Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
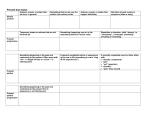
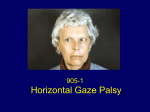
A Case of Progressive Supranuclear Palsy Lauren Maloney, O.D. 4435 N Greenview #1W Chicago, IL 60640 [email protected] Abstract: Recalcitrant to pharmacologic therapy progressive supranuclear palsy, first described in 1964 by Steele, Richardson and Olszewski, presents usually in the seventh decade with parkinsonian-like signs, psuedobulbar signs and extraocular movement abnormalities.2 Initially mis-diagnosed, before being seen at the Veterans Administration medical center, as alcohol related this case with differential diagnosis and video will be discussed. Key words: progressive supranuclear palsy, ocular manifestations Case Report: Patient SJ is a 57-year-old African American male that presented to our clinic on June 25th, 2007 with complaints of blurred vision OU at all distances and an inability to move his eyes vertically over the last eighteen months. He also had reportedly been falling more frequently, which was attributed to his blurred vision. The patient was being followed for glaucoma at an outside hospital and was seen there recently. His past social history is pertinent for 30 years of alcohol abuse, recently discontinued about 6 months prior to his presentation. His past ocular history is pertinent for open angle glaucoma OU. His past medical history is pertinent for moderate dementia attributed to his history of alcohol abuse and a history of a mild CVA confirmed by MRI. His current medications include Travatan 0.004% ophthalmic solution and Timolol 0.5% ophthalmic solution. His uncorrected visual acuity was 20/60 OD and OS at distance with a pinhole acuity of 20/40 OD and OS. He is noted to have significant fluctuations in acuity during exam. Best-corrected visual acuity is unchanged with a manifest refraction of pl -0.50 x087 OD and +0.25-1.50x083 OS. He is noted to have significant difficulty with subjective refraction OU. Pupils were equally round and reactive without afferent pupillary defect OU. Confrontation fields were full to finger counting OU. Extraocular movements were intact in horizontal gazes but he was unable to voluntarily move his eyes vertically. However vertical gaze was intact by oculocephalic maneuvers. Color vision testing was unreliable. The patient was noted to have a blank stare secondary to eyelid retraction and decreased blink rate. Anterior segment evaluation by slit lamp examination revealed clear eyelids and lashes OU; a quiet palpebral and bulbar conjunctiva OU; clear cornea OU with an oily tear film OU and a deep and quiet anterior chamber OU. Intraocular pressures were measured at 18 mmHg OD and 20 mmHg OS by Goldman applanation tonometry. The patient was dilated with one drop 1% Mydriacil and one drop 2.5% Phenylephrine OU. Dilated fundus exam subsequently performed by slit lamp examination revealed trace nuclear sclerosis of the lens OU. Fundus assessment with a 78 diopter lens revealed pink and distinct optic nerve heads with a cup to disc ratio of 0.6/0.6 OD and 0.8/0.8 OS. Maculae had mild retinal pigment changes OU. The retinal vasculature and vitreous were within normal limits OU. The peripheral retinal examination by binocular indirect ophthalmoscopy with a 20 diopter lens was grossly flat and intact but limited due to patient cooperation. During the course of the examination the patient was noted to have a right hand tremor and a hypererect gait as well as an overall rigidity to his movements. The differential diagnoses considered in this case include: -Wernicke-Korsakoff Syndrome -Wernicke-Korsakoff syndrome can present with weakness or paralysis of the lateral rectus and conjugate gaze, nystagmus, and a wide based short stepped gait.5 - Parkinson’s syndrome Parkinson’s syndrome can present with problems with impairment of upgaze, convergence insufficiency, visual sensory disturbances and a simian stature.3 - Dorsal midbrain syndrome Dorsal midbrain syndrome can present with impairment of upgaze, convergence retraction nystagmus, and light near dissociation.4 - Progressive supranuclear palsy (PSP) Progressive supranuclear palsy presents with impairment of downgaze first then impairment of upgaze, and a hypererect gait.2 There was no evidence of light near dissociation or convergence retraction nystagmus. Therefore the patient was diagnosed with oculomotor apraxia, scheduled an MRI and asked to return for neuroophthalmology conference. Follow-up #1: The patient returned on August 1st, 2007 for neuroophthalmology conference. His visual acuity was reduced to 10/140 OD and 10/160 OS with the Designs For Vision chart. The patient’s pupils were equal round and reactive to light without afferent pupillary defect. His extraocular movements were unchanged. The MRI ordered was not yet completed. At this exam the patient’s rigidity, gait and tremor were more fully evaluated. Upon questioning of his spouse he was noted to frequently fall backward while ambulating. Therefore a diagnosis of progressive supranuclear palsy was made. At this point it was decided that a referral to neurology was necessary to evaluate if dopamine agonist therapy to modulate his symptoms was warranted. Discussion: Steele, Richardson and Olszewski first described progressive supranuclear palsy in 1964. It is characterized as a disorder that begins after the age of 55, usually in the seventh decade with parkinsonian-like signs, pseudobulbar signs and extraocular movement abnormalities.2 It has an incidence of 5.3 per 100,000 people but most patients are symptomatic for 3.9 years before the diagnosis is made.7 The pathogenesis of progressive nuclear palsy begins with atrophy of the midbrain and, to a lesser extent, the pons. This atrophy is characterized by neuronal loss, gliosis and neurofibrillary tangles that affect the basal ganglia, diencephalon and brainstem.1 The neuronal and glial inclusions are characterized by microtubule associated tau protein classifying the disorder as a tauopathy. 3 Contrasted with alzeihemer’s disease, amlyoid deposits and neuritic plaques are notably absent. 6 The following is a comparision of the signs found in progressive supranuclear palsy: Parkinson’s PSP DorsalWienickeMidbrain Korsakoff Syndrome Syndrome Bradykinesia X X Postural Instability X-falls X-falls 7 forward backward Axial Rigidity X X Dysarthria X X Dysphagia X Pseudobulbar X confabulations8 Affect Supranuclear usually X upgaze horizontal gaze 7 4 Gaze Palsy upgaze only only paralysis-not supranuclear8 Eyelid Retraction X X Apraxia of Eyelid X X Opening/Closing Square Wave only in 18% X 7 Jerks/ of patients Cogwheel Pursuits The parkinsonian-like signs in PSP significantly differ from Parkinson’s syndrome in the lack of asymmetry in their presentation. Also motor difficulty in PSP tends to involve the axial musculature; neck muscles are more affected than trunk muscles.6 Patients will subjectively complain of blurred vision, eye irritation and photophobia; all likely related to dry eye, secondary to decreased blink rate. Less commonly patients will complain of diplopia, but unrelated to the motility problems. This is also likely due to dry eyes.2 Late in the course of the disease horizontal gaze abnormalities may develop.6 While this disease is a progressive condition, it is typically recalcitrant to pharmacological intervention. Isolated reports of improvement of symptoms after treatment with Traxodone, Idazoxan, Methysergide, L-theo-DOPS, and Amitriptyline have been reported in the literature but have yet to be proven effective.6 Dopamine agonists may provide limited symptomatic improvement, but it is the nature of the condition to be fatal 6-10 years after its onset.5 Falls during the first year, early dysphagia and incontinence are poor prognostic indicators. 6 The causes of death are usually infections and pulmonary complications related to immobility.6 Conclusion: Progressive supranuclear palsy is a rare neurologic condition that often goes undiagnosed and/or misdiagnosed early in the course of the disorder. The ocular complaints and concomitant oculomotor signs that essentially define this disorder make it a necessary part of any differential diagnosis of vertical gaze palsy. The key finding in this disease to complete the diagnosis is the history of backward falls. While nothing can resolve the extraocular muscle abnormalities, it is important for clinicians to realize that they can recognize a clinical entity that may aid patients and their families with the reassurance a diagnosis can bring. Bibliography 1.Dickson, Dennis W. Rademakers, Rosa Hutton, Michael L. Progressive supranuclear palsy: pathology and genetics Brain Pathology 2007; 12:74-82. 2.Friedman, Deborah I., Jankovic, Joseph, McCrary, John A. Neuro-ophthalmic Findings in Progressive Surpanuclear Palsy Journal of Clinical Neuroophthalmology 1992; 12(2): 104-109 3.Hamilton, Steven R. Neuro-ophthalmology of movement disorders Current Opinion in Ophthalmology 2000; 11: 403-407. 4.Kanski, Jack J. Clinical Ophthalmology 5th ed. Oxford, Buttersworth-Heinemann Ltd. 2003 5.Martin PR, Singlton CK, Hiller-Sturmhofel S. The role of thiamine deficiency in alchololic brain disease Alcohol Research & Health : The Journal of the National Institute on Alcohol Abuse and Alcoholism 2003; 27(2): 134-42. 6.Rehman, H.U. Progressive Supranuclear Palsy Postgraduate Medicine Journal 2000; 76:333-336. 7.Pelak, Victoria S. Hall, Deborah A. Neuro-ophthalmic manifestations of neurodegenerative disease.Ophthalmology Clinics of North America 2004; 17: 311-320. 8.Yoon CK, Chang MH, Lee DC. Wernicke-Korsakoff syndrome associated with hyperemesis gravidarum Korean Journal of Ophthalomology 2005; 19(3):239242.