Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
2
Drugs in the Body
LEARNING OBJECTIVES
• Identify the key components of the dose• Identify the main principles of organic
response curve that represent therapeutic
chemistry, pharmacodynamics, and pharmarange, efficacy, potency, and steady state.
cokinetics.
• Describe how those principles influence the
behavior of drugs in the body.
• Describe how atoms combine to form different kinds of molecules.
• Describe factors that influence absorption,
distribution, metabolism, and excretion of
drugs from the body.
• Distinguish how pH affects behavior of acidic
and basic drug molecules.
Interactive self-quizzes,
games, audio files, and
glossaries help you to learn
drug names and facts.
T
he ways that drugs behave in the body depend on the principles of organic
chemistry. Organic chemistry is the study of the structure, properties, and reactions of carbon-based compounds. Learning basic concepts and principles of
organic chemistry will add great depth to your understanding of how drugs behave in
the body and how they are chosen for individual patients. This chapter introduces the
general concepts that govern the chemical makeup of drugs and discusses principles
that affect how they get into, move around in, and exit from the body. Last, this chapter
covers differences in patient populations that change the chemical characteristics and
behavior of drug therapy. Pharmacy technicians with an understanding of these
concepts and how they apply to specific patients will better grasp how drug dosing and
therapy decisions are made in the practice setting.
Atoms and Molecules
All matter can be broken down to its most basic unit, the atom. All matter—including
the human body—is made up of atoms. Ninety-two different types of atoms, or
elements, exist naturally on Earth. Chemists have chosen to organize and display the
elements in a particular arrangement (see Figure 2.1).
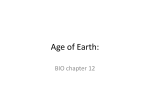
The periodic table of the elements arranges the naturally occurring elements, along
with those synthesized in the laboratory setting, into rows and columns that group
atoms by their chemical properties. Elements in the same column have similar properties
and reactivity, affecting the way they combine with other molecules. Elements in each
row increase in size and mass (from left to right), which also helps predict behavior.
Atomic Structure
20
020-032_PharmEss_02.indd 20
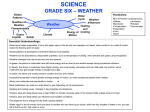
Atoms are made up of a nuclear center and an outer shell. The nucleus is a small core
of solid matter, including protons and neutrons, and the outer shell is an orbital space
where electrons circulate. Each element has a unique number of electrons and protons
(see Figure 2.2).
Protons have a positive electrical charge and determine an element’s atomic
number, as shown in the periodic table of the elements. Protons have measurable mass
and are found in the nucleus. Neutrons are also in the nucleus and are neutral, neither
positively nor negatively charged. However, they have mass and add to an atom’s
atomic weight. Electrons have a negative charge and seek to balance the electrical
6/29/10 8:47:16 AM
Chapter 2 Drugs in the Body
|
21
Figure 2.1
Periodic Table of the Elements
Elements in the same group tend to behave in similar ways when combining with other elements.
1
2
3
4
5
6
7
1
H
1.008
3
Periodic Table of the Elements
IA
Li
6.939
11
Na
22.99
19
K
39.102
37
Rb
85.47
55
Cs
4
II A
5
Be
Fr
215
B
6
IV A
C
7
VA
N
8
VI A
O
VII A
9
F
He
4.003
10
Ne
10.811 12.011 14.007 15.999 18.998 20.183
12
13
Mg
24.312
20
Ca
40.08
38
Sr
87.62
56
Ba
88
III B
21
Sc
44.956
39
Y
88.905
57
•La
IV B
22
Ti
47.9
VB
23
V
VI B
24
Cr
Ra
89
41
Zr
91.22
72
Hf
Nb
92.906
73
Ta
104
Rf
Actinide
series
58
Ce
105
(261)
59
Pr
Db
(262)
60
Nd
140.12 140.91 144.24
90
Th
91
232.04
Figure 2.2
Atomic Structure
Electromagnetic forces keep
an atom together but do not
allow electrons and protons
to touch.
Professional Focus
Nuclear pharmacy is a
specialty practice in which
radioactive isotope material
(usually called dye) is
prepared for imaging
procedures. Technicians
and pharmacists working
in this field must receive
specialized training
to handle radioactive
materials.
Pa
231
VII B
25
Mn
26
Fe
VIII
27
Co
50.942 51.996 54.938 55.847 58.933
40
226.03 227.03
• Lanthanide
series
020-032_PharmEss_02.indd 21
III A
0
9.0122
42
Mo
95.94
74
W
132.91 137.34 138.91 178.49 180.95 183.85
87
2
92
U
106
Sg
(266)
61
Pm
145
93
Np
43
Tc
(97)
75
Re
186.2
107
Bh
44
Ru
Sm
Rh
101.07 102.91
76
Os
190.2
108
Hs
(264)
62
45
(269)
63
Eu
77
Ir
192.2
109
Mt
(268)
64
Gd
28
Ni
58.71
46
Pd
106.4
78
Pt
Pu
95
96
Am Cm
29
Cu
63.546
47
Ag
107.87
79
Au
II B
30
Zn
65.37
48
Cd
112.4
80
Hg
14
Si
15
P
110
Ds
(271)
65
Tb
97
Bk
16
S
17
Cl
18
Ar
26.982 28.086 30.974 32.064 35.453 39.948
31
Ga
69.72
49
In
32
Ge
72.59
50
Sn
33
As
74.922
51
Sb
114.82 118.69 121.75
81
Tl
82
Pb
83
Bi
195.09 196.97 200.59 204.37 207.19 208.98
150.35 151.96 157.25 158.92
94
IB
Al
111
34
Se
78.96
52
Te
127.6
84
Po
210
35
Br
79.904
53
I
126.9
85
At
210
36
Kr
83.8
54
Xe
131.3
86
Rn
222
Rg
(272)
66
Dy
162.5
98
Cf
67
Ho
68
Er
69
Tm
70
Yb
71
Lu
164.93 167.26 168.93 173.04 174.97
99
Es
238.03 237.05 239.05 241.06 244.06 249.08 252.08 252.08
100
Fm
257.1
101
Md
258.1
102
No
259.1
103
Lr
262.11
proton
charge of an atom; thus the number of electrons
normally equals the number of protons. Electrons
weigh so little that they do not contribute significantly to the mass of an atom. The interplay of
electrons and their effect on electrical charge determine the chemical activity of an element and its
ability to combine with other atoms.
Ions are atoms or molecules with an electrical
charge. When electrons are separated from an
atom, energy is released and a positively charged
ion is formed. When an extra electron is added to
electron
an atom’s orbital, a negatively charged ion is
nucleus
formed. When neutrons are added to an atom, the
charge does not change, but the atom becomes heavier. This type of atom is called an
isotope and is often radioactive. Isotopes are used in nuclear medicine to perform imaging on the body, such as in cardiac catheterization.
neutron
Chemical Bonds
Atoms combine by exchanging electrons in their outer shells. This exchange occurs in
two ways. Atoms can share electrons, or they can transfer them completely to another
atom. Sharing electrons is called a covalent bond, a strong bond that creates a neutrally
charged molecule (see Figure 2.3).
Ionic bonds occur when one element has entirely lost and another has gained
electrons, but the two atoms remain connected by electromagnetic attraction (see
Figure 2.4). One atom becomes positively charged, and the other is negative. Each
6/29/10 8:47:19 AM
| Unit 1 Introduction
22
Figure 2.3
Covalent Bond
In a covalent bond, electrons share orbitals around the nucleus.
H (#1)
H (#1)
1P
0N
1P
0N
1P
0N
1P
0N
Molecules and Functional Groups
Figure 2.4
Ionic Bond
Sodium (+) and chloride (–) combine via ionic bonds to
make table salt.
Na (#11)
Cl (#17)
11 P
11 N
17 P
17 N
11 P
11 N
17 P
17 N
• •1
• •1
Figure 2.5
Ampicillin Molecule
The amino functional group in ampicillin is shown as NH2,
and the carboxyl functional group is shown as COOH.
O
CH
C
NH2
S
NH
O
ampicillin
020-032_PharmEss_02.indd 22
atom is individually referred to as an ion, because it has a
charge. Ionic bonds are considered to be polar. They are
weaker and more easily broken than covalent bonds.
In the body, most substances are made up of molecules
using covalent bonds. In fact, all organic material contains
carbon, an element that combines with other atoms or
elements primarily by covalent bonds. Some molecules,
such as minerals and electrolytes, exist in the body as ions.
Examples of ions in the body are sodium (Na+), potassium
(K+), and chloride (Cl–).
N
CH
CH
COOH
When two or more atoms combine via covalent or ionic
bonds, a molecule is formed. Some molecules form the
structure of the body itself, and others, called biochemicals,
react with each other to conduct various physiological
processes.
Organic molecules have a carbon backbone that occurs
in chains of atoms strung together or in ring-like structures.
Forming rings is a unique property of carbon that allows it
to behave in ways conducive to organic life. On each backbone you find functional groups, which are the side
portions of a molecule that give it the chemical properties
that allow it to react with others in specific ways. Each
functional group has a specific shape and particular
tendency to react according to its chemical properties.
Molecules react only with those receptors in the body that
are shaped similarly, much like a lock and key. A drug’s
activity can be predicted by examining its molecular shape
and functional groups (see Figure 2.5).
Isomers are compounds (i.e., molecules with differing
types of atoms) with the exact same chemical makeup (the
same number and types of atoms), but they are not
arranged the same way within space. Many times, isomers
of the same molecule are mirror images of each other
(called stereoisomers). A drug product may contain a
mixture of stereoisomers, one having more drug activity,
and the other causing more side effects.
The most common molecules in the body are carbohydrates, peptides, lipids, and nucleic acids. Carbohydrates are
an essential part of nutrition. Breaking bonds in carbohydrate
molecules, such as glucose and fructose, produces energy
that the body can use to sustain life. Large carbohydrate
molecules, such as starches, are used in building cell
membranes or stored for energy. Peptides are composed of
amino acids and are the building blocks of protein molecules.
Proteins are most often used to build tissue but can also be
used for energy. Lipids are molecules that form long chains
of covalently bonded carbon and hydrogen atoms. Lipids are
soluble in fat or oil and are used to create hormones and
other active biochemicals. Nucleic acids are part of deoxyribonucleic acid (DNA), which forms the genetic material
contained in the nucleus of each cell. DNA serves as the road
map for the body’s processes and growth cycle.
6/29/10 8:47:20 AM
Chapter 2 Drugs in the Body
|
23
No matter what learning styles you prefer, using hands-on manipulation reinforces concepts involving
spatial relationships of molecules. Whether you work in a group, as Creators prefer, or alone, as Producers
prefer, you might find building molecules using a toy building-set (such as Tinkertoys®) useful to
understanding how bonds are formed and why functional groups affect molecular behavior. Using such a
toy, try building two molecules that are stereoisomers (mirror images) of each other.
Acids and Bases
acidic
Understanding acidic and basic properties of molecules is useful because most drugs are
either weak acids or weak bases. These properties affect how drug molecules enter and
behave in the body. The pH scale is a way to measure acidic and basic properties of
substances. Substances with a low pH (below 7) are acids, and those with a high pH
(over 7) are bases (see Figure 2.6).
The pH scale measures the propensity of a molecule to shed or
Figure 2.6
take on hydrogen ions. Hydrogen ions are created when an electron
pH Scale for Acids and Bases
orbiting a hydrogen atom is lost, leaving a lone proton with a positive
Gastric acid in the stomach has a pH around 2 to 3.
charge (H+). In a sense, acidic molecules donate protons to other
molecules. Basic molecules easily accept protons. Those molecules
[H3O] pH
that have the ability to donate multiple hydrogen ions are considered
strong acids, and those that donate few are weak acids. The opposite
concentrated HCl
101 1
is true for bases.
battery acid
100
0
When acids and bases come together and an exchange of protons
occurs,
the remaining molecules become ionized (positively or nega1
10
1
tively charged). Ionization affects drug activity, because ionic molelemon juice
101 2
cules cannot easily cross membranes and enter the bloodstream. For
vinegar
example, putting a basic drug with a high pH into the acidic stomach
soft
drink
103 3
beer
facilitates the exchange of many protons, creating ionic molecules
tomato
104 4
that are difficult to absorb into the bloodstream. Conversely, if an
coffee
acidic drug enters the acidic environment of the stomach, more of it
urine
105 5
rainwater
will get absorbed because few molecules will shed protons and most
milk
106 6
will remain neutrally charged.
7
108
8
saliva
pure water
blood
seawater
109
9
baking soda
basic
neutral 107
1010 10
1011 11
ammonia
1012 12
hair remover
1013 13
oven cleaner
1014
020-032_PharmEss_02.indd 23
soap
14
Pharmacodynamics
Generally, drugs work by mimicking, enhancing, or blocking the
activity of substances that are usually already present in the body. In
most cases, drug molecules interact with receptors on the surface or
inside of specific cells. This interactive process is explained by drug
receptor theory, which is based on a lock and key mechanism (see
Figure 2.7). Cells of the body have many different receptor molecules
(or locks) on their surface and various substances (or keys) fit exactly
into them. Usually, these “key” substances are produced or processed
within the body. That is, they are endogenous chemicals that act as
messengers for communication and for regulating physiological
processes. When a messenger molecule connects with a receptor, it
triggers a series of reactions within the cell.
Pharmacodynamics is the study of drug receptor theory at this
molecular level and how that interaction translates to drug activity on
the entire body. Through pharmacodynamics, you can determine a
drug’s mechanism of action and, therefore, its effect on the body.
Drug molecules mimic the molecular shape of the body’s endogenous
6/29/10 8:47:21 AM
24
| Unit 1 Introduction
Figure 2.7
Drugs and Receptors
Drug molecules are similar to but not exactly the same as
endogenous molecules. Their slight differences can be the reason
why side effects occur.
key drug or endogenous
substance
lock receptor
correct fit,
drug activity
incorrect substrate
no drug activity
chemicals and then either produce similar effects or block the activity. Logically, you
can see why drugs with similar molecular shape are categorized together, because they
interact with the same receptors and thus have similar activity.
Drugs whose activity is to stimulate a specific response when binding to receptors
are agonists, and those drugs that block a response when binding to receptors are
antagonists. Antagonists block a response in one of two ways. They can either directly
inactivate the receptor, blocking its ability to trigger a response. Or they can bind to
the receptor in a competitive fashion, keeping other agonist molecules from binding
and then triggering a response. When a drug binds with high affinity to a receptor, it
sticks to the receptor longer—perhaps even permanently. Those drugs with low affinity
for a receptor may bind quickly and then fall off easily, which can lead to a short duration of action.
Dose-Response Relationship
For a drug to be effective, it must reach its site of action in a large enough concentration
to produce a measurable effect. In other words, enough of the drug molecules must
reach the site of action to elicit a significant response. A drug’s safety for use depends
on its ability to reach desired concentrations without producing too many toxic effects.
Therefore, proper dosing hinges on achieving the desired effect without producing
unwanted effects.
This relationship between dose and effect is depicted graphically as a dose-response
curve (see Figure 2.8). This graph displays concentration of drug in the bloodstream over
time. The curve shows that increases in dose result in increased response. Eventually, a
ceiling effect is reached in which no further increase in dose produces additional response.
Proper drug dosing aims for blood concentrations in the middle of this curve, the
therapeutic range (see Figure 2.9). The lower threshold of this range is the minimum
therapeutic concentration. Drug dosing must achieve at least this concentration to gain
any measurable effect. The upper edge of this range is the toxic concentration; above
this concentration the incidence of toxic effects may outweigh any benefit of the drug
and thus pose too great a risk.
020-032_PharmEss_02.indd 24
6/29/10 8:47:21 AM
Figure 2.8
Dose-Response Curve
The ceiling effect is usually dangerously high and associated
with many toxic effects and even death.
drug concentration in blood (i.e., “response”)
Chapter 2 Drugs in the Body
maximum therapeutic
drug level
|
25
ceiling effect
maximum therapeutic dose
dose
020-032_PharmEss_02.indd 25
minimum drug level
for therapeutic effect
onset of
drug action
0
Professional Focus
In hospitals, pharmacists
often assist prescribers in
dosing medications with
narrow therapeutic ranges
or drugs that have severe
side effects associated
with elevated peaks and
troughs. When helping
gather laboratory results
for drug dosing, you should
be sure to record the time
doses are given in relation
to when blood draws are
performed. Blood draws
taken at the wrong time
can render lab results
useless for drug dosing.
toxic concentration
therapeutic
range
concentration
Figure 2.9
Time-Response Curve
Some drugs have a narrow therapeutic
range whose minimum therapeutic
and toxic levels are close to each other.
In these cases, drug dosing must
be monitored closely to ensure the
appropriate amount of drug is given
to produce desired effects without
overshooting and causing toxic effects.
1
2
3
termination
of drug action
4
5
6
time (hours)
7
8
9
10
The dose-response curve can be used to determine drug efficacy and potency. When
a dose-response curve is lower in vertical height for one drug compared with another, the
first drug is considered less effective. When the curve is shifted horizontally left or right
as compared with another drug, the potency differs. For instance, a drug that achieves the
same response as another drug but at a lower dose (left shift) is more potent.
For drugs with which a constant concentration in the therapeutic range is desired,
timing of doses is important. Figure 2.10 shows how repeated doses are timed to
produce an average drug concentration that remains in the therapeutic range. When
this constant concentration is maintained, steady state is achieved. Up to five doses, if
timed appropriately, may be required before blood concentrations reach steady state.
When time is of the essence, a loading dose is given. A loading dose is a dose that is
large enough to bring blood concentrations up to the therapeutic range immediately.
Subsequent doses keep levels at the steady state.
The point at which a drug is at the lowest concentration between doses is called the
trough. The peak is when the concentration is at its highest. For some drugs, peaks and
troughs are measured to be sure they are high and low enough. Drug levels aid prescribers in making certain that patients get maximum benefit but avoid toxicity. Pharmacy
technicians are sometimes asked to assist pharmacists in retrieving drug concentration
levels from laboratory data. Once steady state has been reached and the prescriber is
sure that peaks and troughs are appropriate, monitoring may become less frequent.
7/8/10 10:23:53 AM
| Unit 1 Introduction
Figure 2.10
Steady State
Another way to maintain a steady
concentration in the therapeutic range
is to give a continuous infusion.
120
average steady state
concentration
110
concentration (% of Css average)
26
100
90
80
70
60
50
40
30
20
10
0
0
1
2
3
4
5
time (elimination half-lives)
6
7
8
Pharmacokinetics
The study of pharmacokinetics uses mathematical modeling to observe and predict
Art for Pharmacology
how a drug enters, moves around, and leaves
body. In other words, pharmacokinetEssentialthe
for Technicians
EMC
ics studies how drugs are absorbed, distributed,
and eliminated from the bloodstream
(see Figure 2.11). This entire process canFig
be02_10A
described in terms of four phases: absorpRolin Graphics
tion, distribution, metabolism, and excretion.
lm 01/19/10 29p4 x 17p9
Figure 2.11
Pharmacokinetic Process
Most oral drugs enter the bloodstream through the lining
of the intestines, where all blood flow goes through the
liver before entering the rest of the body.
1
absorption of drug
into bloodstream
3
metabolism
(biotransformation)
of drug by liver
2
distribution
of drug to
organs and
tissues
4
excretion of drug in
liquid waste by kidney, and
solid waste by intestine
020-032_PharmEss_02.indd 26
6/29/10 8:47:24 AM
Chapter 2 Drugs in the Body | 27
Absorption
Absorption is the process by which drugs enter the bloodstream. It is measured as the
rate and extent to which a drug moves from the site of administration to the circulating
blood. On the time-response curve (see Figure 2.9), absorption is the upward-sloping
part of the curve. Absorption affects the onset of drug action as well as the extent of
action. For instance, if a drug is quickly and easily absorbed, the onset of action is fast
and the effect is noticeable and great. If the absorption is slow and incomplete, only a
small amount of drug reaches the bloodstream and gets to the intended site of action.
The route of administration affects absorption by enhancing or limiting systemic
effect. For example, oral administration is used frequently because it usually results in
good systemic absorption through the small intestines. Intravenous administration
skips the absorption step entirely by administering drugs directly into the bloodstream.
Topical routes do not always produce a measurable systemic effect because absorption
is usually limited.
Dosage form affects absorption by taking advantage of solubility properties to regulate the release of drug molecules. Before a drug can enter circulation, it must dissolve.
Therefore, solid dosage forms usually result in slower absorption rates than do liquids.
Transdermal patches release drug slowly, so that absorption through the skin is steady
and incremental. Some tablets and capsules are specially manufactured or coated for
specific solubility properties. Orally disintegrating tablets (ODTs), also referred to as
rapidly-dissolving tablets, are quickly absorbed when placed on the tongue because
they instantly dissolve in saliva. Coated tablets take longer to dissolve and absorb.
Acidic and basic properties of drugs and their environment affect drug solubility and
ultimately drug absorption. When a basic drug is in an acidic environment, it dissociates into ionic particles, which cannot cross membranes easily. Acidic drugs placed in
an acidic environment do not easily dissociate, and thus more drug will be absorbed.
The transport mechanisms that drugs use to cross membranes also affect absorption.
Molecules cross membranes by active and passive transport mechanisms (see Figure
2.12). Crossing membranes between the site of administration and the circulatory
system is necessary for drug activity. Active transport mechanisms use energy to bring
drug molecules across a membrane, whereas in passive transport mechanisms molecules move across on their own. An example of an active transport mechanism is the
sodium/potassium exchange pump, which requires ATP for energy (Na-K-ATPase, aka,
sodium pump). These proteins, which traverse the cell membrane, use energy to pump
potassium into, and sodium out of, cells. Because active transport mechanisms are
limited by the availability of energy sources, they can become saturated, or maxed out,
which limits overall absorption.
Figure 2.12
Transport Mechanisms
In simple diffusion, molecules move either directly through the membrane itself or through an open channel.
active transport
passive transport
simple diffusion
facilitated diffusion
ions
drug molecules
membrane
{
simple diffusion
through membrane
020-032_PharmEss_02.indd 27
simple diffusion
through gated channel
carrier molecule
carrier molecule
energy
concentration gradient
6/29/10 8:47:25 AM
28
| Unit 1 Introduction
Passive mechanisms, on the other hand, are usually driven by concentration gradients. Drugs absorbed via passive transport move from an area of high concentration
(the site of administration) to an area of low concentration (the bloodstream). Thus,
higher doses typically produce greater absorption. Diffusion is a passive transport mechanism by which many drugs are absorbed because molecules simply move along a
concentration gradient.
Last, blood flow and surface area affect absorption. For instance, the gastrointestinal
tract may not have a conducive pH for a drug to be absorbed. But the great amount of
surface area and good blood flow to the small intestine overcome this limitation to
absorption. Surface areas that are large, thin, and have good blood supply, like those of
the small intestine and lungs, can easily affect systemic absorption.
Distribution
Distribution is the process by which drugs move around in the bloodstream and reach
other tissues of the body. Consequently, distribution is highly affected by blood flow. If
blood flow is poor in a particular tissue or area of the body, few drug molecules are
able to reach it. On the other hand, organs with high blood flow (for example, the
heart, kidneys, liver, and lungs) are exposed to drugs easily.
A measurement known as volume of distribution (Vd) indicates how a drug is
distributed within the compartments of the body. For example, a highly water-soluble
drug stays in the bloodstream—the primary compartment for water-soluble drug distribution. However, if a drug is highly fat- or lipid-soluble, it can accumulate in fatty
tissue and then slowly be released back into the bloodstream over time. This second
example is referred to as a two-compartment model. Drugs are usually distributed to
one- or two-compartment models. Drugs that have more than one compartment for
distribution must be dosed accordingly in order to avoid accumulation over time and
increased potential for toxicity.
Two other factors greatly affect distribution: protein binding and the blood-brain
barrier. Some drug molecules have a high affinity for protein molecules and thus
bind to proteins, such as albumin, that circulate in the blood. When drug molecules
are bound to proteins in the blood, they are not free to reach the intended site of
action. If a drug binds to a large extent (90% or better), distribution is affected. If
two highly protein-bound drugs are given together, they compete with each other for
binding sites, leaving more of both drugs to roam freely in the blood. Therefore, they
are more easily distributed. If dosing is not adjusted accordingly, both drugs can
cause toxic effects.
The blood-brain barrier (BBB) is a physical layer of cells that affects distribution of
drugs to the central nervous system. Although oxygen and carbon dioxide molecules
easily pass across the BBB to reach brain cells, most larger drug molecules do not. This
barrier is structured to allow only select molecules through. It serves as a good defense
mechanism for preventing harmful substances from reaching delicate brain tissue, but
may also limit access for desired drug therapy.
Elimination
Elimination is the process by which drugs leave the body. Elimination can be measured
as the rate and extent to which a drug leaves the bloodstream. On the time-response
curve (see Figure 2.9), elimination is the downward sloping part of the curve. Half-life
(t1/2) refers to the time it takes for half (50%) of a drug to be cleared from the blood. It
takes approximately eight half-lives for a drug to be completely eliminated from the
body. Two processes, metabolism and excretion, affect elimination half-life. Drugs can
be deactivated via metabolism first and then excreted from the body, or they may be
excreted unchanged.
020-032_PharmEss_02.indd 28
6/29/10 8:47:25 AM
Chapter 2 Drugs in the Body | 29
Metabolism The liver contains enzymes that metabolize drugs and other substances
in the body. Its purpose is to detoxify the blood. The liver is considered the primary site
of drug metabolism. Drug metabolism is, therefore, highly dependent on blood flow to
the liver as well as the efficiency and function of enzymes located there. In some cases,
drugs rely on metabolism to activate them. These are called prodrugs.
First-Pass Effect Because blood coming from most of the gastrointestinal system
goes through the liver before entering the rest of the body’s circulation, many drugs
undergo the first-pass effect. This effect refers to the liver metabolizing drugs as they
“pass,” or travel through it. As a result, the full drug dose does not reach the body, and
its systemic effect is lessened or effectively eliminated. For those drugs that are quickly
and easily metabolized by liver enzymes, this first-pass effect is especially problematic,
and alternative routes of administration that bypass the liver must be used.
Drug Interactions Many liver enzymes are involved in metabolism; the cytochrome
P450 enzyme system most frequently deactivates drugs. Cytochrome P450 enzymes
that metabolize drugs are numbered. Common ones include 1A2, 2A6, 2C9, 2D6, and
3A4. Drugs that interfere with these enzymes can affect other drugs that need these
enzymes for proper elimination. Two drugs that use the same enzyme system, when
given together, can compete for elimination and increase potential for toxicity. It’s easy
to see how the cytochrome P450 system is a common source of drug interactions.
Excretion The process by which drug molecules are removed from the bloodstream,
excretion primarily occurs in the kidneys, the organs responsible for filtering substances
from the blood and making urine. Excretion can also occur via bile, feces, sweat, and
exhalation. Usually, excretion is highly dependent on blood flow through the kidney as
well as kidney function itself. Like transport mechanisms that control entry into the
bloodstream, excretion can occur by active or passive mechanisms. Ionization also
affects excretion, because highly ionized drugs cannot easily cross membranes to exit the
bloodstream. The pH of urine can therefore affect ionization and elimination rates.
Special Populations
The specific characteristics of individual patients affect the pharmacokinetic properties
of the drugs they take. Although some population generalizations can be made, no two
patients are exactly alike. Awareness of these differences is important when choosing
the best drug for each patient, as well as for dosing and delivering it in a way that will
be both safe and effective.
Differences in age and function of the liver and kidneys create the most problems,
but other factors also influence pharmacokinetic parameters. In regard to gender,
females have higher body fat content (compared to males), which affects drug distribution. Metabolism rates are often higher in men than in women, again affecting drug
elimination. In pregnancy, gastrointestinal motility slows, allowing more time for
absorption. Blood volume also increases, effectively lowering the concentration of blood
proteins and distribution. Urination also increases, affecting elimination. In severe
cardiovascular disease, blood flow decreases, altering blood supply to vital organs such
as the liver and kidneys. In hyperthyroidism, the metabolism rate increases in the liver,
enhancing elimination.
Age Very young and very old patients pose the greatest risks to safe drug therapy
because the pharmacokinetic behavior of drugs varies widely in these populations. In
pediatric practice (infants and children), infants are of greatest concern, because their
body makeup and liver function are different from those in adults. Babies have higher
body water content, so drugs that are highly water-soluble will distribute well, making
020-032_PharmEss_02.indd 29
6/29/10 8:47:25 AM
30
| Unit 1 Introduction
toxicity an issue. Blood circulation is also very good in pediatric patients. However, liver
function is not fully mature at birth. It takes months to years for all liver enzyme systems
to become fully functional. Therefore, absorption, distribution, and metabolism are all
affected in infants and children.
In geriatric practice (elderly patients), you must consider several different effects
on pharmacokinetic parameters. First, acidity in the stomach is usually decreased in
older adults, which translates to a higher pH. Drugs that need a highly acidic (low pH)
environment for absorption are affected. Older patients tend to have higher body fat
content, so drugs that are highly fat-soluble may distribute well and accumulate. As
people age, both kidney and liver function decrease, so elimination drops dramatically.
Blood flow to these vital organs also decreases with age. Doses are usually decreased
and dosing intervals increased to accommodate altered absorption, distribution, and
elimination in older patients.
Liver Disease Because metabolism occurs primarily in the liver, problems in liver
function can greatly affect drugs eliminated via metabolism. Cirrhosis, hepatitis, and
other liver diseases can severely affect liver function. In these cases, doses must usually
be adjusted downward.
Kidney Disease Because excretion happens most often through the kidneys, problems with kidney function greatly affect drug elimination. Both acute and chronic
kidney failure make a difference in a drug’s ability to leave the body. If doses are not
adjusted accordingly, drugs accumulate and cause toxicity.
Chapter Summary
Grasping concepts related to pharmacokinetics can be difficult. Producers and Directors may find it useful
to redraw the dose-response curve to represent the influence of various factors on absorption and
elimination. Enactors and Creators may find group discussion valuable for reasoning out the effects that
changes in absorption, distribution, and elimination have on the dose-response curve and drug behavior.
The atom is the smallest unit of matter. Atoms
are made up of positively charged protons,
uncharged neutrons, and negatively charged
electrons. The periodic table of the elements
categorizes elements, or types of atoms, into
groups with similar chemical properties. When
atoms bond together, they combine via covalent
or ionic bonds to form molecules. Common
molecules found in the body are carbohydrates,
lipids, proteins, and nucleic acids. Each of these
molecules contains various functional groups
that give them particular qualities that predict
how they behave in the body. The same may be
said about drug molecules. Their functional
groups and behavior in acidic and basic environments determine how drugs are absorbed,
distributed, and eliminated from the body.
Pharmacodynamics studies how drugs act on
the body at the molecular level. Drug receptor
020-032_PharmEss_02.indd 30
theory helps explain drug activity. Receptor
agonists stimulate a response, whereas antagonists block a response.
Pharmacokinetics is the study of how drugs
move around in the body. The four phases of
pharmacokinetics are absorption, distribution,
metabolism, and excretion. Mathematical
models describe these phases, and graphical
representation describes how drugs enter and
exit the bloodstream. Drug dosing depends on
these concepts.
Various factors affect individual patient
pharmacokinetic parameters for drug therapy.
Factors such as age, gender, liver/kidney function, and certain disease states affect how drugs
are absorbed, distributed, and eliminated. Such
characteristics are taken into account when
choosing appropriate drug therapy and dosing.
6/29/10 8:47:26 AM
Chapter 2 Drugs in the Body | Chapter Review
✔
For the following sets of exercises, write the exercise heading, exercise numbers, and your answers on a
separate sheet of paper. Your instructor may direct you to turn in the sheet of paper or discuss your
answers as a class.
REVIEW THE BASICS
Choose a, b, c, or d as the correct answer to each multiple-choice question.
1. Which of the following is the part of an
atom that is negatively charged and orbits
around the nucleus?
a. proton
b.neutron
c. electron
d.isotope
6. In which of the following routes of administration would you most likely encounter
problems with the first-pass effect?
a. oral
b.intravenous
c. transdermal
d.inhalation
2. Which of the following is a chemical bond
between atoms wherein electrons are shared?
a. covalent
b.ionic
c. polar
d.stereoisomer
7. If someone had alcoholic liver cirrhosis,
which pharmacokinetic phase would most
likely be affected?
a. absorption
b.distribution
c. metabolism
d.excretion
3. Which of the following is true of acidic
substances?
a. Acids easily accept hydrogen ions (H+).
b.Acids easily donate hydrogen ions (H+).
c. Acids exist in their ionic form when put
in an acidic environment.
d.Acids exist in their nonionic form when
put in a basic environment.
4. Which of the following is the membrane
transport process that moves drug molecules
from the site of administration into the bloodstream according to a concentration gradient
(high to low)?
a. diffusion
b.active transport
c. sodium/potassium ion pump
d.none of the above
5. Which of the following factors could affect
the absorption of an oral drug?
a. poor blood flow to gastrointestinal tract
b.changing the pH of the stomach (such as
taking an antacid)
c. dissolving the drug in water before
swallowing
d.all of the above
020-032_PharmEss_02.indd 31
31
8. Which of the following is the term for the
time it takes for the concentration of drug in
the blood to drop to half?
a. onset of action
b.duration of action
c. half-life
d.volume of distribution
9. The hepatic cytochrome P450 enzyme
system affects drugs in which phase of
pharmacokinetics?
a. absorption
b.distribution
c. metabolism
d.excretion
10. Which of the following phases is represented in the upward-sloping portion of the
dose-response curve?
a. absorption
b.distribution
c. metabolism
d.excretion
6/29/10 8:47:26 AM
32
| Unit 1 Introduction
✔
KNOW THE DRUGS
Match each major types of body molecule with its corresponding description.
Body Molecule
Body Molecule Description
1. Carbohydrates
a. Molecules that form the building blocks of protein and tissue
2. Peptides
b. Molecules that form hormones and biochemicals
3. Lipids
c. Molecules that form sugars and are used for energy
4. Nucleic Acids
d. Molecules that form genetic material (DNA) inside cells
✔
PUT IT TOGETHER
For each item, write down a single term to complete the sentence, the correct letter in response to the
multiple-choice question, true or false, or a short answer.
1. Protein binding within the bloodstream
primarily affects ____________ of a drug.
2. Water molecules move across membranes
by diffusion like drug molecules do. If a cell
were placed in a solution of pure water,
which of the following would happen?
Explain why you chose your answer.
a. Water would enter the cell, which may
burst.
b. Water would leave the cell, which may
shrivel.
c. Nothing, the concentration gradient is
equal.
3. True or False: A leftward shift in the doseresponse curve for one drug compared with
another means the drug is less effective.
4. For the following organs of the body, describe
how the phases of pharmacokinetics are
different in an infant as compared with a
normal adult.
Body fat
Liver
Kidney
5. Describe the difference between an agonist
and an antagonist drug.
✔
THINK IT THROUGH
Read and think through each numbered scenario carefully and then write several sentences in reply to
the question(s) presented. Question 4 requires you to do some Internet research before completing your
answer(s).
1. Describe two ways that the pharmacokinetics of drugs are altered in the elderly patient population and explain what happens to that phase.
2. If a patient had severe diarrhea that drastically increased gastrointestinal motility, what pharmacokinetic phase would be affected? Why?
3. Someone has end-stage renal disease from diabetic nephropathy. What pharmacokinetic phase
would be affected and in what way? Describe how the dose-response curve would change for
such a patient. How would this affect drug dosing?
4. On the Internet, locate information about renal dosing for metformin (commonly prescribed in
the outpatient setting) and cefuroxime (commonly ordered in the inpatient setting). What
changes in dose are necessary for these drugs in patients with kidney dysfunction or failure?
Hint: Manufacturers’ Web sites often have FDA-approved labeling that includes guidelines for
renal dosing. If you work for a hospital or retail pharmacy, look in the professional references
and resources (such as Micromedex or Drug Facts and Comparisons) provided to you online
through your employer.
020-032_PharmEss_02.indd 32
6/29/10 8:47:26 AM