Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
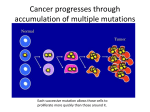
THE HIERARCHY OF SOMATIC MUTATIONS IN FOLLICULAR LYMPHOMA Michael R. Green, Andrew Gentles, Ramesh Nair, Jonathan Irish, Ron Levy, Ash Alizadeh. Follicular Lymphoma (FL) Follicular lymphoma histology FL flow cytometry black stain = T Cells (CD3) 3X B Cells (follicular structures) Lymphoma B cell receptor Ig light chain (k) T Cells (infiltrating tumor) Tumor-infiltrating T cells (CD3) 10X Lymphoma B cell receptor Ig light chain (k) BCL2 CD20 Follicular Lymphoma (FL) Clonally rearranged immunoglobulin Characterized by t(14;18)(q32;q21) translocation Incurable using conventional therapy ◦ Good candidate for molecularly-targeted therapies Frequent mutation of MLL2 histone methyltransferase Recurrent mutation of CREBBP histone acetyltransferase DLBCL FL MZL PTCL CLL/SLL MCL PMBL A. Adapted from WHO 2008 B. Solal-Celigny et al. Blood 2004;104:1258 Genetic “constants” Histone Modification by MLL2 and CREBBP CREBBP/EP300 MLL2/3 INACTIVATING MUTATION INACTIVATING MUTATION HAT MLL ING K27 K4 Targeted Therapy: Hitting the Achilles Heel of Cancer 7 July 2012 8 July 2012 9 July 2012 The Theory of “Personalized Oncology” MacConaill and Garraway J. Clin. Oncol. 2010;28:5219 Roychowdhury et al. Sci. Transl. Med. 2011;3:111 The Reality of “Personalized Oncology” Peter C. Nowell (1976) Science.194(4260):23-8. Mutation 1 Mutation 2 Mutation 3 Catalogue of Mutations Mutation 1 Mutation 2 Mutation 3 RELAPSE DRUG The Reality of “Personalized Oncology” Mutation 1 Mutation 2 Mutation 3 Catalogue of Mutations Mutation 1 Mutation 2 RELAPSE Mutation 3 DRUG Premise, Aim and Approach Premise: Early genetic events are likely to be clonally dominant and represent good targets for mutation-directed therapy Aim: To identify the hierarchy of genetic events in FL Approach: Identify clonally dominant mutations ◦ Consistently represented between intratumoral subpopulations ◦ Maintained from diagnosis to relapse Experimental approach FACS T-cells CD20int CD20hi DNA Extraction Whole Exome Sequencing Sanger Validation t(14;18) qPCR Tumor Purity Measurement IgHV cloning/sequencing Genetic “Constants” Exome Sequencing Methodology Constructed libraries from 3ug of DNA Captured exome with with Nimblegen SeqCap (v2) Indexed with Illumina barcodes 4-plexed samples on a single HiSeq 2000 lane (2x101bp) Mutation Calling Called somatic nucleotide variants (SNVs) with stringent implementation GATK: ◦ GATK score of ≥250 in B-cells ◦ GATK score of <50 in T-cells Filtered silent mutations and those in dbSNP/1000genomes Only considered cSNVs with: ◦ ≥20X coverage in both T-cells and B-cells ◦ <5% variant allele frequency (VAF) in T-cells ◦ ≥5% VAF in B-cells 96% validation rate Exome Sequencing and Mutation Detection In 10 tumors from 8 cases, identified 877 coding SNVs in 572 unique genes ◦ 95% of genes mutated in only 1/8 cases 100.0% 75.0% 50.0% 25.0% 0.0% Majority of Mutations in FL are Subclonal Assessing sub-population skew Interrogated minor allele frequencies of 232 germ-line coding SNPs/patient (1856 total) Some noise around VAFs of heterozygous SNPs ◦ By definition, variation in germline SNPs are false-positives* ◦ Set thresholds to obtain confident calls At 16% VAF deviation, 85 false-positives ◦ 4.58% error At 33% VAF deviation, 18 false-positives ◦ 0.97% error *Possibility of LOH over-estimating error Mutation Frequencies in Tumor Subpopulations More mutations, more clonal divergence Illustrative Case of Diagnosis/Relapse Comparison CASE 128 A 40 year old woman with enlarged lymph nodes and fevers found to have advanced follicular lymphoma Diagnosis (1996) ◦ Histology: FL grade 1 ◦ Stage: 4B ◦ Time to first treatment = 362 days ◦ First treatment = CVP (1997) achieved Complete Remission (CR) ◦ Second treatment = Id-vac (1998) Relapse (1999) ◦ Histology: FL grade 1 ◦ Treatment: Fludarabine + Cyclophosphamide, CR Second relapse in 2003, treated Patient alive as of Feb 2013 Interrogation of FL Relapses: Case 128 Genetic Evolution of Case 128 Conclusions The majority of mutations in FL are not recurrent and are subclonal. MLL2 and TNFRSF14 ◦ Skewed distribution in tumor cell subpopulations ◦ Lost between diagnosis and relapse in LP-J128 Subclonal = Late event CREBBP ◦ Equally represented in tumor cell subpopulations ◦ Maintained between diagnosis and relapse Clonally dominant = Early event Conclusions Acknowledgments Prof. Ron Levy Prof. Ash Alizadeh Prof. Jonathan Irish Dr. June Myklebust Dr. Itai Kela Shingo Kihira Dr. Chih Long Liu Prof. Sylvia Plevritis Dr. Andrew Gentles Dr. Ramesh Nair Prof. Hanlee Ji Dr. Eric Hopmans