Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
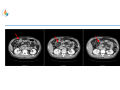
Case Presentation Stage II Transverse Colon cancer without high risk factor Joo Han Lim Dept of Medical Oncology Inha University School of Medicine and Hospital Stage II Colon Cancer Subgroups • 5 year survival after surgical resection alone is: • Stage I : 85-05% • Stage II : 60-80% • Stage III : 30-60% ESMO Clinical Practice Guidelines 2013 Clinical Case • 36-years-old man • Abdominal pain; 1 month /5kg weight loss • ECOG Performance status 0 • Never colonoscopy • No hepatosplenomegaly • No palpable lymph nodes Past Medical History No Medications No Social history Unmarried Current smoker – total 20 Pack years Occasional social alcohol: average less than three drinks per week Family history No cancers found in first degree or second degree relatives • Colonoscopy; ulcerofungating mass in proximal transverse colon • no definite obstruction, but there was severe luminal narrowing. • Scope could go through the lesion. • moderately differentiated adenocarcinoma. PET CT Op findings • Op date 25/AUG/2014 • Laparoscopic transverse colectomy with lymphadenectomy • 5.5cm sized ulcerofungating mass with severe pericolic infiltration, located on mesocolic border of transverse colon • Grossly negative regional lymph node • No distant metastasis Pathology Report • • • • • • • • • • Well differentiated adenocarcinoma 5cm size Depth of invasion: invades pericolic adipose tissue (pT3) Resection margin: free / safety margin: prox 6cm, distal 3cm Regional lymph node metastasis: no metastasis in all 12 regional lymph nodes (0/12) Lymphatic invasion: not identified Venous invasion: not identified Perineural invasion: not identified Pathologic stage pT3pN0 IHC for microsatellite instability MLH1: positive MSH2: positive MSH6: positive PMS2: positive • 8/SEP/2014 • RLQ area abdomen huge abscess pocket • Intraabdominal drainage due to postoperative intraabdominal abscess Adjuvant chemotherapy? • The surgeon referred to the department of medical oncology for consideration of adjuvant chemotherapy after recovery of infection. • The surgeon concerned about the possibility of recurrence. The patient’s operation finding was not favorable. Post op intra-abdominal infection: high risk factor? • According to pathologic staging, there was nothing related to high risk feature. Stage II A, B, C (T3 N0 M0, T4 a-b N0 M0) Standard treatment options: (i) Wide surgical resection and anastomosis. (ii) Following surgery, adjuvant therapy should not be routinely recommended for unselected patients. In high-risk patients who present at least one of the previously mentioned clinical high-risk features (see above), adjuvant therapy could be considered in clinical practice. The general consensus suggests that patients with stage II are considered at high risk if they present at least one of the following clinical characteristics: lymph nodes sampling <12; poorly differentiated tumour; vascular or lymphatic or perineural invasion; tumour presentation with obstruction or tumour perforation and pT4 stage ESMO Clinical Practice Guidelines 2013 • Discussed patient • We concluded to treat this patient with adjuvant chemotherapy. • Do we treat and if so, with what regimen? • He had received 6 cycles of LF chemtherapy (adjuvant)
















![Provider Bulletin: [Subject]](http://s1.studyres.com/store/data/000975616_1-3f817b14a0d66ce9d7f5c5c63cd4030c-150x150.png)