Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
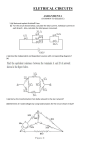
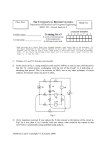
Isolation and Characterization of Atrioventricular Nodal Cells From Neonate Rabbit Heart Xiao Ye Sheng, MD, MSc*; Yang Qu, MD, PhD*; Pauline Dan, PhD; Eric Lin, PhD; Linda Korthout, MSc; Aaron Bradford, BSc; Leif Hove-Madsen, PhD; Shubhayan Sanatani, MD, FRCPC; Glen F. Tibbits, PhD Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 Background—The properties of the atrioventricular (AV) node in the neonate heart and its role in unique pediatric cardiac arrhythmias such as junctional ectopic tachycardia (JET) are poorly understood. This is due in large part to the dearth of information on the structure and physiology of the AV node in the immature myocardium. Methods and Results—Sinoatrial nodal cells (SANCs), AV nodal tissues, and myocytes (AVNCs) were obtained from neonatal (10-day-old) rabbits, and the histological, immunohistological, and electrophysiological properties were characterized in detail. Masson’s trichrome histological staining clearly delineated AV nodal structures including the inferior nodal extension, compact node, and the bundle of His region. AV tissue sections and AVNCs were immunolabeled against neurofilament 160 (NF160), connexin 43 (Cx43), hyperpolarization-activated, cyclic nucleotide modulated channel (HCN4), sodium/calcium exchanger, ryanodine receptor, sarcoplasmic/endoplasmic reticulum Ca2⫹ pump (SERCA), and phospholamban (PLB). In AVNCs with triple-positive NF160, SERCA, and PLB labeling, SERCA and PLB were found with high degrees of colocalization. The majority (59%) of NF160-positive AVNCs were found to coexpress HCN4. NF160 and HCN4 expression was found to be even higher in SANCs, where 88% of SANCs exhibited coexpression. Spontaneous action potentials recorded from isolated neonatal AVNCs were uniformly of the atrionodal type, showing none of the action potential heterogeneities found in the mature heart. Current recordings found the hyperpolarization-activated funny current (If) in 55% (11 of 21 cells) of AVNCs, consistent with the immunocytochemistry results. Conclusions—This represents the first detailed electrophysiological and immunohistological report of the neonatal AV node and lays the groundwork for a better understanding of heart rate regulation and unique arrhythmias in the neonate heart. (Circ Arrhythm Electrophysiol. 2011;4:936-946.) Key Words: cardiac arrhythmogenesis 䡲 pacemaking cells 䡲 HCN4 䡲 NCX 䡲 NF160 䡲 compact node 䡲 inferior nodal extension T junction proteins and fast-acting voltage-gated ion channels impart specific electric characteristics of each region.7–9 he atrioventricular (AV) node represents the sole conduction pathway between the atrial and ventricular compartments of the normal adult heart. The AV node is localized within the triangle of Koch, bordered by the coronary sinus, tendon of Todaro, and tricuspid valve.1 Within this diminutive area lie considerable structural and functional heterogeneities that determine the complex physiological functions of the AV node. Functionally and histologically, the AV node can be further subdivided into the inferior nodal extension (INE), compact node (CN), and lower nodal bundle.2– 4 This intricate structure forms the slowly conducting electric pathway that provides the critical AV delay that ensures adequate diastolic ventricular filling.5,6 Differential expression of gap Clinical Perspective on p 946 In addition to the crucial role of the AV node in providing the required AV delay, the AV node also plays a critical role as a secondary pacemaking site, preserving cardiac function in the absence of sinoatrial (SA) pacemaker activity.10 Despite the ability of AV node to act as a fail-safe mechanism, pathology within the AV node can be a significant source of life-threatening cardiac arrhythmias. Cardiac morphology and function continues to develop after birth and specific arrhythmias occur more frequently in certain developmental stages. Received April 5, 2011; accepted September 12, 2011. From Cardiovascular Sciences, Child and Family Research Institute, Vancouver, British Columbia, Canada (X.Y.S., Y.Q., P.D., E.L., L.K., A.B., S.S., G.F.T.); Molecular Cardiac Physiology Group, Simon Fraser University, Burnaby, British Columbia, Canada (X.Y.S., Y.Q., P.D., E.L., A.B., G.F.T.); Maastricht University, Maastricht, The Netherlands (L.K.); Cardiovascular Research Center, Hospital de Sant Pau, Barcelona, Spain (L.H.-M.); and Pediatric Cardiology, BC Children’s and Women’s Hospital, Vancouver, British Columbia, Canada (S.S.). *Drs Sheng and Qu contributed equally to this work. The online-only Data Supplement is available at http://circep.ahajournals.org/lookup/suppl/doi:10.1161/CIRCEP.111.964056/-/DC1. Correspondence to Glen F. Tibbits, PhD, Molecular Cardiac Physiology Group, Simon Fraser University, Burnaby, BC, V5A 1S6, Canada. E-mail [email protected] © 2011 American Heart Association, Inc. Circ Arrhythm Electrophysiol is available at http://circep.ahajournals.org 936 DOI: 10.1161/CIRCEP.111.964056 Sheng et al AV Nodal Cells in Neonate Heart 937 Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 Figure 1. Neonatal rabbit atrioventricular (AV) nodal histology. A, Ten-day rabbit endocardium with anatomic landmarks as indicated: superior vena cava (SVC); inferior vena cava (IVC); tendon of Todaro (tT); coronary sinus (CS); fossa ovalis (FO); aorta (Ao); and tricuspid valve (TV). The approximate location of the inferior nodal extension (INE) and the compact node (CN) of the AV nodal area are shown in the boxed area. The orientation is also indicated by the arrows in the upper left-hand corner. Masson’s trichrome staining of 3 sections taken from the neonate AV nodal area are shown in B (S125), C (S165), and D (S302), in which red indicates muscular tissue, blue indicates collagen/connective tissue, black indicates nuclei, and white indicates fibrous tissue. B through D illustrate atrial muscle (AM), aortic valve (AoV), central fibrous body (CFB), ventricular muscle (VM), and a specific regions of the AV nodal tract; INE (B), compact node (CN) (C), and bundle of His (HB) (D). However, the specific differences between the immature and mature heart are poorly understood. In the present report, we further a developmental AV nodal model using electrophysiological and immunohistological techniques to investigate the essential components of the funny current and calcium clock hypotheses of pacemaker activity,11 including the hyperpolarization activated, cyclic nucleotide-gated channel (HCN4), sodium/calcium exchanger (NCX), ryanodine receptor (RyR), phospholamban (PLB) and sarcoplasmic/endoplasmic reticulum calcium ATPase (SERCA). AV nodal dysfunctions produce arrhythmias with distinct characteristics at different stages of development. For instance, the presentation of atrioventricular nodal reentrant tachycardia (AVNRT) is distinct in pediatric patients12 due to changes in the electrophysiological properties of the AV node as the heart matures with development.13 The ontogenic differences in AVNRT are believed to be due to a higher incidence of anterograde dual AV nodal pathways in adult patients. Junctional ectopic tachycardia (JET), another arrhythmia consistent with an AV nodal dysfunction, is uniquely associated with open heart surgery for congenital heart defects in infants and young children.14 Nevertheless, for virtually all arrhythmias associated with AV node dysfunction, the agerelated etiology has not been clearly understood. Intensive immunohistochemical, electrophysiological and computational modeling studies have been performed on the intact adult AV node for more than 40 years,2,15,16 whereas the electrophysiological characteristics of single AV nodal cells 938 Circ Arrhythm Electrophysiol December 2011 Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 Figure 2. Immunohistochemistry of the neonate atrioventricular (AV) nodal area. A, B, and C are dual-labeled (NF160 and NCX) images of sections taken from approximately S125, S165, and S302 as shown in Figure 1A, respectively. Locations of anatomic landmarks are indicated: atrial muscle (AM), aortic valve (AoV), inferior nodal extension (INE), central fibrous bundle (CFB), ventricular muscle (VM), and compact node (CN). High-magnification (63⫻) images are provided of the INE (D, I, II, and III), CN (E, I, II, and III), and bundle of His (HB) (F, I, II, and III) for NF160, NCX, Cx43, and HCN4 Abs, respectively. Sheng et al Table 1. AV Nodal Cells in Neonate Heart 939 Immunohistochemical Summary NF160 NCX Cx43 HCN4 Atrial muscle ⫺ ⫹ ⫹⫹ ⫺ Inferior nodal extension ⫹ ⫹⫹ ⫺ ⫹ Compact node ⫹ ⫹⫹ ⫺ ⫹ Bundle of His ⫹ ⫹⫹ ⫹ ⫹ Ventricular muscle ⫺ ⫹ ⫹⫹ ⫺ the neonatal AV node at the histological and cellular levels that provide information that furthers the understanding of ontogenic changes of the cardiac conduction pathway. Methods Heart Excision and Cannulation Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 The experimental protocols used in this study were in accordance with the Canadian Council on Animal Care (CCAC) regulations. The Animal Care Committee of the University of British Columbia approved the use of animals for this study. A total of 15, 10-day New Zealand rabbits were used. Briefly, hearts isolated from 10-day rabbits were cannulated and retrogradely perfused with Solution A. Detailed descriptions of the procedures and solution compositions are provided in the online-only Data Supplement. Histology and Immunohistochemistry Figure 3. Outlines of the structures shown in the Masson’s trichrome and IHC images. Sixteen different sections spanning the region from S105 to S352 are shown in cartoon fashion to highlight areas of the atrioventricular (AV) nodal area vis-à-vis other cardiac structures in the sections. The areas outlined in red and mustard-colored lines include the atrial and ventricular tissues, respectively. The areas colored in blue include the aorta and aortic valves (cyan) and tricuspid valves (dark blue). The fuchsia-colored area is the central fibrous bundle (CFB) and the green-colored region represents the nodal track. Each section is 10 m thick and thus the distance, for example between sections 105 and 126 is ⬇210 m. The 16 images span the region between the 2 long vertical red bars shown in Figure 1A. (AVNCs) were not explored until a method for the isolation of single AVNCs in adult hearts was developed by Hancox and Levi in 1993.17 The extension of these techniques to the investigation of AV conducting mechanisms found in neonates has so far been extremely limited, due primarily to the technical difficulties associated with isolation and characterization of cells from this nodal area in the immature heart. For the present study, we developed an AVNC isolation technique for the 10-day-old (10-day) rabbit heart, which consistently produced a high-yield of spontaneously beating AVNCs. We also performed immunohistochemical and electrophysiological experiments on intact neonatal AV nodal sections and isolated beating AVNCs. The development of these techniques has allowed for detailed characterizations of A rectangular section of right atrial tissue (3⫻5.5 mm) including not only the triangle of Koch but also the aorta and the bundle of His (HB) (see Figure 1A) was excised immediately after Solution A perfusion. The preparation was imbedded in O.C.T Tissue-Tek (No. 4583, Sakura) and frozen in isopentane precooled to ⫺140°C in liquid N2 and then stored at ⫺80°C; 10-m serial cryosections were sliced perpendicular to the long axis of the tricuspid valve (Figure 1A). Sections were mounted onto poly-L-lysine– coated glass slides, fixed with 4% paraformaldehyde for 10 minutes, and quenched with glycine for 10 minutes. Detailed descriptions of the histology and immunohistochemistry procedures are provided in the online-only Data Supplement. Isolation of Single AVNCs and SA Nodal Cells From the Neonate Rabbit Heart Isolation procedures specific to AVNCs were adapted from myocyte isolation protocols used in our laboratory18 for neonatal ventricular myocytes and from AVNC isolation protocols published for adult hearts.17 Enzyme concentrations and perfusion rates were refined to ensure viable, Ca2⫹-tolerant AVNCs and SA nodal cells (SANCs) from the neonate heart. The complete procedure is described in online-only Data Supplement Table S2 and related material. Electrophysiological Recordings Perforated (amphotericin B, 250 g/mL) whole-cell current-clamp and voltage-clamp techniques were used to record spontaneous action potentials and ionic currents (MultiClamp 700A, Axon Instruments, Union City, CA) from isolated single cells as described in the online-only Data Supplement. Immunocytochemistry The excised enzyme-digested rectangular tissue was chopped in a tissue culture dish containing 2% paraformaldehyde for 10 minutes. Cells were quenched by 100 mmol/L glycine for 10 minutes, permeabilized with 0.1% Triton X-100 for 10 minutes, washed with PBS 2⫻ for 10 minutes each, then allowed to settle onto poly-Llysine– coated (No. P5899, Sigma) coverslips for 1 hour at room temperature, followed by primary antibodies incubation overnight at 4°C. Detailed descriptions of the immunohistochemistry procedures are provided in the online-only Data Supplement. 940 Circ Arrhythm Electrophysiol December 2011 Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 Figure 4. Action potential characteristics. A shows the length and width of spindle and rod atrioventricular nodal cells (AVNCs) measured using Image J software (publicly accessed at http://rsbweb.nih.gov/ij/). B shows spontaneous action potentials recorded from current clamped AVNCs and sinoatrial nodal cells (SANCs) as well as an induced action potential from an atrial cell (AC), all of which are representative for these cell classes. The diastolic depolarization of both AVNCs and SANCs are clearly evident. C indicates the frequency of depolarization of the 3 cell types. Whereas ACs were stimulated at 0.5 Hz, both AVNC and SANC contracted spontaneously over the period of measurements at an average of ⬇17 and ⬇73 bpm, respectively. The diastolic depolarization rates (DDR) are indicated and varied in a manner consistent with the spontaneous depolarization rates. Note that the DDR value for ACs was not determined (N.D.), as diastolic depolarization is not observed in these cells. D shows the mean diastolic potential (MDP), action potential (AP) overshoot, amplitude, and duration (as both time for 50% [AP50] and 75% [AP75] repolarization). These values were not corrected for differences in cycle length. Statistical analysis of AP parameters demonstrate significant increases in the length (AP50 and AP75) in the atrial versus both types of pacemakers cells in the neonate heart (*P⬍0.050). Statistical Analysis Unless otherwise stated, data are presented as means with 95% confidence intervals (95% CI), and n represents cell number. Statistical significance of the results was tested using a 1-way or 2-way ANOVA and a Tukey test was used for post hoc multiple comparisons between groups with significant differences based on ANOVA. Student t test for paired samples as indicated or 2 test for categorical frequency data were used. A probability value of ⬍0.050 was considered significant. Results Histology and Immunohistochemistry of the Neonate AV Node Landmarks demarking the adult AV node are also identifiable in the neonate heart. The coronary sinus, tendon of Todaro, and tricuspid valve, which outline the triangle of Koch, can be clearly observed in Figure 1A. Representative results of Masson’s trichrome staining are shown in Figure 1B, 1C, and 1D, corresponding to serial sections S125, S165, and S302, as indicated in Figure 1A. Protein expression within the AV node was investigated with immunohistological techniques. Neurofilament 160 (NF160) is widely accepted as a unique cardiac pacemaker marker in rabbits.19,20 Serial sections neighboring the S125, S165, and S302 trichrome sections were labeled with NF160 and NCX and are shown as Figure 2A, 2B, and 2C, respectively. Immunolabeling for NF160 demonstrates high expression levels in the INE (Figure 2A and 2C-I), CN (Figure 2B and 2D-I) and HB (Figure 2C, 2E-I) conductive tissues. Whereas NF160 expression was extremely low in atrial tissue, NCX expression was high, providing a clear outline of the myocardium as well as a counter stain for the conductive tissues (Figure 2A through 2C). Connexin isoform expression is a key determinant of the electric conductivity between cells. Connexin 43 (Cx43) is the general cardiac isoform which forms high conductance gap-junctions. However in mature nodal cells, Cx43 is not expressed and connexin 45 (Cx45) is the predominant isoform, forming relatively low conductance gap-junctions. Thus, Cx43 expression is associated with low resistance, fast conducting pathways and Cx45 expression is associated with high resistance, slowly conducting pathways. Cx43 was found in abundance in atrial and ventricular muscle as well as within the bundle of His (Figure 2F-II), all areas associated with rapid conduction speeds. Cx43 in the atrial and ventricular myocardium was expressed as highly organized clusters at the intercalated disks. Cx43 expression was only rarely found associated with the INE (Figure 2D-II) and CN (Figure 2E-II) 2 areas associated with slow conduction speeds. Previous studies have suggested that HCN4 is the predominant hyperpolarization activated current (If) expressing channel in adult AVNCs.3,7,19 We used a monoclonal anti-HCN4 antibody on these sections and found that HCN4 labeling was abundant in the INE (Figure 2D-III), the CN (Figure 2E-III), and the HB (Figure 2F-III) and rarely seen in working myocardium. A schematic representation, combining the trichrome staining and immunohistological results, is presented in Figure 3. Sheng et al 50 mV -120 mV 2s 10d AVNC 50 pA 1s 10d AC AV Nodal Cells in Neonate Heart 941 containing 1.8 mmol/L calcium, 10% of cells began beating spontaneously. These spontaneously beating cells had mostly spindle-shaped morphologies and sustained their spontaneous rhythms for several hours at room temperature at 15– 60 beats per minute. Isolated AVNCs are identifiable by their absence of strong striations and 2 common cellular morphologies were identified: rod-shaped and spindle-shaped. Rod-shaped cells maintained a uniform cell width along the cell body, whereas spindle-shaped cells had significant tapering at the cell ends. Isolated atrial cells (ACs) contained obvious striations and are generally rod-shaped. Some spindle-shaped ACs with clear striations were also occasionally observed. General cellular dimensions and membrane capacitance of both neonate AVNCs (both spindle and rod-shaped) and ACs are shown in Figure 4A. Spontaneously Occurring Action Potentials in Pacemaking Cells Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 50 pA 1s 10d SANC 50 pA 1s Figure 5. Input resistance of atrioventricular nodal cells (AVNCs), sinoatrial nodal cells (SANCs), and atrial cells (ACs). The applied voltage protocol is shown. Representative current traces from ACs but not AVNCs or SANCs exhibited a large inward rectifier current. In these drawings, the atria and ventricle are outlined in red and mustard and the tricuspid value, central fibrous bundle, aorta, and aortic valve are highlighted in dark blue, fuchsia, and cyan, respectively. The nodal track, areas expressing NF160, is demarked in green. In sections S105 and S126, the nodal track lies on the atrial side of the central fibrous body (CFB), consistent with the INE propagating toward the penetrating bundle. The penetrating bundle, where the nodal track passes through the CFB, appears in S140 –S276. The nodal track emerges from the CFB as the HB, located in S302–S352. The intensities of protein labeling for different areas of the heart are presented Table 1. As expected, NF160 was only expressed within conductive tissues, whereas NCX was widely expressed. However, NCX intensity in the INE, CN, and HB was consistently higher than that found in the musculature. Atrial and ventricular cardiomyocytes were found to express Cx43 strongly with lesser intensities found in the HB. Neither the INE nor CN was found to express Cx43; however, these areas were found to express HCN4. Characterization of Single Isolated AVNC and SANC in the Neonate Heart When cells isolated from the AV nodal region were switched from a storage solution to a physiological Tyrode solution Action potentials were recorded from both spindled- and rod-shaped spontaneously beating AVNCs. Both types of cells appear to share the same general action potential profile, containing a pronounced diastolic depolarization during phase 0 (Figure 4B). The neonatal AVNC action potential quantitatively resembled the atrionodal (AN⫺) type action potential recorded on adult rabbit AVNCs, in terms of maximum diastolic potential (MDP), action potential (AP) overshoot, AP amplitude, and AP duration at 50% (APD50) repolarization.21 The previously reported nodal (N⫺) type and nodal-His (NH⫺) type action potentials were not observed in these neonate cardiac preparations. Action potentials were also recorded from neonatal ACs by electric stimulation (10 ms, 2⫻ threshold, 0.5 Hz). This induced action potential configuration was typical of the working myocardium, with a more hyperpolarized MDP and significantly longer APD50 and APD75 (P⬍0.050), as seen in the representative traces shown in Figure 4B. Temporal and voltage aspects of all three action potentials profiles are summarized in Figure 4C and 4D. Input Resistance Input resistance, measured from the linear component of the current recording, was used to quantify the susceptibility of a cell to changes in membrane voltage. Cells with high input resistance have low background conductance and only require small current injections to induce a change in membrane voltage. A 10-second voltage ramp from ⫺120 mV to ⫹50 mV was applied and representative currents are shown in Figure 5. A linear current was observed in AVNCs, suggesting a small inward rectifier current (IK1). This linear current had a reversal potential of ⫺53.8 mV (⫺58.7 to ⫺48.9 mV) (n⫽19), substantially more positive than the predicted potassium equilibrium potential (EK⫹), indicating a relatively low potassium conductance. In ACs, a strong inwardly rectified current was consistently recorded as a large inward current at strongly hyperpolarized potentials. Current recordings in ACs had a reversal potential of ⫺77.7 mV (⫺85.0 to ⫺70.4 mV) (n⫽9), almost equal to EK⫹, indicating a large dominating potassium conductance under diastolic conditions. 942 A Circ Arrhythm Electrophysiol December 2011 B 10d AVNC 5 mV -50 mV -40 mV -150 mV 100 pA 500 ms mV -150 -130 -110 -90 -70 -50 * * ** ** 200 pA 10d SANC 10d AVNCs (n=8) 10d ACs (n=9) Figure 6. Hyperpolarization-activated currents (If) of neonate atrioventricular nodal cells (AVNCs), sinoatrial nodal cells (SANCs), and atrial cells (ACs). A, Representative If traces for AVNCs, ACs, and SANCs, from top to bottom, as the result of the applied voltage protocol (B). C, Averaged instantaneous currents from AVNCs and ACs (*P⬍0.050; **P⬍0.010). D, Averaged If density, measured from the difference between the steadystate and instantaneous currents, for AVNCs, ACs, and SANCs. The number of cells is indicated below each bar in the bar graph (**P⬍0.010). D Peak difference current at -150 mV (pA/pF) Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 ** 500 ms 10 0 -10 -20 -30 -40 -50 -60 -70 Initial current (pA/pF) C 10d AC 0 10d AVNCs 10d SANCs 10d ACs 8 ** -2 11 -4 -6 100 pA 500 ms AVNCs had ⬇7-fold higher input resistance than ACs (AVNCs: 759.9 M⍀ (636.4 – 883.4 M⍀), n⫽19 versus ACs: 103.4 M⍀ (86.0 –120.8 M⍀), n⫽9; P⬍0.010), indicating a more readily modified membrane potential in AVNCs. The high input resistance associated with pacemaker-type cells allows small inward currents, from the presence of If and or a strong inward NCX current, to effectively depolarize these cells. Hyperpolarization-Activated Current If If is activated by hyperpolarization and can be assessed by inducing hyperpolarized membrane potentials. Figure 6A indicates the induced current in neonate AVNCs, ACs, and SANCs as the result of 2-second voltage-clamps stepped from ⫺150 mV to ⫺50 mV at 20 mV intervals, as shown on Figure 6B. If is measured from the difference between the instantaneous current evoked at the beginning of the voltage step and the steady-state current found at the end of the voltage step (Figure 6A). The current-voltage relationships for this instantaneous current component in ACs were clearly associated with large inward currents at these hyperpolarized potentials, stabilizing the resting membrane potential (Figure 6C). If was seen in 55% (11 of 21 cells) of AVNCs and 100% of SANCs (11 cells) with spontaneously action potential activity. If density in SANCs was more than twice that of AVNCs, and no functional expression of If in any of the ACs (9 cells) was found (Figure 6D). 11 Immunocytochemistry of AVNCs, SANCs, and ACs From the Neonate Heart The higher prevalence of If in SANCs with respect to AVNCs correlated with HCN4 expression intensities observed in single cells (Figure 7A through 7D). The distribution of HCN4 was predominately on the sarcolemma in both neonate AVNCs (Figure 7A) and SANCs (Figure 7B). In NF160positive cells, 87.6% of cells isolated from the SA node were found to also contain HCN4 (Figure 7C). In neonatal cells isolated from the AV node, only 58.8% of cells expressing NF160 were also found to express HCN4 (Figure 7C). No significant colocalization between HCN4 and NCX was observed in either SANCs or AVNCs, as in Figure 7D. Figure 7E shows NF160 (red) has a striated appearance in the intracellular compartment that corresponds to the sarcomere pattern of the AVNC sarcomere structures from the xz, xy, and yz planes. There was very little colocalization of NF160 observed with NCX (green). The distribution patterns of NF160, RyR and NCX are shown in neonate AVNC (Figure 8A-I), SANC (Figure 8A-II), and AC (Figure 8A-III). All 3 cell types demonstrated clear RyR striations with ⬇2 m periodicity but only AVNCs and SANCs were NF160 positive. NCX expression in all 3 cell types was limited to the cell periphery indicating the absence of significant t-tubular formation. The NCX to RyR colocalization was significantly higher in neonatal AVNCs Sheng et al AV Nodal Cells in Neonate Heart 943 Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 Figure 7. Dual NF160 and HCN4 labeling in neonate atrioventricular nodal cells (AVNCs) and sinoatrial nodal cells (SANCs). A and B are representative images of single cells with NF160 and HCN4 labeling, in AVNCs and SANCs, respectively. C is a 2⫻2 contingency table that presents the percentage of cells containing NF160 labeling that also contain HCN4 labeling for AVNCs and SANCs. The difference in HCN4 expression levels between AVNCs and SANCs was highly significant (P⬍0.0001). D presents subcellular colocalization data for AVNCs and SANCs expressing HCN4 and NCX. HCN4-with-NCX colocalization refers to how often HCN4 pixels are found to also contain NCX and vice versa. There was no significant difference between AVNCs and SANCs HCN4 and NCX colocalization values. E shows the 3D expression of NF160 (red) and NCX (green) in a neonate AVNC. I, II, and III represent the xz, xy, and yz planes, respectively, from a 3D confocal Z-stack. 944 Circ Arrhythm Electrophysiol December 2011 Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 Figure 8. NF160 triple labeling images of neonate atrioventricular nodal cells (AVNCs), sinoatrial nodal cells (SANCs). A presents representative deconvolved images for NF160, RyR and NCX triple labeling for AVNCs (A-I), SANCs (A-II), and atrial cells (ACs) (A-III) and the subsequent colocalization results (A-IV). B presents representative deconvolved images for NF160, SERCA, and PLB triple labeling for AVNCs (B-I), SANCs (B-II), and ACs (B-III) and the subsequent colocalization results (B-IV). NCX-with-RyR colocalization indicates how often a NCX pixel is found to also contain RyR. The NCX to RyR colocalization is significantly higher in AVNCs compared with ACs (P⫽0.041). Similar calculations were performed for the SERCA and PLB relationship. SERCA to PLB colocalization is significantly higher in AVNCs compared with SANCs (P⫽0.019). compared with ACs (Figure 8A-IV). Substantial levels of SERCA and PLB colocalization were found in all 3 cell types (Figure 8B-IV) and AVNCs contain significantly higher degrees of SERCA to PLB colocalization than do SANCs. Discussion AV Node and AVNC Morphology in Neonate Heart The examination of the histological and immunochemical sections in our study suggests the neonate heart shares similar AV anatomic complexity as the adult, consistent with the findings of other groups.4,19 INE, CN, and HB regions are clearly identifiable in 10-day AV nodal region. The HCN4 immunolabeling pattern in single cells was also reminiscent of what others have observed in adult SANCs.22,23 The HCN4 fluorescence intensity was found to be consistently higher in SANCs compared with that found in AVNCs with the majority of HCN4 staining distributed along the cell membrane. Occasionally, some cells had HCN4 localized intracellularly, which may be attributable to protein trafficking.19,24 Several different AVNC morphologies have been reported in adult hearts, including spider, spindle, rod, and ovoid phenotypes. Salient electrophysiological properties such as the action potential shape and ionic channel composition appear to vary with these different cellular morphologies.17,21,25 Compared with the adult, neonatal AVNCs were observed to be relatively homogeneous in the phenotypic features, and only spindle and rod morphologies were found. Although spontaneous pacemaker activity was observed more frequently in spindled cells, both cell shapes had similar action potential configurations and, If, ICa, and INa current densities (data not shown). Future studies may determine the developmental relationship between the variety of AVNC morphologies present in the adult and the more limited spindle- and rod-shaped morphologies found in the neonate heart. In 10-day rabbit hearts, AVNCs and ACs have similar cellular dimensions and membrane capacitances (Table 2), yet these 2 cell types are vastly different at ⬇56 days of development (Munk et al21,26). Combining our observations with those of Munk et al, ACs can be expected to grow ⬇1.7-fold in length and ⬇1.5-fold in width during this development period, with a ⬇2.6-fold increase in membrane capacitance. We have previously observed a ⬇3.5-fold change in membrane capacitance in rabbit ventricular myocytes over the same time frame,27 indicating that both atrial and ventricular myocytes undergo significant changes in cell morphology over this development period. However, over the same period, AVNCs were shown to undergo negligible changes in cell length and increased their cellular volume and membrane capacitance by only 1.3- and 1.5-fold, respectively. Therefore, in morphological terms, AVNCs appear to Sheng et al Table 2. AV Nodal Cells in Neonate Heart 945 Comparison of Neonatal (10-Day) Versus Mature (⬃56-Day) AVNCs and ACs: Cell Dimensions AVNCs (Rod-Shaped) 10-Day ACs 56-Day* 10-Day 56-Day* Mean 95% CI Mean 95% CI % Inc Mean 95% CI Mean 95% CI Length, m 64.5 54.9 –74.1 76.2 69.0 – 83.5 118.1 70.3 58.3– 82.3 121.8 102.2–141.4 173.3 Width, m 7.6 7.0–8.2 10.7 9.9–11.5 140.8 8.2 7.6–8.8 12.6 10.6–14.6 153.7 16.0–37.6 40.7 28.7–52.7 151.9 19.1 16.6–21.7 50.4 35.1–65.7 263.9 Cm, pF 26.8 Cells, n 6 8 9 % Inc 5 AVNCs indicates atrioventricular nodal cells; ACs, atrial cells; CI, confidence interval; and Inc, increase. *Data taken from Munk et al.21 In that study, the adult rabbits weighed 1.5–2.5 kg, which we have calculated to be approximately 8 weeks of age.26 Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 be nearly fully developed even at 10 days of age. The voltage aspects of the action potential from both 10-day and 56-day AVNCs are similar (Table 3). The functional consequences of this observation and the electric properties of these cells at different development stages remain to be determined. Electrophysiological Properties of Neonate AVNCs When compared with AVNCs, SANCs (NF160⫹) exhibit significantly higher expression of HCN4 and larger If, all consistent with their role as the dominant pacemaker in the heart. In the adult rabbit heart, the AV nodal rhythm is thought to originate from the INE, an area defined by a specific pattern of protein expression (NF160⫹, Cx43⫹/⫺, HCN4⫹, CaV1.3⫹), where a AN-type action potential predominates.4,19 Thus, HCN4 expression correlates to regions of strong pacemaker activity. In the adult heart, AVNCs appear to be electrically diverse with multiple action potential phenotypes having been reported.16,17,21,25,28 Among these reports, Billette28 subdivided the nodal cells into 6 groups, namely AN, ANCO, ANL, N, NH, and H cells, according to their action potential morphology and responses to periodic premature stimulation. Similar action potential diversity has also been found in the intact neonatal AV node, where Hewett et al recorded 4 action potential configurations designated as AN, N, high NH, and low NH.29 In our hands, only spindle- and rod-shaped AVNC morphologies could be identified and the action potentials recorded from these cells were uniformly of the AN-type. Table 3. Comparison of Neonatal (10-Day) Versus Mature (⬃56-Day) AVNCs and ACs: Action Potential Characteristics AVNCs (Rod-Shaped) 10-Day 56-Day* Mean 95% CI Mean 95% CI MDP, ⫺mV 68.8 71.4 – 66.3 71.9 77.4 – 65.4 Overshoot, mV 22.0 12.4–31.6 13.9 9.6–18.2 Amplitude, mV 90.8 82.2–99.4 85.8 81.5–90.1 APD50, ms 44.3 36.7–51.9 70.7 35.2–106.2 Cells, n 8 5 AVNCs indicates atrioventricular nodal cells; ACs, atrial cells; CI, confidence interval; MDP, mean diastolic potential; and APD, action potential duration. *Data taken from Munk et al.21 In that study, the adult rabbits weighed 1.5–2.5 kg, which we have calculated to be approximately 8 weeks of age.26 Neither the N- nor the NH-type action potentials, associated with compact nodal and nodal-his cell in the adult, were observed in our preparation. Immunolabeling results found both the anatomic INE and the anatomic CN to contain similar protein expression patterns (NF160⫹, Cx43⫹/⫺, HCN4 ⫹). However, it is not known whether the single cell recordings represent just the immature INE or other areas of the nodal track. Because of the diminutive size of the neonate nodal preparation, it is unclear whether the AN-type uniformity stems from an immature nodal action potential phenotype common among all nodal cells or from the relative prevalence of AN-type nodal cells in this preparation. We observed the diameter of CN in neonatal rabbit to be approximately 0.25 times of the adult compact node, and it is possible that non–AN-type cells are present but not observed due to their limited number. As the excision area predominantly isolated the AV node and only included a limited extension of the His Bundle, it is also conceivable that this cell type may be limited within the isolated cells. Nevertheless, HCN4 staining and the lack of Cx43 expression in both the INE and compact node could suggest that both regions may contain active pacemaker activity in the neonate heart. Further studies will be required to determine the functional contribution of HCN4 expression in the compact node. Although many AVNCs (NF160⫹) exhibited HCN4 and/or If expression, not all AVNCs contain these pacemaker hallmarks. All AVNCs were, however, found to contain the major components of the Ca2⫹ clock pacemaker mechanism (eg, RyR, NCX, SERCA, and PLB). Whether the prevalence or role of the calcium clock mechanism are the same as in the adult heart remains to be determined. In summary, neonatal AV nodal tissue shows similar histological complexity as the adult AV node. Although further structural and functional studies using optical mapping and computer reconstruction techniques need to be performed to delineate the neonatal AV nodal conduction pathways, this study represents the first characterization of isolated neonate AV cells. These findings should make a significant contribution to our understanding of AV nodal function in the neonate heart and the pathologies therein that are unique to that stage of ontogeny. Acknowledgments We thank Toro Min for contributions to the study. 946 Circ Arrhythm Electrophysiol December 2011 Sources of Funding These studies were generously supported by an operating grant from the Canadian Institutes of Health Research (to Dr Tibbits) and a junior research fellowship from the Heart and Stroke Foundation of Canada (to Dr Qu). Dr Tibbits is the recipient of Tier I Canada Research Chair. Disclosures None. References Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 1. Koch. Weiter mitteilungen uber den sinusknoten der herzens. Verh Dtsch Pathol Ges. 1909;13:85–92. 2. Efimov IR, Mazgalev TN. High-resolution, three-dimensional fluorescent imaging reveals multilayer conduction pattern in the atrioventricular node. Circulation. 1998;98:54 –57. 3. Efimov IR, Nikolski VP, Rothenberg F, Greener ID, Li J, Dobrzynski H, Boyett M. Structure-function relationship in the AV junction. Anat Rec A Discov Mol Cell Evol Biol. 2004;280:952–965. 4. Li J, Greener ID, Inada S, Nikolski VP, Yamamoto M, Hancox JC, Zhang H, Billeter R, Efimov IR, Dobrzynski H, Boyett MR. Computer threedimensional reconstruction of the atrioventricular node. Circ Res. 2008; 102:975–985. 5. Gaskell WH. On the innervation of the heart, with especial reference to the heart of the tortoise. J Physiol. 1883;4:43–127. 6. Hoffman BF, De Carvalho AP, De Mello WC. Transmembrane potentials of single fibres of the atrio-ventricular node. Nature. 1958;181:66 – 67. 7. Greener ID, Tellez JO, Dobrzynski H, Yamamoto M, Graham GM, Billeter R, Boyett MR. Ion channel transcript expression at the rabbit atrioventricular conduction axis. Circ Arrhythm Electrophysiol. 2009;2: 305–315. 8. Yoo S, Dobrzynski H, Fedorov VV, Xu SZ, Yamanushi TT, Jones SA, Yamamoto M, Nikolski VP, Efimov IR, Boyett MR. Localization of Na⫹ channel isoforms at the atrioventricular junction and atrioventricular node in the rat. Circulation. 2006;114:1360 –1371. 9. Hancox JC, Levi AJ. L-type calcium current in rod- and spindle-shaped myocytes isolated from rabbit atrioventricular node. Am J Physiol. 1994; 267:H1670 –H1680. 10. Guyton AC, Hall JE. Textbook of Medical Physiology. Philadelphia, PA: Elsevier Inc; 2006. 11. Lakatta EG, DiFrancesco D. What keeps us ticking: a funny current, a calcium clock, or both? J Mol Cell Cardiol. 2009;47:157–170. 12. Stefanelli CB, Fischbach PS. Cardiac arrhythmias in children. ACC Curr J Rev. 2003;12:103–107. 13. Lee PC, Chen SA, Chiang CE, Tai CT, Yu WC, Hwang B. Clinical and electrophysiological characteristics in children with atrioventricular nodal reentrant tachycardia. Pediatr Cardiol. 2003;24:6 –9. 14. Mildh L, Hiippala A, Rautiainen P, Pettila V, Sairanen H, Happonen JM. Junctional ectopic tachycardia after surgery for congenital heart disease: incidence, risk factors and outcome. Eur J Cardiothorac Surg. 2010;39: 75– 80. 15. De Carvalho AP, De Almeida DF. Spread of activity through the atrioventricular node. Circ Res. 1960;8:801– 809. 16. Anderson RH, Janse MJ, van Capelle FJ, Billette J, Becker AE, Durrer D. A combined morphological and electrophysiological study of the atrioventricular node of the rabbit heart. Circ Res. 1974;35:909 –922. 17. Hancox JC, Levi AJ, Lee CO, Heap P. A method for isolating rabbit atrioventricular node myocytes which retain normal morphology and function. Am J Physiol. 1993;265:H755–H766. 18. Huang J, Hove-Madsen L, Tibbits GF. Na⫹/Ca2⫹ exchange activity in neonatal rabbit ventricular myocytes. Am J Physiol Cell Physiol. 2005; 288:C195–C203. 19. Dobrzynski H, Nikolski VP, Sambelashvili AT, Greener ID, Yamamoto M, Boyett MR, Efimov IR. Site of origin and molecular substrate of atrioventricular junctional rhythm in the rabbit heart. Circ Res. 2003;93: 1102–1110. 20. Rothenberg F, Nikolski VP, Watanabe M, Efimov IR. Electrophysiology and anatomy of embryonic rabbit hearts before and after septation. Am J Physiol Heart Circ Physiol. 2005;288:H344 –H351. 21. Munk AA, Adjemian RA, Zhao J, Ogbaghebriel A, Shrier A. Electrophysiological properties of morphologically distinct cells isolated from the rabbit atrioventricular node. J Physiol. 1996;493(Pt 3):801– 818. 22. Barbuti A, Terragni B, Brioschi C, DiFrancesco D. Localization of f-channels to caveolae mediates specific beta2-adrenergic receptor modulation of rate in sinoatrial myocytes. J Mol Cell Cardiol. 2007;42:71–78. 23. Brioschi C, Micheloni S, Tellez JO, Pisoni G, Longhi R, Moroni P, Billeter R, Barbuti A, Dobrzynski H, Boyett MR, DiFrancesco D, Baruscotti M. Distribution of the pacemaker HCN4 channel mRNA and protein in the rabbit sinoatrial node. J Mol Cell Cardiol. 2009;47: 221–227. 24. Barbuti A, Gravante B, Riolfo M, Milanesi R, Terragni B, DiFrancesco D. Localization of pacemaker channels in lipid rafts regulates channel kinetics. Circ Res. 2004;94:1325–1331. 25. Meijler FL, Strackee J. Evolution and scaling of atrioventricular conduction time in mammals: part 1. Am Heart Hosp J. 2006;4:53–57. 26. Rao DR, Sunki GR, Johnson WM, Chen CP. Postnatal growth of New Zealand white rabbit (oryctolagus cuniculus). J Anim Sci. 1977;44: 1021–1025. 27. Huang J, Xu L, Thomas M, Whitaker K, Hove-Madsen L, Tibbits GF. L-type Ca2⫹ channel function and expression in neonatal rabbit ventricular myocytes. Am J Physiol Heart Circ Physiol. 2006;290: H2267–H2276. 28. Billette J. Atrioventricular nodal activation during periodic premature stimulation of the atrium. Am J Physiol. 1987;252:H163–H177. 29. Hewett KW, Gaymes CH, Noh CI, Ross BA, Thompson RP, Buckles DS, Gillette PC. Cellular electrophysiology of neonatal and adult rabbit atrioventricular node. Am J Physiol. 1991;260:H1674 –H1684. CLINICAL PERSPECTIVE The atrioventricular (AV) node represents the sole conduction pathway between the atrial and ventricular compartments of the normal adult heart. Many properties of the adult AV node have been elucidated, including anatomy, molecular architecture, and electric activity. However, the properties of the neonatal AV node and its role in unique pediatric cardiac arrhythmias such as junctional ectopic tachycardia (JET) are poorly understood. For the first time, histological and immunochemical examination of sections suggests the neonate heart shares similar AV anatomic complexity as the adult. Compared with the adult, single neonatal AV nodal cells were observed to be relatively mature in size and homogeneous in phenotypic features, as only spindle and rod morphologies were found. Spontaneous action potentials recorded from isolated neonatal AV nodal cells were uniformly of the atrionodal-type, showing none of the action potential heterogeneities found in the mature heart. Our report lays the groundwork for a better understanding of heart rate regulation and future studies aiming to find mechanisms of unique arrhythmias in the neonate heart such as JET. Isolation and Characterization of Atrioventricular Nodal Cells From Neonate Rabbit Heart Xiao Ye Sheng, Yang Qu, Pauline Dan, Eric Lin, Linda Korthout, Aaron Bradford, Leif Hove-Madsen, Shubhayan Sanatani and Glen F. Tibbits Downloaded from http://circep.ahajournals.org/ by guest on May 13, 2017 Circ Arrhythm Electrophysiol. 2011;4:936-946; originally published online October 14, 2011; doi: 10.1161/CIRCEP.111.964056 Circulation: Arrhythmia and Electrophysiology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2011 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-3149. Online ISSN: 1941-3084 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circep.ahajournals.org/content/4/6/936 Data Supplement (unedited) at: http://circep.ahajournals.org/content/suppl/2011/10/14/CIRCEP.111.964056.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Arrhythmia and Electrophysiology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Arrhythmia and Electrophysiology is online at: http://circep.ahajournals.org//subscriptions/ Supplementary Materials Methods Heart Excision and Cannulation The experimental protocols used in this study were in accordance with the Canadian Council on Animal Care (CCAC) regulations. The Animal Care Committee of the University of British Columbia approved the use of animals for this study. Isolation procedures specific to AVNCs were adapted and modified from isolation protocols used in our laboratory 1 formulated for neonatal ventricular myocytes and AVNC isolation protocols published for adult hearts 2. 10 day old (10-d) New Zealand rabbits (150 to 240 g) of either sex were deeply anaesthetized by an intra-peritoneal injection of thiopental sodium (60 mg/kg body weight) and sodium heparin (102.1 mg/kg body weight). Upon the disappearance of pinch-toe response the heart was rapidly excised. The aorta was cannulated 1.5 mm above the coronary orifice on a Langendorff apparatus providing retrograde perfusion. A 15 gauge stainless needle was used as a cannula to tightly fit into the 10-d aorta. Successful isolations required this entire procedure, from puncturing the thoracic cavity to perfusion of the heart, to be completed in less than one minute. Histology and Immunohistochemistry A rectangular section of right atrial tissue (3 x 5.5 mm) including not only the triangle of Koch but also the aorta and the bundle of His (see Figure 1A) was excised immediately after Solution A perfusion. The preparation was imbedded in O.C.T Tissue-Tek (#4583, Sakura) and frozen in isopentane pre-cooled to -140°C in liquid N2 and then stored at -80°C. 10 µm serial cryosections were sliced perpendicularly to the long axis of tricuspid valve (Figure 1A). Sections were mounted onto poly-L-lysine coated glass slides, fixed with 4% paraformaldehyde for 10 minutes and blocked with glycine for 10 minutes Masson’s trichrome staining was conducted using the manufacturer’s prescribed protocol (#HT15, Sigma). After staining, sections were rinsed, dehydrated with alcohol and cleared in xylene followed by Histomount (#19479, Ted Pella) mounting. Histological images were acquired using an Olympus BX51 microscope with a 4x objective. Mosaic images were created from ten to fifteen individual images using Adobe Photoshop CS5.5 (Figure 1B-D). Supplementary Materials ‐ AV nodal cells in neonate heart Immunohistology was applied to the serial sections adjacent to the trichrome sections. Sections were permeabilized with 0.1% Triton X-100 for 10 minutes and then washed with PBS 2x for 10 minutes each. Sections were then incubated with a variety of primary antibodies including: chicken anti neurofilament 160 (NF160) IgY, mouse anti NF160 IgG1, mouse anti sodium/calcium exchanger (NCX) IgM, mouse anti connexin 43(Cx43) IgG1 and mouse anti HCN4 IgG1) overnight at 4°C. After being washed with PBS 3x 10 minutes, sections were incubated with the secondary antibodies (goat anti-chicken IgY conjugated to Alexa 488 and goat anti-mouse IgG1 conjugated to Alexa 488 or 555) for 1 hour at room temperature. Detailed antibody information and dilutions are provided in Table S1. After 3 additional washes with PBS, the sections were mounted in Antifade reagent (#S36936, Sigma) and coverslips sealed with nail polish. Fluorescence images were acquired using an Olympus BX61 microscope with a 10x objective. On average 100 individual fluorescence images (tiles) were stitched together (Image Pro, MediaCybernetics) to generate the mosaic images (Figure 2A-C). Enzymatic Perfusion Following cannulation, the heart was retrogradely perfused for 5 minutes with solution A containing (in mM: 130 NaCl, 4.5 KCl, 3.5 MgCl2, 0.75 CaCl2, 0.4 NaH2PO4, 5 HEPES, 50 taurine, 10 glucose, titrated to pH 7.25 with NaOH) to clear the blood in the coronary circulation (18 ml min-1); followed with calcium-free solution A for 5 minutes (10 ml min-1). The perfusate was then switched to an enzyme solution which contained collagenase (0.1 mg/ml, Yakult, Japan), protease (0.05 mg/ml, P5147, Sigma) and BSA (1 mg/ml, #10775835001, Roche) in solution A. The perfusion volume of enzyme solution was adjusted from 65 to 95 ml depending on rabbit weight. The flow rate was maintained at 3.6 ml min-1. Detailed perfusion rates and enzyme concentrations are provided in Table S2. Mechanical Dissociation After digestion, the heart was removed and the AV nodal area exposed in a dissecting dish filled with cold storage solution (in mM: 100 L-glutamate potassium, 30 KCl, 5 Na-pyruvate, 20 taurine, 5 creatine, 5 succinic acid, 2 Na2ATP, 5 β-OH butyrate, 20 glucose, 5 MgCl2, 1 EGTA, 10 HEPES, titrated to pH 7.4 with KOH). A ~2 x 4 mm section of tissue was excised around the AV node for mechanical dissociation. This tissue was then transferred to a separate dish containing cold storage solution and minced with a surgical blade. Dissociated cells were filtered through a nylon mesh Supplementary Materials ‐ AV nodal cells in neonate heart (105 µm) and centrifuged at 80 x g for 2.5 minutes. The cell pellet was re-suspended and allowed to rest in storage solution for 30 minutes at room temperature and then transferred to Ca2+-free Tyrode’s solution (in mM: 140 NaCl, 5.4 KCl, 1 MgCl2, 10 HEPES,10 glucose, titrated to pH 7.4 with NaOH). The cellular solution was then titrated to 1.8 mM [Ca2+] over 20 minutes. Single atrial cells (ACs) were isolated from areas adjacent to the excised area from the same heart. Isolation of sinoatrial nodal cells (SANCs) from 10-d rabbit heart SANCs were isolated from 10-d rabbit hearts using similar procedures as that for AVNCs. Fifty ml of enzyme solution containing collagenase (0.2 mg/ml), elastase (0.4 mg/ml, #2292, Worthington), and protease (0.1 mg/ml) were recirculated at 3.6 ml min-1 for around 30 minutes to digest the whole heart (see Table S1). The endocardial surface was exposed with a longitudinal incision in the free wall and a rectangular section of tissue (~2 x 3 mm) including the whole SA node, superior vena cava and inferior vena cava 3 was excised. Cells were dissociated and dispersed into the storage solution, then washed and resuspended in Tyrode’s solution. Determinants for the successful isolation of AVNCs in neonatal heart We have established a well-defined isolation protocol through which a consistent high-yield of single ventricular myocytes and AVNCs from the neonatal heart was achieved. For successful isolation of functional AVNCs there were several critical factors. While some of these are intuitive, the technical aspects of this process cannot be overstated. The first is the rapidity and precision of anesthesia administration, heart excision and aortic cannulation. We observed that cannulation at ~1.5 mm above the coronary orifice provided the most efficient perfusion in hearts of this size. The second is the enzyme concentration and perfusion rate. In contrast to other adult AV nodal isolation protocols 2 4, it was determined that a much lower enzyme concentration and perfusion rate had to be employed to ensure the timely adjustment of perfusion time in accordance with the digestion status. The third is to minimize the mechanical stress on the cells. These cardiomyocytes from the immature heart are extremely vulnerable and less tolerant to enzymatic and mechanical treatment. Normally we did not repeatedly pipette the finely chopped tissue through small pore pipette tips unless the digestion was not complete. Supplementary Materials ‐ AV nodal cells in neonate heart Electrophysiological Recordings Isolated single cells were allowed to settle on poly-L-lysine coated glass-bottomed dishes and the perforated whole-cell patch-clamp technique was used to record action potentials and ionic currents (MultiClamp 700A, Axon Instruments, Union City, CA). Individual cells were visualized on an inverted microscope equipped with a 63x oil immersion objective (Eclipse TE300 Nikon). Patch pipettes (3 to 4 M) were pulled from thin-walled glass capillaries (World Precision Instruments, Sarasota, FL) using a vertical puller (PP-830, Narashige, Japan) and liquid junction potentials were corrected by -10 mV. 1-2 G seals were formed under the voltage clamp configuration and only cells in which the access resistance dropped to less than 10 M within 10-20 minutes after seal formation were used. Recordings acquired using pClamp (version 8.2, Axon Instruments, Digidata, 1322A) at 20 kHz and filtered at 1 kHz. All experiments were conducted at room temperature (22C). The external Tyrode’s solution contained (in mM): 140 NaCl, 5.4 KCl, 1.8 CaCl2, 1 MgCl2, 10 HEPES, and 10 glucose, pH 7.4 adjusted with NaOH. Extracellular solution was superfused at 0.2 ml min-1. The internal pipette solution contained (in mM): 10 NaCl, 50 KCl, 80 KOH, 80 aspartic acid, 1 MgCl2, 10 HEPES, pH 7.2 adjusted with KOH. Amphotericin B (Sigma) which was solubilized in dimethyl sulfoxide (DMSO) was used in a final concentration of 250 g/ml in the patch pipette and the final DMSO concentration was 0.2%. Immunocytochemistry The excised enzyme-digested rectangular tissue was chopped in a tissue culture dish containing 2% paraformaldehyde for 10 minutes. Cells were quenched by 100 mM glycine for 10 minutes, permeabilized with 0.1% Triton X-100 for 10 minutes, washed with PBS 2x for 10 minutes each, then allowed to settle onto poly-L-lysine (#P5899, Sigma) coated coverslips for one hour at room temperature. Cells were labeled with primary and secondary antibodies (see Table S2) following the same protocols as for immunohistochemistry. Single cell images were acquired on a Zeiss LSM 5 Pascal laser scanning confocal microscope equipped with Zeiss 63x/1.4 Plan-Apochromat oil immersion objective. Images were deconvolved to maximize available resolution5 using a maximum likelihood estimation (MLE) algorithm (Huygens Pro 2.4.1, Scientific Volume imaging, Supplementary Materials ‐ AV nodal cells in neonate heart Hilversum, Netherlands) in conjunction with an empirically determined point spread function6. Colocalization analyses were then conducted to determine the frequency of colocalization events. Supplementary Materials ‐ AV nodal cells in neonate heart Table S1. Primary (1o) and secondary (2o) antibodies used for immunohistochemistry and immunocytochemistry Antibodies Vendor Catalog # Dilution Mouse anti NF160 IgG1 DSHB 2H3 Supernatant Chicken anti-NF160 IgY SCT 1452 1:1000 Mouse anti-NCX IgM TS MA3-926 1:3000 Mouse anti-HCN4 IgG1 NM 75-150 1:10 Mouse anti-Cx43 IgG1 MP MAB3068 1:500 Mouse anti-RyR IgG1 TS MA3-916 1:200 Mouse anti-SERCA IgG1 TS MA3-910 1:3000 Mouse anti-PLB IgG2a TS MA3-922 1:200 Goat anti-mouse IgG1 IV A-21121 1:500 o 1 Ab 2o Ab congugated to Alexa Fluor 488 or 555 AffiniPure Goat Anti-chicken IgY A-21127 JIR 103-485-155 1:3000 IV A-21426 1:500 conjugated to DyLight 488 Goat anti-mouse IgM conjugated to Alexa Fluor 555 DSHB - Developmental Studies Hybridoma Bank; SCT - StemCell Technologies; TS - Thermo Scientific NM - Neuromab; MP - Millipore; IV - Invitrogen; JIR - Jackson ImmunoResearch Supplementary Materials ‐ AV nodal cells in neonate heart Table S2. Parameters for single cell isolation 10d AVNCs 10d SANCs 10d ACs Solution A Perfusion rate (ml/min) 18 18 18 Enzyme solution perfusion rate (ml/min) 3.6 3.6 3.6 Enzyme solution concentration (mg/ml) Collagenase 0.10 Collagenase 0.20 Collagenase 0.10 Protease 0.05 Protease 0.10 Protease 0.05 Elastase 0.00 Elastase 0.40 Elastase 0.00 BSA 1.00 BSA 1.00 BSA 1.00 Enzyme solution volume (ml) 65-95 50 65-95 Enzyme solution recirculation? no yes no Supplementary Materials ‐ AV nodal cells in neonate heart Table S3. Action Potential Parameters – Range of Observations 10d AVNC MDP (mV) Overshoot (mV) Amplitude (mV) APD50 (ms) APD75 (ms) min -70 -1 69 33 80 max -60 40 105 66 230 MDP (mV) Overshoot (mV) Amplitude (mV) APD50 (ms) APD75 (ms) min -95 -4 85 29 58 max -60 50 110 141 192 MDP (mV) Overshoot (mV) Amplitude (mV) APD50 (ms) APD75 (ms) min -100 -7 87 72 141.7 max -65 30 105 213 354 10d SANC 10d AC Figure S1 - Measurement of diastolic depolarization rate (DDR). Figure S2 - AP50 and AP75 Figure S1. The measurement of DDR was performed by determining the maximum diastolic potential (MDP) as indicated in the above diagram with the arrow labeled 1 and connecting it to the threshold as indicated in the above diagram with the arrow labeled as 2. Figure S2. Measurement of Action Potential Duration (AP50 and AP75). The AP amplitude was determined as the difference between the MDP and the point of maximum overshoot. The times required to repolarize to 50% (AP50) and 75% (AP75) of this value were then calculated. Supplementary Materials ‐ AV nodal cells in neonate heart Figure S3. S3A S3B S3C Figure S3. Figures S3A, S3B, and S3C are the original images of Figures 2A, 2B, and 2C, respectively. Images shown in the text were slightly modified with Adobe Photoshop CS5.5 to remove artifactual staining of debris on slides (Figures S3A-C) and of the aorta (Ao) (top right of Figure S3C). Using a 40x objective, the staining of the debris was found to be extracellular in origin thereby constituting non-specific staining. Likewise, staining of the aorta was found to be extracellular and appears to constitute the well-established “edge effect” 7 thereby constituting non-specific staining. Movie S1. A rotating 3D AVNC cell dual-labeled with NF160 and NCX clearly indicating that NF160 (red) shows a striated appearance in the intracellular compartment that corresponds to the sarcomere pattern of the AVNC sarcomere structures and very little co-localization was observed with NCX (black). Supplementary Materials ‐ AV nodal cells in neonate heart References for Supplementary Material 1. 2. 3. 4. 5. 6. 7. Huang J, Hove-Madsen L, Tibbits GF. Na+/Ca2+ exchange activity in neonatal rabbit ventricular myocytes. Am J Physiol Cell Physiol. 2005;288:C195-203 Hancox JC, Levi AJ, Lee CO, Heap P. A method for isolating rabbit atrioventricular node myocytes which retain normal morphology and function. Am J Physiol. 1993;265:H755-766 Boyett MR, Honjo H, Yamamoto M, Nikmaram MR, Niwa R, Kodama I. Downward gradient in action potential duration along conduction path in and around the sinoatrial node. Am J Physiol. 1999;276:H686-698 Munk AA, Adjemian RA, Zhao J, Ogbaghebriel A, Shrier A. Electrophysiological properties of morphologically distinct cells isolated from the rabbit atrioventricular node. J Physiol. 1996;493 :801-818 Sedarat F, Lin E, Moore ED, Tibbits GF. Deconvolution of confocal images of dihydropyridine and ryanodine receptors in developing cardiomyocytes. J Appl Physiol. 2004;97:1098-1103 Dan P, Lin E, Huang J, Biln P, Tibbits GF. Three-dimensional distribution of cardiac Na+/Ca2+ exchanger and ryanodine receptor during development. Biophys J. 2007;93:25042518 True LD. Quality control in molecular immunohistochemistry. Histochem Cell Biol. 2008;130:473-480