Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
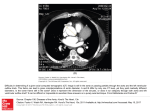
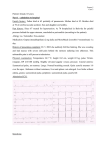
Congestive Heart Failure and Absent Femoral Pulses in Newborns without Coarctation of the Aorta Cuillermo R. Sdnchez, M.D.;* Charles D. Vinocur, M.D.;* Charles U! Wagner, M.D.;* Glenn S. Kaplan, M.D.;* S. David Rubenstein, M. D.;* Fre&rickJ. Fricker, M. D.;t and Yoshie Hashida, M. D . t Two infants with thrombosis of the abdominal aorta are discussed. In each case the presentation was indistinguishable from that in coarctation of the aorta, with heart failure and absent femoral pulses. Surgery in one infant successfully relieved the obstruction. The diagnosis may not be suspected from the history. Aggressive management is indicated. v ascular occlusion in the newborn is an uncommon clinicopathologic entity associated with significant morbidity and mortality.' Several reports have described the development of aortic thrombosis in infants with a history of umbilical artery catheterization and have demonstrated the high mortality associated with this c o m p l i c a t i ~ nWe . ~ ~present two additional cases of aortic occlusion in infancy, emphasizing the clinical presentation as being indistinguishable from that of severe coarctation of the aorta, and demonstrating that aggressive therapy may be successful. infusion were begun, but the infant showed little improvement, and cardiac catheterization with angiography was performed. The study showed a normal aortic arch, a patent ductus arteriosus, and no coarctation. Flow in the descendingaorta was sluggish, and the distal aorta was not visualized. The impression was thrombotic occlusion of the abdominal aorta. Despite heparinization and intensive medical efforts, the infant died 19 hours after admission. At autopsy a large thombus was found occluding the abdominal aorta from a point just proximal to the renal arteries to the bifurcation of the aorta (Fig 1). The thrombus propagated into the left renal artery, and small recent infarcts were present in the left kidney. No inflammation or degeneration was noted in the adjacent aortic wall, and no venous thrombii were present. A 3,700-g male was born at term to a mother with gestational diabetes mellitus. Vaginal delivery was complicated by shoulder dystocia, with asphyxia and Apgar scores of 1and 1 at one and five minutes, respectively. Umbilical artery and vein catheters were inserted, bicarbonate was administered (exact route not known), and the infant was transferred to another hospital. The hemoglobin prior CASE1 An eight-day-old male had been born by cesarean section at term to a mother with gestational diabetes mellitus. Birth weight was 3,300 g, and Apgar scores were 4 and 8 at one and five minutes, respectively. He was meconium stained, but was not intubated, and the umbilical vessels were not catheterized. He was discharged at five days ofage. Two days later respiratory distress developed, and he was transferred to Children; Hospital of Pittsburgh. The systolic pressure was 56 mm Hg in the ri&t arm and 30 m i Hg in &e left leg. there was no murmur, the liver was enlarged, and the femoral pulses were absent. Chest roentgenogram showed cardiomegaly and increased vascular markings. The ECG was normal. M-mode echocardiogram showed diminished left ventricular shortening fraction. Hemoglobin was 16.6 g/dl and hematocrit 51.5 percent; the ~ with polymorphonuclear preponWBC count was 1 2 . 7 0 0 1 ~mm, derance; the platelets were 120,00O/cu mm; PT was 12 seconds (control, 11.5 seconds), and PIT 36 seconds (control, 34 seconds). The clinical impression was coarctation of the aorta and congestive heart failure. Mechanical ventilation, digoxin, and prostaglandin E, *Departments of Pediatrics and Surgery, St. Christopheri Hos ital for Children and Temple University School of Medicine, ~ f i l a delphia. ?Departments of Pediatrics and Pathology. Children's Hospital of Pittsburgh and the University of Pittsburgh - School of Medicine, ~ittsbura. Reprint requests: D1: Sdnchez, Division of Pediatric Cardiology, St. Christopheri Hospital, Philadelphia 19133 I . .....,.. ..... ....-- ..1romFIGURE . ..v.vg.mtr.. .,. -u.uy., rtrrr -..., bus originating at the level of the renal arteries and occluding the distal abdominal aorta. The umbilical arteries remain connected to the umbilicus stump. CHF in Newborns ~ i t h t WCOE~clation l (Sanchez eta) Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21351/ on 05/13/2017 to transfer was 12.9 gldl. In the first day of life, the left leg became cyanotic, but this cleared after immediate removal of the catheter. Seizureswere controlled with phenobarbitaland phenytoin, and the infant's status improved until the fifth day of life, when both legs became transiently cyanotic and the femoral pulses diminished. During the subsequent four days, the femoral pulses became more diacult to appreciate, and on the tenth day of life, signs ofcongestive heart failure and pulmonary hemorrhage developed. Digoxin and antibiotic therapy, and mechanical ventilation were begun, and the infant was transferred to St. Christopher's Hospital for Children. On examination, the infant was hypertonic with occasional spontaneous respirations and frequent seizure activity. Systolic pressure was 140 mm Hg in the left arm and 50 mm Hg in both legs. Small amounts of blood were suctioned from the endotracheal tube. A continuous murmur was present at the left infraclavicular space, the liver was enlarged, and the femoral pulses were absent. The ECG showed biventricular hypertrophy, and a roentgenogram of the chest showed cardiomegaly, with parenchymal haziness and scattered densities compatible with congestive heart failure and pulmonary hemorrhage. A two-dimensional echocardiogram failed to satisfactorily visualize the distal aortic arch. Hemoglobin was 13.6 g/dl and hematocrit, 40.8 percent. The white blood cell count was 14,0001~~ mm, with polymorphonuclear preponderance; and platelets, 58,0001~~ mm. There was occult hematuria. An infusion of prostaglandin E, was begun, but six hours later the infant's status was not improved, and cardiac catheterization with angiography was performed. The study showed a normal aortic arch and complete occlusion of the distal abdominal aorta proximal to the ostia of the renal arteries (Fig2).Thmmbolytictherapy was not initiated because d b d a M&rr h i s . but in view of hwertension and CNS FIGURE 2. Angiogram m me aescenalng aorta in the posteroanterior projection showing complete occlusion of the distal abdominal aorta beyond the origin of the superior mesenteric artery. The renal arteries do not opacify. irritability, surgical embolectomy was attempted via a transverse lower abdominalincision and transperitonealapproach. The abdominal aorta was opened just above the level of the bifurcation, and a large thrombus was removed. Smaller thrombi were also removed from both iliac arteries with Fogarty catheters. There was prompt resolution of the systemic hypertension, and appearanceofexcellent pulses in the lower extremities. Heparin therapy was begun eight hours after surgery and was continued for three days. Neurologic problems persisted which required adjustment of medications. Seven weeks after surgery, the infant was discharged with normal blood pressure and pulses. Thrombotic occlusion of the abdominal aorta in infants is rare, and has been observed in association with umbilical artery ~atheterization,'~as well as in cases where the umbilical vessels had not been m a n i p ~ l a t e d . ' . ~Sepsis, '~ polycythemia, maternal diabetes, dehydration, and clotting factor abnormalities have been considered to play a role in the etiology.'."," In those patients with no history of umbilical artery catheterization, it has been suggested that thromboembolic phenomena may b e related to the changes in the circulation at birth,'.u with emboli originating in a patent ductus arterios~s'.'."'~." or in the umbilical vein." Our two patients illustrate the typical presentation and rapid deterioration characteristic of this disorder. The nature of the problem in case 1 was unsuspected, while in case 2 it was suspected from the history. In both cases the role of maternal diabetes and perinatal asphyxia in the development of aortic thrombosis must remain speculative, but in case 2 the umbilical artery catheter and hypertonic fluid infusions must b e considered contributing hctors. Polycythemia was not present in either infant. Although in our cases the diagnosis was confirmed by angiography, other investigators have used Doppler blood flow and echocardiography as well as radionuclide perfusion studies6 to diagnose the condition noninvasively, thus avoiding the use of angiographic contrast media that could decrease the chances of survival. Although conservative management has proven successful in cases of peripheral occlusive disorders in infants,',' we are not aware of survival of any infant with symptomatic occlusion of the abdominal aorta with medical therapy alone. It is possible that thrombolytic may provide an alternative to the management of these critically ill infants, but success may depend on early recognition and diagnosis. It is questionable whether thrombolytic therapy could have been successfully administered in case 2 in view of signs of pulmonary hemorrhage. The value of postoperative anticoagulation or thrombolytic therapy remains to b e defined. The clinical course of these two infants demonstrates that thromboembolic aortic occlusion must b e suspected in any infant who presents with signs suggestive ofcoarctation ofthe aorta, and that aggressive surgical management of the symptomatic infant can successfully relieve the obstruction. Since submitting this manuscript, a report has appeared" describing the failure of intra-arterial thrombolytic therapy to induce clot lysis in a newborn with aortic occlusion. Failure was attributed to inability to induce a hyperfibrinolytic state due to physiologic reduction in plasminogen levels. CHEST 1 83 I 4 1 Aprll, 1983 Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21351/ on 05/13/2017 688 ACKNOWLEDGMENT: We wish to acknowledge the assistance provided by Marianna Donleavy in the preparation of the manuscript REFERENCES 1 Gross RE. Arterial embolism and thrombosis in infancy. Am J Dis Child 1945; 70:61-73 2 Anderson VM, Harris PJ. Thrombotic occlusion of the aorta in infants of diabetic mothers [abstract]. Pediatric Pathology Club Fall Meeting, Providence, RI. Oct 11-13, 1979. 3 Henry CG, Gutierrez F, Lee JT, Hartmann AF, Bell MJ, Bower RJ. et al. Aortic thrombosis presenting as congestive heart failure: An umbilical artery catheter complication. J Pediatr 1981; 98:820-22 4 Doshi U, Bhat R, Rao S, Flanigan D, Vidyasagar D. Neonatal aortic thrombosis [Letter]. J Pediatr 1981; 99:1002-03 5 Bhat R, Fisher E, Doshi U, Roza S, Sepehri B, Flanigan P, et al. Neonatal abdominal aortic thrombosis. Crit Care Med 1981; 9:858-61 6 O'Neill JA, 'Neblett WW 111, Born ML. Management of major thromboembolic complications of umbilical artery catheters. J Pediatr Surg 1981; 16:972-78 7 Stout C, Koehl G. Aortic embolism in anewborn infant. Am J Dis Child 1970; 120:74-76 8 Ordway NK, Stout LC. Thromboembolus to abdominal aorta in a neonate. J Pediatr 1973; 82:143-48 9 Bjarke B, Herin P, Blomback M. Neonatal aortic thrombosis: a possible clinical manifestation of congenital antithrombin 111 deficiency. Acta Paediatr Scand 1974; 63:297-301 10 Knowlson GT, Marsden HB. Aortic thrombosis in the newborn period. Arch Dis Child 1978; 53164-66 11 Oppenheimer EH, Avery ME. Clinical pathological conference. J Pediatr 1968; 73:143-49 12 Henriksson P, Wesstrom G, Hedner U. Umbilical artery catheterization in newborns: 111. Thrombosis-a study of some ~ r e d i s ~ o s i nfactors. g Acta Paediatr Scand 1979; 68:719-23 13 Woodward JR, Patterson JH, Brinsfield D. Renal artery tbrombosis in newborn infants. Am J Dis Child 1967; 114:191-94 14 McFaul RC, Keane JF, Nowicki ER, Castaneda AR. Aortic thrombosis in the neonate. J Thorac Cardiovasc Surg 1981; 81:334-37 15 Delaplane D, Scott JP, Riggs TW, Silverman BL, Hunt CE, Urokinase therapy for a catheter-related right atrial thrombus. J Pediatr 1982; 100:149-52 16 Corrigan JJ Jr, Allen HD, Jeter M, Malone JM. Aortic thrombosis in a neonate: failure of urokinase thrombolytic therapy. Am J Pediatr Hematol Oncol 1982; 4:243-47 Paroxysmal Nodal Reentrant Tachycardia* Surgical Cure with Preservation of Atrioventricular Conduction Joaquin Marquez-Montes, M.D.;Juan J. Rufilanchas, M . D . ; Juan J. Esteve, M . D . ; Lour&s Alvarez, M . D . ; Juan Benezet, M . D . ; Raul Burgos, M . D . ; and Diego Figuera, M . D . , EC.C.I! *From the Division of Cardiology and Cardiovascular Sur e Centro Nacional de Especialidades Medie~Quirurgicasf e y ; Seguridad Social, Clinica Puerta de Hierro (Universitary Hospital), Madrid, Spain. 690 In a patient with repetitive disabling tachycardias refractory to pharmacologic treatment, t h e electrophysiologic study suggested t h e existence of atrioventricular nodal reciprocating tachycardia. D u r i n g ventricular pacing, e n doepicardial mapping of t h e lower atrium showed t h e atrial breakthrough point in a n a r e a of t h e lower interatrial septum close to t h e AV node crista. A selective atriotomy was performed. T h e postoperative electrophysiologic studies showed absence of ventriculoatrial conduction a t several ventricular pacing rates, while antegrade conduction is preserved. f i e patient remained free of arrhythmias 21 months after surgery, taking n o antiarrhythmic drugs. ectrophysiologic studies using programmed stimulaE l tion,14 endoepicardial m a p p i n g , ' . h n d surgical results"' have led to a better knowledge of AV junctional reciprocating tachycardias. There is more experience in t h e surgical treatment of AV junctional reciprocating tachycardias incorporating Kent bundles in t h e circuit. However, those tachycardias with intranodal mechanism o r those incorporating other types of accessory pathways are less wellknown, and surgical treatment experience is limited.&" T h e surgery in the latter type ofAV reciprocating tachycardias basically d e p e n d s o n t h e surgical interruption o r cryoablation of t h e His bundle, as demonstrated by Harrison e t a18 and Klein e t al.' Pritchett e t all0 and Ward e t al" have recently reported surgical correction of arrhythmia while preserving AV conduction. We recently operated o n a patient with recurrent AV reciprocating tachycardia which was refractory to medical treatment, using endoepicardial mapping of t h e lower atrium close to the AV junction prior to AV interruption of t h e tachycardia circuit. T h e patient remained free of arrhythmias 21 months after surgery, with preserved AV conduction. The patient was a 62-year-old woman with no clinical or hemodynamic evidence of heart disease, who had had bouts ofpalpitations since 1966. Initially, the tachycardia appeared once or twice a month, lasted for 15 to 30 minutes, and remitted spontaneously. Since 1975 the tachycardia episodes had become more frequent (five to six per month) and lasted longer. From 1979on, the crises increased to three or four per week, rangingfrom three to 12 hours, with occasional syncope. Furthermore, the patient showed evidence of severe impairment of her quality of life and was unable to perform her usual activities. The arrhythmia remitted temporarily after intravenous (IV) administration of verapamil (10 mg), ajmaline (1 mglkg), or mexiletine (250 mg as single doses). Multiple oral antiarrhythmic drugs were used without preventing tachycardia, the only ones showing some effect being arniodarone (600mg/day)and quinidine sulfate (1g/day), or the association of digoxin (0.25 mg/day) with verapamil (240 mg/ day), which lengthened the intercrisis interval and shortened the crises. Preoperative Electrophysiologic Study This study was camed out to assess the mechanism of arrhythmia and the action antiarrhythmic drugs and diverse modalities ofcardiac pacing. The basal ECG showed sinus rhythm with 0.12-sec P-R interval, left anterior hemiblock and occasionally right bundle branch block (Fig LA). All antiarrhythmic medication was suspended one week before the study. Three multipolar electrode catheters were inserted Paroxysmal Nodal Reentrant Tachycardia (Marquez-Monteseta/) Downloaded From: http://publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21351/ on 05/13/2017