Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
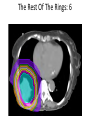
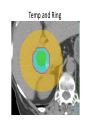
Clinical applications of SBRT: Lung, Liver, Pancreas MaryLou DeMarco, MS, CMD Susan Leuthold, CMD Over 1000 SBRT Lung Patients Planned at Moffitt Lung: Sim and Immobilization Gantry Collision Check Contours: PTV/GITV Contours: RINGS RING100 RING100 RING RING Boarding Pass: Constraints Case Study: Lung SBRT, Previous Tx Previous Tx Right On New PTV Make Contours Out Of Previous Tx Isodose Lines OARs Lungs: Minus GITV Challenge: Chestwall Dose PTV_edit PTV_edit Chestwall_R: 3cm up and down RING_100 RING 2 Arc Beams Prescription: 1000 x 5 = 5000cGy Optimizer: First Ring First Isodose Rings that we get The Rest Of The Rings: 6 Rings Into Optimizer With EUD @0.6 Rings to Max DVH & 0.09 Isodose Lines Pull In Make Ring of 50% Line The 50% line in Optimizer: EUD The 50% Line In Optimizer: Max DVH Gradient Index: RTOG 549.1 / 201.1 = 2.7 From RTOG: a 201.1cc PTV needs a Dose Gradient < 3.3, so the Dose Gradient is good OARs Previous Tx Areas Into Optimizer Isodose Lines Graded Plan Into Mosaiq SBRT of the Pancreas and Liver Susan Leuthold, CMD Dosimetry at MCC… Specializing Primary and secondary services GI and Sarcoma Esop, panc, gastric, adrenal, liver, gb, rectal, anal • Sim and treat (palliative) • 3D, IMRT, SRT, SBRT, HDR, LDR, Intra-op • My Team • • • • Advantages of SBRT • Shorter treatment course – Less scheduling conflicts – Less driving, lodging – More likely to complete tx • As effective (increase dose and local control) • Ease of planning • Overview of pancreas cancer • Definition of borderline resectable • Treatment technique – SBRT (3D gated) also use IMRT/VMAT • Then on to Liver (3D gated Vs. IMRT) The Pancreas What does the pancreas do? • Hormone production (endocrine) – Insulin – decrease glucose – Glucagon – increase glucose – Somatostatin – regulate insulin/glucagon production • Digestion (exocrine) – Break down protein, carbohydrates, and fat – Neutralize acid from stomach Pancreas Cancer • 9th most common cancer but 4th most common cause of cancer death in U.S. • ~50,000 new diagnoses per year • Most present at advanced stage • 15 – 20% resectable at diagnosis • R0 resection offers chance for cure Pancreas Cancer • Most present at advanced stage • Clinical presentation – Jaundice – Weight loss – Diabetes – Abdominal pain – Pruritus (itchy sensation) – Steatorrhea (excess fat in stool) Pancreas Cancer • Prognosis is grim – Long-term survival for all patients 3 – 4%, 5 yr – If have surgery 5 yr survival to 20% – “systemic disease” • Median survival – After resection: 12 – 26 months – Locally advanced: 9 – 13 months – Metastatic: 3 – 6 months Definitions • • • • Resectable Locally advanced – non-resectable Borderline resectable Resection classification Borderline Resectable Definition 1. ≤180° circumferential tumor abutment of portal vein (PV), superior mesenteric vein (SMV), or superior mesenteric artery (SMA) 2. Short segment (1.5 cm) encasement of PV or SMV amenable to partial resection and reconstruction 3. Gastroduodenal artery encasement to origin of hepatic artery Resectable SMV Locally advanced/unresectable Tumor SMA Borderline-resectable Tumor SMV Margin definitions • Negative margins – R0 • Microscopically positive margins – R1 • Grossly positive margins – R2 Goal of treatment • Complete surgical removal of the tumor • With no cancer at the edges of the specimen Our approach Chemo (GTX) over 9 weeks Gemcitabine (IV infusion) -Taxotere (IV infusion) -Xeloda (oral) • Then SBRT for 5 days • Re-eval for poss resection - Re-evaluation 3-4 weeks after • Restaging PET/CT • Tumor board presentation to see if lesion has shrunk away from blood vessel enough for surgeon to attempt resection SBRT planning • Tumor localization – Find tumor location accurately for each fraction. • Patient simulation – Modified simulation for SBRT • SBRT planning (3d gated or IMRT) – In this case, we create a set of beam angles and portals that deliver the treatment & the boost simultaneously – Dose painting – Gated if a lot of motion Prior to Simulation • Patient undergoes implantation of fiducial markers – Done via Endoscopic ultrasound (EUS) – Place 3-4 gold fiducials into the tumor itself – Fiducial markers will be useful for target delineation and for daily image guidance Fiducial markers Motion • Fluoro-sim before CT sim • Short term solution • Look at motion in orthog planes Motion analysis: how much does the pancreas move • Superior to inferior range – ~ 1 cm • Medial to lateral – ~ 1 cm • Ant – Post – ~ 1 cm At simulation • • • • • Full length custom cradle immobilization Arms up overhead Simulate on empty stomach Oral gastrograffin at least 30 mins prior to sim IV contrast with time delay to capture venous phase. Evaluate the motion 4D CT Evaluate the phases of maximum exhale Usually 40-60% If 50% is maximum exhale, this will be primary dataset • Fuse the 40 and 60 and the free breathing for target delineation. • • • • Gating box: measures respiratory excursion Motion during treatment SBRT planning Beam angle selection Blocking Jaw setting MLC settings Off kidneys Prescription • Multi-level prescription • Prescribe to lowest dose level • Prescribe to 85% isodose – Will adjust later • Typically 5 fractions • Start with 15 MV – Adjust lower if needed • Equally weight all beams – Will adjust later • Compute Preliminary dose Dose volume histogram Field-in-field MLC setting Intermediate dose PTV 30 DVH post calculation Segment weight optimizer • NOT IMRT! • SWO will not “rescue” OAR objectives • Min MU set to 10. Segment weight optimizer Final plan Final DVH Examples of Dose Painted Plans More examples Interesting examples Multiple prescriptions • The only chance a patient has for cure is if surgery is possible • A sub-class within the unresectable classification that is deemed borderlineresectable • By sufficiently shrinking the tumor with neo-adjuvant therapy these cases can become resectable • Using this technique… – Of the borderline-resectable patients more than half have been down-staged to resectable. • These patients are given the highest chance of long term survival. Example outside the pancreas Multiple PTV objectives simultaneously achieved LIVER SBRT (GATED) 3D Beam Angles Pre-conformed collimators MLC Blocking Conformed collimators Sup/inf opened ~1cm Sup/inf opened ~1cm MLC opened accordingly Prescription Equal weighting Dose objectives Dose Volume Histogram Final Beam Weights IMRT just for fun Temp and Ring Optimizer 3D versus IMRT SBRT Questions?