the same level. Quantification was performed on the basis of established kinetic perfusion models20,21 with the following values for the physical constants: ␣ (efficiency of the inversions pulse)⫽1.0; R1 (longitudinal relaxation rate of tissue)⫽1.0 s⫺1 (1.5 T) or 1.2 s⫺1 (3.0 T); R1a (longitudinal relaxation Perfusion Territories The segmented perfusion territory maps of the ECA, the contralateral ICA, and the VBA for all patients with unilateral ICA occlusion (n⫽30) showed a relatively large variation in perfusion territories (Figure 3). An example of representative images of a 62-year-old patient with transient ischemic attacks associated with a right-sided ICA occlusion shows the ECA collateral pathways on DSA and the ASL MRI perfusion territories of the ECA on the side of the occlusion, the left-sided nonoccluded ICA, and the VBA (Figure 4). Six (20%) of 30 patients with unilateral ICA occlusion had ECA Grade 0 collateral flow, 6 (20%) patients had ECA Grade 1 collateral flow, and 18 (60%) patients had ECA Grade 2 collateral flow as demonstrated on DSA. Subcategories of patients with ECA Grade 0, Grade 1, and Grade 2 showed considerably lower variation in perfusion territories of the ECA ipsilateral to the side of the ICA occlusion compared with the group as a whole (Figure 5). The perfusion territory maps in patients with ECA Grade 0 demonstrated that the ECA in these patients did not contribute to the cerebral perfusion. In patients with Grade 1, the ECA supplied a focal region of the ipsilateral MCA territory, and in patients with Grade 2, the ECA supplied the MCA and, to a lesser extent, the ACA perfusion territory ipsilateral to the side of the occlusion. Regional Cerebral Blood Flow Although the brain region that is supplied by the ECA is larger in the Grade 2 group than in the Grade 1 group, the mean rCBF of the brain perfusion territory supplied by the ECA showed no significant difference (P⫽0.70) in rCBF between the Grade 1 group (57⫾16 mL/min/100 g) and the 3006 Stroke November 2008 Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 Figure 4. Top, Intracranial anteroposterior (AP) and lateral (LAT) views of the selective angiogram of the common carotid artery on the side of the ICA occlusion in a 62-year-old patient with transient ischemic attacks associated with a right-sided ICA occlusion demonstrating Grade 2 ECA collateral flow: filling to MCA and ACA. Bottom, Transverse arterial spin labeling MRI perfusion territory images in the same patient (TR, 3000; TE, 5.6; TI, 1600 ms, 90° flip angle). When the ECA on the side of the ICA occlusion was labeled selectively, perfusion signal was observed in the right MCA territory. When labeling the left-sided nonoccluded ICA, signal was detected in the left MCA territory and in both the left and right ACA territories. The perfusion territory of the VBA supplied the posterior part of the imaging slices and extended into the MCA territory ipsilateral to the side of the ICA occlusion. Red line, outline of segmented ECA perfusion territory images. Grade 2 group (60⫾12 mL/min/100 g). The mean rCBF of the entire brain in the ECA Grade 0 group was 5⫾13 mL/min/100 g. Discussion Our study in patients with symptomatic unilateral ICA occlusion demonstrated that although the brain region that is supplied by the ECA is larger in the Grade 2 group than in the Grade 1 group, the mean rCBF of the perfusion territory supplied by the ECA is not significantly different between both groups. The ipsilateral ECA can be an important extracranial-tointracranial collateral in patients with symptomatic ICA occlusion.2 In our study, 24 (80%) of 30 patients with unilateral ICA occlusion had retrograde, collateral flow in the ophthalmic artery ipsilateral to the side of the occlusion on DSA. In previous studies of patients with unilateral ICA occlusion, researchers demonstrated that the percentage of Figure 5. Transverse segmented perfusion territory maps of the ECA in patients with unilateral ICA occlusion. Colors correspond to the color bar, which indicates the percentage of patients who demonstrated perfusion in that region of the brain. van Laar et al Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 patients with retrograde flow in the ophthalmic artery varied between 36% and 89%.3,5,7,8,23 The inclusion of patients who had no major neurological deficit may explain the relative high prevalence of collateral flow in the ophthalmic artery in our study. Thus far, the extent of the contribution of the ipsilateral ECA to cerebral perfusion in patients with symptomatic ICA occlusion has remained unclear. The presence of collateral flow through the ECA as assessed with transcranial Doppler has been associated with relatively preserved cerebral hemodynamics.3,4 Other studies have found contradicting results and showed that the presence of ECA collateral pathways assessed with DSA or transcranial Doppler was associated with impaired cerebral hemodynamic measurements.6,7 In these studies, collateral supply through the ECA was only assessed as present or absent and could not be quantified as is possible by the method we have presented in this study. This may explain the discrepant findings of either favorable or impaired cerebral hemodynamics with presence of ECA collateral flow. The results of previous postmortem and in vivo studies have shown large variability in perfusion territories of the major brain-feeding arteries (ICA and VBA) in healthy subjects and in patients with carotid occlusive disease.18,24,25 In this light, it is not surprising that our results show a considerable variation in individual ECA territorial distribution. Because we examined patients with ICA occlusion who had no major neurological deficit, collateral pathways are expected to exist in these patients to reroute blood to compensate for absent ipsilateral ICA flow, thereby resulting in altered territorial supply. To our knowledge, our study is the first to actually show the extent of the altered ECA perfusion territories in patients with ICA occlusion. In the past decade, numerous selective ASL methods have been developed to image the perfusion territories of individual brain-feeding arteries. Selective ASL techniques have been introduced to assess the perfusion territories of the individual common carotid arteries,26 –28 the individual ICAs, and the VBA.10,29 –32 Although selective ASL could potentially detect certain boundary areas that are shared between the ECA and the other arteries, these boundary areas with combined perfusion were not observed in the present study. Other selective ASL methods have enabled perfusion territory mapping of intracranial arteries such as the ACA and MCA.31,33 Thus far, no method was presented to selectively label the ECA. The combination of ICA occlusion and the selective ASL method enabled us to perform perfusion territory mapping of the ECA ipsilateral to the side of the occlusion. Currently, DSA is the standard for visualizing the cerebral vascular tree and for assessing collateral flow at the level of the circle of Willis or leptomeningeal anastomoses at the brain surface. DSA offers excellent information on the presence of collateral flow, showing also the distal arteries of a collateral pathway. However, DSA does not provide quantitative information on the actual perfusion of the brain, and to visualize all the collateral pathways, this technique requires an invasive, selective multivessel approach. In the future, selective ASL MRI may be capable of replacing diagnostic DSA in a selected group of patients. For instance, in patients Contribution of ECA to Brain Perfusion 3007 with a severe stenosis of an ECA ipsilateral to an ICA occlusion, knowledge of the actual contribution of the ECA to cerebral perfusion as assessed by ASL MRI may help to select patients who may benefit most from endarterectomy of the ipsilateral ECA.34 A limitation of our study may be that perfusion territory segmentation was performed at a single delay time between labeling and imaging. In general, this delay time is sufficient for adequate exchange of the label with the brain. However, with severe obstruction of the main brain-feeding arteries, and subsequent presence of collateral flow, labeled blood may have delayed arrival at the brain tissue. This may result in an underestimation of the flow territory. However, a previous study in patients with ICA occlusion demonstrated that a delay time of 1600 ms (used in our study) is a good tradeoff between signal-to-noise ratio, washout of the tracer, and T1 relaxation.35 Similar to the quantification of rCBF with nonselective ASL MRI, rCBF quantification in patients with ICA occlusion requires more advanced selective ASL techniques.35 With delayed collateral flow, the label will have a delayed arrival at the brain tissue and ASL techniques with measurements at a single time point may suffer from underestimation of the rCBF in the areas with collateral blood supply. Acquiring images at multiple time points as we did in our study can prevent underestimation of rCBF. In addition to ASL at multiple time points, several methods have been developed to render ASL MRI relatively insensitive to transit delays by applying saturation pulses to obtain sharply defined and a uniform shape of the bolus profile.36,37 In the present study, we had a relatively small sample size. The number of patients might have been too small to demonstrate potential small differences in rCBF between ECA Grade 1 and 2 groups. With selective ASL, there may be some contamination of arteries from other vascular territories. When labeling the VBA, the curved anatomy of the ICA in the neck will incidentally lead to superfluous labeling of the proximal ICAs. This artifactual residual labeling of the ICAs will however be very small.10 With respect to the selective labeling of the ECA on the side of an occluded ICA, the selective labeling of the ECA will be easily separated from the other brain-feeding arteries in the neck, and no artifactual labeling of other arteries will occur. For selective ASL methods, the labeling efficiency may be lower than 1.0 both for both 1.5 and 3.0 T due to partial labeling of the proximal arterial tree to the angulation of the labeling slab. This means that we might have slightly underestimated the extent of the flow territories. Furthermore, although ASL MRI rCBF measurements are highly comparable with rCBF measurements obtained with positron emission tomography,38 ASL is well known to yield slightly overestimated rCBF values in the gray matter owing to the presence of label in the vasculature.39 In conclusion, we showed that in patients with symptomatic ICA occlusion, focal brain regions may strongly depend on the contribution to cerebral perfusion of the ECA ipsilateral to the side of the ICA occlusion, even in patients with limited ECA collateral supply as demonstrated on DSA. The actual contribution of the ECA as assessed by ASL MRI 3008 Stroke November 2008 could be taken into account when considering vascular intervention of an ECA stenosis in patients with symptomatic ICA occlusion. Sources of Funding C.J.M.K. is supported by a clinical fellowship from the Netherlands Organization for Health Research and Development (grant 907– 00103) and by The Netherlands Heart Foundation (grant 2003B263). Disclosures None. References Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 1. Powers WJ. Cerebral hemodynamics in ischemic cerebrovascular disease. Ann Neurol. 1991;29:231–240. 2. Liebeskind DS. Collateral circulation. Stroke. 2003;34:2279 –2284. 3. van Everdingen KJ, Visser GH, Klijn CJM, Kappelle LJ, van der Grond J. Role of collateral flow on cerebral hemodynamics in patients with unilateral internal carotid artery occlusion. Ann Neurol. 1998;44: 167–176. 4. Vernieri F, Pasqualetti P, Matteis M, Passarelli F, Troisi E, Rossini PM, Caltagirone C, Silvestrini M. Effect of collateral blood flow and cerebral vasomotor reactivity on the outcome of carotid artery occlusion. Stroke. 2001;32:1552–1558. 5. Mead GE, Wardlaw JM, Lewis SC, Dennis MS. No evidence that severity of stroke in internal carotid occlusion is related to collateral arteries. J Neurol Neurosurg Psychiatry. 2006;77:729 –733. 6. Muller M, Schimrigk K. Vasomotor reactivity and pattern of collateral blood flow in severe occlusive carotid artery disease. Stroke. 1996;27: 296 –299. 7. Yamauchi H, Kudoh T, Sugimoto K, Takahashi M, Kishibe Y, Okazawa H. Pattern of collaterals, type of infarcts, and haemodynamic impairment in carotid artery occlusion. J Neurol Neurosurg Psychiatry. 2004;75: 1697–1701. 8. Rutgers DR, Klijn CJ, Kappelle LJ, van der Grond J. Recurrent stroke in patients with symptomatic carotid artery occlusion is associated with high-volume flow to the brain and increased collateral circulation. Stroke. 2004;35:1345–1349. 9. Henderson RD, Eliasziw M, Fox AJ, Rothwell PM, Barnett HJM. Angiographically defined collateral circulation and risk of stroke in patients with severe carotid artery stenosis. Stroke. 2000;31:128 –132. 10. Hendrikse J, van der Grond J, Lu H, van Zijl PC, Golay X. Flow territory mapping of the cerebral arteries with regional perfusion MRI. Stroke. 2004;35:882– 887. 11. Bamford JM, Sandercock PAG, Warlow CP, Slattery J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1989;20:828. 12. Golay X, Stuber M, Pruessmann KP, Meier D, Boesiger P. Transfer insensitive labeling technique (TILT): application to multislice functional perfusion imaging. J Magn Reson Imaging. 1999;9:454 – 461. 13. Calamante F, Thomas DL, Pell GS, Wiersma J, Turner R. Measuring cerebral blood flow using magnetic resonance imaging techniques. J Cereb Blood Flow Metab. 1999;19:701–735. 14. Barbier EL, Lamalle L, Decorps M. Methodology of brain perfusion imaging. J Magn Reson Imaging. 2001;13:496 –520. 15. Petersen ET, Lim T, Golay X. Model-free arterial spin labeling quantification approach for perfusion MRI. Magn Res Med. 2006;55L219 –232. 16. Pruessmann KP, Golay X, Stuber M, Scheidegger MB, Boesiger P. RF pulse concatenation for spatially selective inversion. J Magn Reson. 2000;146:58 – 65. 17. Hendrikse J, Lu H, van der Grond J, van Zijl PC, Golay X. Measurements of cerebral perfusion and arterial hemodynamics during visual stimulation using TURBO-TILT. Magn Reson Med. 2003;50:429 – 433. 18. van Laar PJ, Hendrikse J, Klijn CJ, Kappelle LJ, van Osch MJ, van der Grond J. Symptomatic carotid artery occlusion: flow territories of major brain-feeding arteries. Radiology. 2007;242:526 –534. 19. Ashburner J, Friston KJ. Voxel-based morphometry—the methods. Neuroimage. 2000;11:805– 821. 20. Buxton RB, Frank LR, Wong EC, Siewert B, Warach S, Edelman RR. A general kinetic model for quantitative perfusion imaging with arterial spin labeling. Magn Reson Med. 1998;40:383–396. 21. Gunther M, Bock M, Schad LR. Arterial spin labeling in combination with a look-locker sampling strategy: inflow turbo-sampling EPI-FAIR (ITS-FAIR). Magn Reson Med. 2001;46:974 –984. 22. Lu H, Clingman C, Golay X, van Zijl PC. Determining the longitudinal relaxation time (T1) of blood at 3.0 Tesla. Magn Reson Med. 2004;52: 679 – 682. 23. Rutgers DR, Klijn CJM, Kappelle LJ, van Huffelen AC, van der Grond J. A longitudinal study of collateral flow patterns in the circle of Willis and the ophthalmic artery in patients with a symptomatic internal carotid artery occlusion. Stroke. 2000;31:1913–1920. 24. van der Zwan A, Hillen B, Tulleken CAF, Dujovny M, Dragovic L. Variability of the territories of the major cerebral arteries. J Neurosurg. 1992;77:927–940. 25. van Laar PJ, Hendrikse J, Golay X, Lu H, van Osch MJ, van der Grond J. In vivo flow territory mapping of major brain feeding arteries. Neuroimage. 2006;29:136 –144. 26. Zhang W, Silva AC, Williams DS, Koretsky AP. NMR measurement of perfusion using arterial spin labeling without saturation of macromolecular spins. Magn Reson Med. 1995;33:370 –376. 27. Zaharchuk G, Ledden PJ, Kwong KK, Reese TG, Rosen BR, Wald LL. Multislice perfusion and perfusion territory imaging in humans with separate label and image coils. Magn Reson Med. 1999;41:1093–1098. 28. Trampel R, Mildner T, Goerke U, Schaefer A, Driesel W, Norris DG. Continuous arterial spin labeling using a local magnetic field gradient coil. Magn Reson Med. 2002;48:543–546. 29. Wong EC. Vessel encoded arterial spin labeling using pseudo-continuous tagging. Magn Reson Med. 2007;58:1086 –1091. 30. Davies NP, Jezzard P. Selective arterial spin labeling (SASL): perfusion territory mapping of selected feeding arteries tagged using twodimensional radiofrequency pulses. Magn Reson Med. 2003;49: 1133–1142. 31. Werner R, Norris DG, Alfke K, Mehdorn HM, Jansen O. Continuous artery-selective spin labeling (CASSL). Magn Reson Med. 2005;53: 1006 –1012. 32. Golay X, Petersen ET, Hui F. Pulsed star labeling of arterial regions (PULSAR): a robust regional perfusion technique for high field imaging. Magn Reson Med. 2005;53:15–21. 33. Taoka T, Iwasaki S, Nakagawa H, Nakagawa H, Fukusumi A, Hirohashi S, Sakmoto M, Kichikawa K, Murata K. Distinguishing between anterior cerebral artery and middle cerebral artery perfusion by color-coded perfusion direction mapping with arterial spin labeling. AJNR Am J Neuroradiol. 2004;25:248 –251. 34. Klijn CJM, Kappelle LJ, Tulleken CAF, van Gijn J. Symptomatic carotid artery occlusion. A reappraisal of hemodynamic factors. Stroke. 1997;28: 2084 –2093. 35. Hendrikse J, van Osch MJ, Rutgers DR, Bakker CJ, Kappelle LJ, Golay X, van der Grond J. Internal carotid artery occlusion assessed at pulsed arterial spin-labeling perfusion MR imaging at multiple delay times. Radiology. 2004;233:899 –904. 36. Wong EC, Buxton RB, Frank LR. A theoretical and experimental comparison of continuous and pulsed arterial spin labeling techniques for quantitative perfusion imaging. Magn Reson Med. 1998;40:348 –355. 37. Luh WM, Wong EC, Bandettini PA, Hyde JS. QUIPSS II with thin-slice TI1 periodic saturation: a method for improving accuracy of quantitative perfusion imaging using pulsed arterial spin labeling. Magn Reson Med. 1999;41:1246 –1254. 38. Ye FQ, Berman KF, Ellmore T, Esposito G, van Horn JD, Yang Y, Duyn J, Smith AM, Frank JA, Weinberger DR, McLaughlin AC. H(2)(15)O PET validation of steady-state arterial spin tagging cerebral blood flow measurements in humans. Magn Reson Med. 2000;44:450 – 456. 39. Ye FQ, Mattay VS, Jezzard P, Frank JA, Weinberger DR, McLaughlin AC. Correction for vascular artifacts in cerebral blood flow values measured by using arterial spin tagging techniques. Magn Reson Med. 1997;37:226 –235. Assessment of the Contribution of the External Carotid Artery to Brain Perfusion in Patients With Internal Carotid Artery Occlusion Peter Jan van Laar, Jeroen van der Grond, Jochem P. Bremmer, Catharina J.M. Klijn and Jeroen Hendrikse Downloaded from http://stroke.ahajournals.org/ by guest on April 29, 2017 Stroke. 2008;39:3003-3008; originally published online August 7, 2008; doi: 10.1161/STROKEAHA.108.514265 Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2008 American Heart Association, Inc. All rights reserved. Print ISSN: 0039-2499. Online ISSN: 1524-4628 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://stroke.ahajournals.org/content/39/11/3003 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Stroke is online at: http://stroke.ahajournals.org//subscriptions/