Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
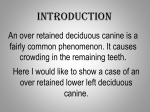
Information Sheet Regarding the Management of Lingually Displaced Mandibular Canine Teeth in Young Dogs Puppies are often presented to a practice for first or second vaccinations with significant bite defects. It is extremely important that practitioners examine the bite at the first opportunity to ensure that the owner is informed that a problem is present and to allow them to contact the breeder and advise them at the earliest opportunity of the difficulty. We see a significant number of puppies in which a bite defect is identified at the second vaccination by the owner’s practice but is missed at the first vaccination by the breeder’s practice. This causes some difficulties as you can imagine. Puppies whose deciduous canine teeth are displaced lingually will generally have some form of obvious traumatic injury to the hard palate or to the gingiva surrounding the upper canine/upper incisors. It is possible that the bite defect can be a combination of lingual displacement of the deciduous lower canine teeth and short mandibles. The treatment does not vary for this additional difficulty. Our advice is to remove the deciduous lower canines as soon as possible. The principle of removing these deciduous canine teeth at the earliest opportunity is based on the following factors. 1. We want to eliminate the immediate trauma and pain damage to the hard palate. This is very painful to the pups and, although they may be stoical enough not to show external difficulties, may well resent closure of the mouth. They tend to hold the mouth open if possible so that their canine teeth do not make contact with the hard palate at all times. Removal will resolve this difficulty immediately. 2. We wish to remove the interlock that occurs between the lower and the upper jaws when the lower canine teeth are lodged into pits into the hard palate. This interlock prevents rostral growth of the mandible at a time when this growth is at its most significant. Rostral growth of the mandible comes from a growth plate at the angle of the jaw. Any canine interlock will prevent rostral growth and result in ventral bowing. 3. Removal of the lower deciduous canine teeth via a lateral flap and bone plate ostectomy with create a space for the permanent lower canines to erupt into. The permanent canines erupt on the lingual side of the deciduous canines and, if the deciduous canines are in a poor position, the permanent canines must inevitably be worse. Removal of the deciduous canines therefore is advised as soon as is practical. This could be as early as 8 weeks. The later this surgery takes place the less time there is to influence events as regards eruption of the permanent teeth. This eruption of the permanent lower canines happens between 22 and 26 weeks in most breeds. Removal of the deciduous canines is complex surgery. In general terms the length of the root is three times the length of the visible crown. To successfully influence events all of the tooth must ©DentalVets 2013 be removed without any resort to instrumentation on the lingual aspect. The reason for this is that instrumentation on the lingual aspect of the deciduous canine will damage the soon-to-erupt permanent canine. The deciduous mandibular canine tooth (teeth) should be removed via a wide based mucogingival flap on the buccal aspect and removal of the buccal bone plate before the deciduous canine tooth can be “flipped” out of the socket. The area is then irrigated before closure with absorbable sutures. The genetic nature of this defect is relatively complex but is considered to be an autosomal recessive mutation. It usually follows a Mendelian pattern in its penetrance and this generally means that 1 puppy in 4 in any affected litter will show the problem whilst the others will carry the recessive gene. In addition both parents will be recessive carriers although their dentition may look normal. Clearly breeders producing such litters need to be advised of this and the fact that the siblings and parents of the affected puppy may look normal but are not. There is a further difficulty with insurance cover with many of these puppies. If the puppies are not insured before the problem is diagnosed it must be considered pre-existing by the insurance company. This will result in a rejection of any claim subsequently submitted. In addition, those owners arriving with 6 weeks free insurance should be advised to keep the insurance running as, if they change companies, the problem of a pre-existing condition again applies. For those owners who are not insured there is a clear duty on the breeder to refund the majority of the purchase price. This is something that many new owners are reluctant to do but, armed with an expert report including photographs, it is hard for the breeder to refuse that there is a problem. An expert report can only be rebutted by a contrary expert report. Norman W Johnston BVM&S FAVD DipAVDC DipEVDC MRCVS RCVS, American and European Specialist in Veterinary Dentistry ©DentalVets 2013