Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
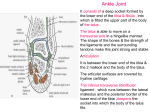
The Ankle Joint (Talocrural Articulation) By Prof. Dr. Muhammad Imran Qureshi Articulating Bones: Tibia (Lower end) Fibula (Lower end) Talus …. Body (Superior and Lateal aspects) Important Structural Landmarks: Tibia Medial Malleolus Fibula Lateral Malleolus Talus o Superior Pulley shaped articular surface o Medial Comma shaped articular surface o Lateral Triangular articular surface Type Of the Joint: Compound Synovial Variety Of the Joint: Hinge (Ginglymus) The movements are not quite those of a simple hinge, because the axis of movement is not fixed. It rather changes between the extremes of plantarflexion and dorsiflexion. Articular Surfaces: The articulating surfaces are covered with hyaline cartilage. The weight-bearing surfaces are the upper facet of the talus and the inferior facet of the tibia. The Stabilizing surfaces are those of the medial and lateral malleoli, which grip the sides of the talus. On the medial side, the distal articular surface of the tibia shows a saddle shaped facet for the talus. This articular surface extends to line the medial malleolus. On the lateral side, only the fibular malleolus articulates with the talus. Its medial articular surface is triangular to articulate with the lateral articular surface of the talus. The superior articular surface of the talus is pulley like thus called the trochlear surface. It is convex from before backwards but concave from side to side. It is also broad in front and narrow behind. The trochlear surface is continued down over each side of the body for articulation with the respective malleolus. On the medial side, it is comma shaped, the broad end of the comma being anterior. It articulates with the tibial malleolus. On the lateral side, almost the whole surface is articular, and is triangular. It is concave from above downwards and usually convex from before backwards. It articulates with the fibular malleolus. Synovial Capsule / Membrane: The synovial membrane is attached to the articular margin of the talus and clothes the intracapsular part of the neck. Elsewhere it is attached to all articular margins. Occasionally the joint cavity extends up a little between tibia and fibula, into the inferior tibiofibular ligament. Ligaments of the joint: Strong medial and lateral ligaments strengthen the joint. The ligament, on the medial side, is in two layers. The deeper part is narrow, extending from the tibial malleolus to the side of the talus, inserted there into the concavity below the comma shaped articular surface. Its shape is rectangular. The superficial part is triangular, like a delta and is therefore called the Deltoid ligament. It fans downwards from the borders of the tibial malleolus and its lower margin is attached to the medial tubercle of the talus (a weak band), to the edge of the sustentaculum tali and spring ligament (very strong band), and to the tuberosity of the navicular (a weak band). Thus the medial ligament not only strengthens the ankle joint, but also holds the calcaneus and the navicular against the talus. On the lateral side there are three separate bands, radiating from the lateral malleolus, which are collectively called the lateral ligament. The anterior and posterior bands pass to the talus, the intermediate band to the calcaneus. The anterior talofibular ligament joins the anterior border of the lateral malleolus to the neck of the talus. It is a flat band. The calcaneofibular ligament is a rounded cord extending from the front of the tip of the malleolus down and back to the lateral surface of the calcaneus. The strong posterior talofibular ligament lies horizontally between the malleolar fossa and the lateral tubercle of the talus. Above it lies the posterior tibiofibular ligament, whose lower part articulates with the talus. In plantarflexion these two ligaments lie edge to edge, but in dorsiflexion they diverge like the blades of an opening pair of scissors. Ligaments of the joint (Alternate Description) The three ligaments on the medial side are most conveniently described as originating from the medial malleolus and passing to insertions on tarsal bones; however, they are named as if they started on tarsal bones and converged on the tibia. The anterior talotibial ligament passes from the medial malleolus forward to the neck of the talus. The calcaneotibial ligament runs from the medial malleolus downward to the sustentaculum tali. The posterior talotibial ligament passes from the medial malleolus backward to the posteromedial corner of the talus. The gap between the anterior talotibial and calcaneotibial ligaments is filled in by fibers passing from the medial malleolus to the edge of the plantar calcaneonavicular ligament. Moreover, the breadth of the calcaneotibial and posterior talotibial ligaments is so considerable that the back edge of the former abuts the front edge of the latter. As a result, the three ligaments on the medial side of the ankle appear to form a single, fan-shaped complex radiating out from the' medial malleolus. The name given to this complex is the Deltoid ligament. Its middle fibers are primarily responsible for preventing abduction of the foot at the ankle; its anterior and posterior fibers resist fore and aft sliding. On the lateral side of the foot there are anterior talofibular, calcaneofibular, and posterior talofibular ligaments that originate from the lateral malleolus and correspond to their medial counterparts. These three ligaments are more obviously separate than their medial counterparts, and, thus, no lateral deltoid ligament exists. The calcaneofibular ligament resists adduction of the foot at the ankle; the anterior talofibular ligament resists forward sliding of the foot on the leg; the posterior talofibular ligament resists backward sliding of the foot. Blood Supply of the joint: The blood supply of the capsule and ligaments is derived from anterior and posterior tibial arteries and the peroneal artery. Nerve Supply of the joint: In accordance with Hilton's law, the joint is supplied from the deep peroneal and tibial nerves Movements of the joint: The upper and medial surfaces of the talus are in contact with the tibia and its medial malleolus in all positions of the joint. The lateral malleolus adapts itself to the lateral surface of the talus; this involves rotary and lateral movements of the lower end of the fibula, which cause reciprocal movements at the upper end of the bone, in the superior tibiofibular synovial joint. In full plantarflexion the smallest area of the talus is in contact with the tibia, but even in this position the amount of inversion and eversion possible at the ankle joint is very small indeed. Practically speaking, the ankle may be regarded as a true hinge joint. The axis of rotation is not horizontal, but slopes downwards and laterally. It passes through the lateral surface of the talus just below the apex of the articular triangle and through the medial surface at a higher level, just below the concavity of the comma-shaped articular area. It passes through the malleoli just above their apices. In fact , the axis changes during movement, because the upper convexity of the talus is not the arc of a circle, but rather of an ellipse. The obliquity of the axis involves a slight movement resembling inversion in full plantarflexion, and the reverse, resembling slight eversion, in full dorsiflexion, but these apparent movements are not of true inversion and eversion. Plantarflexion (up to 50°) is a powerful movement and is produced the gastrocnemius and soleus. This gives the basic thrust for propulsion. The long flexor tendons and the long and short peronei all have a secondary action of flexion on the ankle joint. Dorsiflexion (up to 25°) is produced by the tibialis anterior and peroneus tertius, aided on occasion by the toe extensors. Stability Of the joint: It depends upon THREE factors: Bony Factors Ligamentous Factors, and Muscular Factors The stability of the joint is ensured: By the powerful ligaments and tendons around it; By the insertion of the trochlea tali into the deep socket between the medial and lateral malleoli. The trochlea bears on the malleoli and on the distal surface of the tibia between them. The socket is not entirely rigid but has some spring because of the flexibility of the body of the fibula. If the talus is forced laterally, the lateral malleolus can move slightly outwards because, acting with the tibiofibular ligaments as a fulcrum, it springs the body of the fibula medially. In extreme cases this may lead to fracture of the fibula in the leg. The socket is deepened posteriorly by the inferior part of the posterior tibiofibular ligament (transverse tibiofibular ligament). Bony Factors: The top of the talus is "grasped" firmly by the socket formed by the distal tibia and fibula, preventing side to side and rotatory motion of the talus. Ligamentous Factors: Anteroposterior sliding and abduction / adduction are prevented by ligaments. There are three such ligaments on the medial side of the joint and a matching set on the lateral side. Muscular Factors: The tendons of the Flexor, Extensor and Peroneal muscles strengthen the joint from the sides.