Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Telecommunications relay service wikipedia , lookup
Lip reading wikipedia , lookup
Hearing aid wikipedia , lookup
Hearing loss wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Sensorineural hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
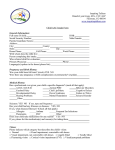
Journal of Advanced Clinical & Research Insights (2015), 2, 189–192 ORIGINAL ARTICLE Audiometric analysis of type and degree of hearing impairment and its demographic correlation: A retrospective study Sumanth Kanjikar1, Anil Doddamani2, Rajkamal Malige1, Nagbhushan Reddy1 Department of ENT, Bidar Institute of Medical Sciences, Bidar, Karnataka, India, 2Department of ENT, Employees State Insurance Corporation Medical College, Gulbarga, Karnataka, India 1 Keywords Audiometry, conductive, demography, hearing impairment, screening Correspondence Dr. Sumanth Kanjikar, Assistant Professor, Department of ENT, BRIMS, Bidar, Karnataka, India. e-mail: [email protected] Received 27 July 2015; Accepted 5 September 2015 doi: 10.15713/ins.jcri.76 Abstract Background: This retrospective study was done to know the demographic characteristics of patients suffering from hearing loss. The type and degree of hearing impairment were correlated with the demographic characteristics. Aims and Objectives: (1) To establish the type and degree of hearing loss in patients (2) evaluate age and gender-wise differences with respect to type and degree of hearing loss. (3) Correlate age of a patient with degree of hearing impairment. Materials and Methods: Audiometric data of 252 patients were taken. Demographic characteristics were compared with types and degrees of hearing impairment. Results: Sensorineural hearing loss (SNHL) type was the highest with 163 (66.5%) out of 252 cases. Males were more affected by SNHL, mixed and conductive types. In the SNHL category, the highest number of cases belonged to the 51-60 yeas age group (24.5%) whereas in the conductive and mixed types of hearing loss, the maximum patients were found in the 21-30 age group (51.5% and 25.6% respectively). Least number of cases was in the age groups of 1-10 years followed by 81-90 years. Bilateral impairment was more than unilateral impairment. Conclusion: Our study concludes that men are more affected than women, bilateral involvement is more common than unilateral, and SNHL type is the most common type of hearing impairment. Introduction Hearing impairment is one of the most prevalent chronic conditions after hypertension and arthritis.[1] Over 5% of the world’s population - 360 million people - has disabling hearing loss (328 million adults and 32 million children).[2] The prevalence of hearing impairment is increasing with increase in the ageing population and exposure to noise, both occupational and at leisure. Hearing loss can impair the communication skills of the affected person. The individual thus suffers both physically and socially. In relation to public health, hearing impairment is known to be associated with depression, diabetes and dementia.[1] Approximately, one-third of people over 65 years of age are affected by disabling hearing loss. The prevalence in this age group is greatest in South Asia, Asia Pacific and sub-Saharan Africa.[2] There are only a few audiometry based studies about the demographic characteristics of patients with hearing impairment. This hospital-based retrospective study was done to know the demographic characteristics of patients suffering from hearing loss. There was an attempt to correlate the type and degree of hearing impairment with the demographic characteristics. Methods This is a retrospective study on the audiometric data of 252 patients in the year 2013, who visited the outpatient Department of Otolaryngology of Bidar Institute of Medical Sciences, with different types and degrees of hearing impairment. The data were compiled and groups based on demographic characteristics such as age, [Graph 1] and sex were compared with types and degrees of hearing impairment. The age of the patients in this study ranged between 1 and 90 years. The types of hearing impairment were categorized as sensorineural hearing Journal of Advanced Clinical & Research Insights ● Vol. 2:5 ● Sep-Oct 2015189 Kanjikar, et al. Audiometric analysis Table 1: Distribution of study participants based on the type of hearing impairment Type SNHL n (%) 163 (66.5) Conductive 33 (13.5) Mixed 39 (15.9) Mixed+SNHL 5 (2) Others 5 (2) SNHL: Sensorineural hearing loss Graph 1: Age group distribution (in %) of study participants loss (SNHL), conductive, mixed, mixed + SNHL, and others (conductive loss in one ear and mixed or SNHL in the other) [Table 1].[3] In this study, we also considered unilaterality and bilaterality of hearing impairment.[3] The degree of hearing impairment was graded as mild (25-40 dB threshold), moderate (41-55 dB threshold), moderately severe (56-70 dB threshold), severe (71-90 threshold), and profound (>90 dB threshold).[4] All the observations were tabulated and subjected to statistical analysis using Chi-square test. Results Age group distribution graph when observed reveals that more number of patients belonged to the 51-60 years age group accounting for 21.8% of total cases, followed by 21-30 years age group with 20.8%. Least percentage of cases belonged to the 1-10 years age group with 0.8% cases [Graph 1]. The average age of the patients was 45.8 years. Gender distribution showed that males were more affected with 66.9% of total cases compared to females with 33.1% of cases. Among the type of hearing impairment, SNHL was seen in 163 (66.5%) out of 252 cases followed by 39 (15.9%) cases of mixed type. Conductive type of hearing loss was seen in 33 (13.5%) cases. The other types of hearing impairment were contributing to 2% of cases [Table 1]. When we compared gender-wise distribution of various types of hearing impairment using Chi-Square test, we observed that SNHL, mixed and conductive types of hearing impairment affected more males, i.e., 71.2%, 69.2% and 51.5%, respectively, compared to females. This difference showed statistically significant P = 0.04 [Table 2]. Age wise comparison of various types of hearing impairments among the study participants showed that in the SNHL category, the highest number of cases belonged to the 51-60 yeas age group(24.5%) whereas in the conductive and mixed types of hearing loss, the maximum patients were found in the 21-30 age group (51.5% and 25.6% respectively). Least number of cases was in the age groups of 1-10 years followed by 81-90 years. This difference in age and type distribution showed significant P = 0.006 [Table 3]. 190 Table 2: Comparison of gender‑wise distribution of various types of hearing impairment using Chi‑square test SNHL Sex (n (%)) Total Chi‑square P value n (%) value Males Females 116 (71.2) 47 (28.8) 163 (100.0) 8.235 0.04* Conductive 17 (51.5) 16 (48.5) 33 (100.0) Mixed 27 (69.2) 12 (30.8) 39 (100.0) 4 (40.0) 6 (60.0) 10 (100.0) Type Others Total 164 (66.9) 81 (33.1) 245 (100.0) *Statistically significant, SNHL: Sensorineural hearing loss In our study population, we also observed that bilateral hearing loss accounted for 89.8% of total cases compared to 10.2% of unilateral cases. Bilateral involvement was observed in high percentage of the population in all the types of hearing impairment as shown in Table 4. When the types of hearing loss were compared with degree of loss we observed that 27.6% of SNHL, 54.5% of conductive and 60.0% of mixed + SNHL type patients showed moderate degree of loss, whereas 51.3% of mixed showed moderately severe degree of loss. This when compared showed a statistically significant difference with a P < 0.001 [Table 5]. Discussion In our study, we found that the age distribution of hearing loss patients showed two peaks in the 51-60 age group (21.8%) followed by 21-30 age group (20.8%). This being a hospital based retrospective study based on pure tone audiometry of patients presenting to the outpatient department with hearing loss, prevalence of hearing loss in the population and in the different age groups cannot be commented on, but the distribution of hearing loss in this study is a fair indication of the prevalence of hearing loss in different age groups and both the sexes. Different studies have shown that the prevalence of hearing loss increased with age among all demographic groups.[5] In our study, the first peak was seen in the 21-30 age group maybe because of the higher incidence of noise exposure in the working class population and smoking in this age group.[6-8] The 51-60 age group peak could be due to age-related pathophysiologic changes in the cochlea.[9] The data collected by Agrawal et al. in their survey of the American population also suggest that the Journal of Advanced Clinical & Research Insights ● Vol. 2:5 ● Sep-Oct 2015 Kanjikar, et al. Audiometric analysis Table 3: Age wise comparison of various types of hearing impairments among the study participants using Chi‑square test Type 71‑80 16 (9.8) 81‑90 7 (4.3) Total n (%) Chi‑square value P value 61‑70 26 (16.0) 163 (100.0) 45.111 0.006* 2 (6.1) 1 (3.0) 0 (0.0) 0 (0.0) 33 (100.0) 5 (12.8) 6 (15.4) 5 (12.8) 1 (2.6) 0 (0.0) 39 (100.0) 1 (10.0) 4 (40.0) 1 (10.0) 1 (10.0) 0 (0.0) 10 (100.0) 27 (11.0) 52 (21.2) 33 (13.5) 18 (7.3) 7 (2.9) 245 (100.0) SNHL 1‑10 2 (1.2) 11‑20 12 (7.4) 21‑30 23 (14.1) Age (years) (n (%)) 31‑40 41‑50 51‑60 18 (11.0) 19 (11.7) 40 (24.5) Conductive 0 (0.0) 4 (12.1) 17 (51.5) 7 (21.2) 2 (6.1) Mixed 0 (0.0) 6 (15.4) 10 (25.6) 6 (15.4) Others 0 (0.0) 1 (10.0) 1 (10.0) 1 (10.0) Total 2 (0.8) 23 (9.4) 51 (20.8) 32 (13.1) *Statistically significant, SNHL: Sensorineural hearing loss Table 4: Comparison of distribution of different types of hearing impairments with respect to the affected sides Type SNHL Side affected (n (%)) Total Chi‑square P value n (%) value Unilateral Bilateral 6 (3.7) 157 (96.3) 163 (100.0) 29.926 <0.001* Conductive 7 (21.2) 26 (78.8) 33 (100.0) Mixed 12 (30.8) 27 (69.2) 39 (100.0) 0 (0) 5 (100.0) 5 (100.0) 0 (0.0) 5 (100.0) 5 (100.0) Mixed+SNHL Others Total 25 (10.2) 220 (89.8) 245 (100.0) *Statistically significant, SNHL: Sensorineural hearing loss prevalence of hearing loss is increasing among the younger age groups (20-29 and 30-39). This correlates with the findings of our study.[5] Evidence from several studies suggests that age-related hearing loss differs between men and women.[9,10] In our study, 66.9% of the participants were male and 33.1% were females. When we compared gender-wise distribution of various types of hearing impairment using Chi-square test, we observed that SNHL, mixed and conductive types of hearing impairment affected more males, i.e. 71.2%, 69.2% and 51.5%, respectively, compared to females. This difference showed statistically significant P value of 0.04. This suggests that male sex itself is a risk factor for developing hearing loss. This correlates well with other studies.[1] A study on Korean population by Hong et al. suggests that being male was independently associated with highfrequency mild hearing impairment.[1] Agrawal et al. conclude that a disproportionate burden of hearing loss is experienced by male and white (and to a lesser extent Mexican American) participants and is manifest in the third decade of life. Their study also suggests that men generally had higher prevalence of bilateral, unilateral, and high-frequency hearing loss across the age range compared with women.[5] It is likely that men have a tendency to experience more occupational noise exposure, more likely to smoke and more prone for other risk factors like smoking and hypertension.[7,8,11] In our study, Bilateral hearing loss accounted for 89.8% of the cases and Unilateral for 10.2% cases. In all types of hearing loss, bilateral involvement was seen more than unilateral loss. In the study by Agrawal et al. they reported that approximately 50% speech frequency hearing loss was unilateral and 50% was bilateral.[5] Though we did not divide the patients into speech frequency and high frequency hearing loss categories, we had significantly more number of patients in the bilateral category. More percentage of people in the bilateral category could be due to the fact that patients with bilateral hearing loss are more likely to come to the hospital seeking help. Unilateral loss may go unnoticed or not considered significant by the patient. Systemic causes like atherosclerosis or Diabetes mellitus are more common which lead to bilateral loss rather than unilateral loss.[12-16] Among the type of hearing impairment, SNHL was seen in 66.5% cases followed by mixed type (15.9%). Conductive type of hearing loss was seen in 13.5% cases. Such a big burden of sensorineural hearing loss cases maybe due to an ageing population,[9] more occupational and recreational noise exposure,[7] increasing hypertension,[11] and diabetes incidence.[13,14] Age wise comparison of various types of hearing impairments among the study participants showed that in the SNHL category, the highest number of cases belonged to the 51-60 yeas age group (24.5%) whereas in the conductive and mixed types of hearing loss, the maximum patients were found in the 21-30 age group (51.5% and 25.6% respectively). Least number of cases was in the age groups of 1-10 years followed by 81-90 years. This again indicated the effect of age on hearing loss of the sensorineural type and effect of occupational noise exposure and smoking in the working class population (21-30 years). We feel that the lesser number of cases in the 1-10 and 81-90 age groups is an underestimate of the true burden of hearing loss in these age groups, as these patients are less likely to visit the hospital for hearing problems because of school in the 1-10 years category and because of other physical disabilities in the older age group. This reiterates the importance of audiometric screening of school going children to detect early onset hearing loss and manage it so that the academic and social performance of these children does not suffer. In our study, most of the patients across the spectrum of the types of hearing loss presented to the hospital when their hearing loss was either moderate degree (27.6% of SNHL, 54.5% of conductive and 60.0% of mixed + SNHL type patients) or of moderately severe degree (51.3% of mixed type). This indicated that either the mild hearing loss is not noticed by most of the patients because it does not cause them significant problems in Journal of Advanced Clinical & Research Insights ● Vol. 2:5 ● Sep-Oct 2015191 Kanjikar, et al. Audiometric analysis Table 5: Comparison of distribution of different types of hearing impairments with respect to the degree of impairment Type Total n (%) Chi‑square value P value Profound 32 (19.60) 163 (100.00) 55.181 <0.001* 0 (0.00) 0 (0.00) 33 (100.00) 20 (51.30) 4 (10.30) 2 (5.10) 39 (100.00) 1 (20.00) 0 (0.00) 0 (0.00) 5 (100.00) Degree UB (n (%)) Mod‑severe Severe 40 (24.50) 19 (11.70) SNHL Mild 27 (16.60) Moderate 45 (27.60) Conductive 13 (39.40) 18 (54.50) 2 (6.10) Mixed 1 (2.60) 12 (30.80) Mixed+SNHL 1 (20.00) 3 (60.00) Others 2 (40.00) 0 (0.00) 2 (40.00) 0 (0.00) 1 (20.00) 5 (100.00) Total 44 (18.00) 78 (31.80) 65 (26.50) 23 (9.40) 35 (14.30) 245 (100.00) *Statistically significant, SNHL: Sensorineural hearing loss their daily activities or there is a tendency to neglect mild hearing loss. In India, many patients with age-related hearing loss don’t seek medical help. Therefore, audiometric screening is necessary in apparently healthy people to detect mild hearing loss so that these persons can be helped by dealing with the correctable causes, taking care of the risk factors and by giving them suitable hearing aids. Agrawal et al. also suggested that audiometric screening is critical to capture the true prevalence of hearing loss, particularly at an early pathogenetic stage among young adults.[5] Conclusion It can be said in conclusion that hearing loss prevalence is increasing globally because of the increase in life expectancy and in the younger age group because of occupational and recreational noise exposure and smoking. It is of utmost importance to detect the mild hearing loss cases early by audiometric screening at the school level for effective management of these cases. The general population has to be made aware of the risk factors for hearing loss like smoking, noise exposure. There is also a need for a crosssectional study in India to estimate the true prevalence of hearing loss. References 1. Hong JW, Jeon JH, Ku CR, Noh JH, Yoo HJ, Kim DJ. The prevalence and factors associated with hearing impairment in the Korean adults: THe 2010-2012 Korea National Health and Nutrition Examination Survey (observational study). Medicine (Baltimore) 2015;94:e611. 2. WHO. Deafness and Hearing Loss. Fact Sheet N 300. Available from: http://www.who.int/mediacentre/factsheets/fs300/en/. [Last accessed on 2015 Aug 17; Last updated on 2015 Mar]. 3. Shemesh R. Hearing impairment: Definitions, assessment and management. In: Stone JH, Blouin M, editors. International Encyclopedia of Rehabilitation. 2010. Available from: http:// www.cirrie.buffalo.edu/encyclopedia/en/article/272/. [Last accessed on 2015 Sep 12]. 4. Dhingra PL, Dhingra S. Diseases of ear, nose and throat and head and neck surgery. Diseases of Ear Hearing Loss. 6th ed. New Delhi: Elsevier Health Sciences; 2014. 192 5. Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences by demographic characteristics among US adults: Data from the National Health and Nutrition Examination Survey, 1999-2004. Arch Intern Med 2008;168:1522-30. 6. Daniel E. Noise and hearing loss: A review. J Sch Health 2007;77:225-31. 7. Morata TC. Young people: THeir noise and music exposures and the risk of hearing loss. Int J Audiol 2007;46:111-2. 8. Kumar A, Gulati R, Singhal S, Hasan A, Khan A. The effect of smoking on the hearing status-A hospital based study. J Clin Diagn Res 2013;7:210-4. 9. Helfer KS. Gender, age, and hearing. Semin Hear 2001;22:271-86. 10.Kim S, Lim EJ, Kim HS, Park JH, Jarng SS, Lee SH. Sex differences in a cross sectional study of age-related hearing loss in Korean. Clin Exp Otorhinolaryngol 2010;3:27-31. 11.Gates GA, Cobb JL, D’Agostino RB, Wolf PA. The relation of hearing in the elderly to the presence of cardiovascular disease and cardiovascular risk factors. Arch Otolaryngol Head Neck Surg 1993;119:156-61. 12.Fischer ME, Schubert CR, Nondahl DM, Dalton DS, Huang GH, Keating BJ, et al. Subclinical atherosclerosis and increased risk of hearing impairment. Atherosclerosis 2015;238:344-9. 13.Dalton D, Cruickshanks K, Klein R, Klein B, Wiley T. Association of NIDDM and hearing loss. Diabetes Care 1998;21:1540-4. 14.Fukushima H, Cureoglu S, Schachern PA, Paparella MM, Harada T, Oktay MF. Effects of type 2 diabetes mellitus on cochlear structure in humans. Arch Otolaryngol Head Neck Surg 2006;132:934-8. 15.Ishii EK, Talbott EO, Findlay RC, D’Antonio JA, Kuller LH. Is NIDDM a risk factor for noise-induced hearing loss in an occupationally noise exposed cohort? Sci Total Environ 1992;127:155-65. 16.Makishima K, Tanaka K. Pathological changes of the inner ear and central auditory pathway in diabetics. Ann Otol Rhinol Laryngol 1971;80:218-28. How to cite this article: Kanjikar S, Doddamani A, Malige R, Reddy N. Audiometric analysis of type and degree of hearing impairment and its demographic correlation: A retrospective study. J Adv Clin Res Insights 2015;2:189-192. Journal of Advanced Clinical & Research Insights ● Vol. 2:5 ● Sep-Oct 2015