Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
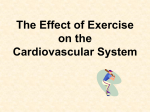
566 MEDICINA (2002) Vol. 38, No. 5 - http://medicina.kmu.lt Long-term risk of stroke after a first-ever myocardial infarction Daiva Rastenytė, Diana Šopagienė, Ričardas Radišauskas Institute of Cardiology, Kaunas University of Medicine, Lithuania Key words: stroke, myocardial infarction, risk, cumulative risk. Summary. Purpose. To examine the incidence of stroke during the first three years after a first-ever myocardial infarction. Material and methods. Both Kaunas community-based ischemic heart disease register and stroke register were used as the primary source of data. The methods used for data collection were those applied by the WHO for the international MONICA project. During 1986 to 1996, 4201 persons aged 25 to 61 years with a first-ever myocardial infarction were included into Kaunas community-based ischemic heart disease register and followedup for three years against first-ever stroke or death from any cause. Actuarial life tables were used to analyze risk of stroke. Results. During the study period, 82 (2.0%) patients with the first-ever stroke that occurred among survivors of myocardial infarction were identified: 68 (82.9%) men and 14 (17.1%) women. The cumulative risk of stroke was 3.19% (95% CI 2.50 to 3.88%) by 3 years: among male myocardial infarction survivors this risk was accounted for 3.37% (95% CI 2.54 to 4.17%) and that among female – for 2.51% (95% CI 1.22 to 3.80%). The risk was identified as the highest one early after ictus among the myocardial infarction survivors: 0.43% (95% CI 0.21-0.65%) by 3 months (men – 0.51% (95% CI 0.24 to 0.78%), women – 0.12% (95% CI 0 to 0.38%)) and 0.23% (95% CI 0.05 to 0.41%) by 6 months (men – 0.25% (95% CI 0.03 to 0.47%), women – 0.18% (95% CI 0 to 0.53%)). Conclusion. The risk of stroke is identified as the highest one early after the myocardial infarction. Introduction Heart diseases - acute myocardial infarction (AMI), disorders of heart rhythm and conduction, endocarditis, heart tumors, diseases of heart valves, etc., are not the last ones among the main modifiable risk factors of stroke such as arterial hypertension, smoking, cholesterol, impaired glucose tolerance, diabetes mellitus (DM) (1-3). Stroke is an important complication of the AMI, occurring in 1% to 3% of all AMI patients and in 2% to 6% of the patients with anterior wall infarctions (4). Majority of strokes after AMI is thought to be embolic, arising from left ventricular wall mural thrombi, but a number may be atherothrombotic or, in the acute phase, secondary to hemodynamic compromise. Most strokes occur in the first week after the infarction, but some risk for stroke remains for an indefinite time (4). Although morbidity and mortality of major cardiovascular diseases – AMI and stroke are high in comparison with the other European and world countries, there are only very few studies on relationship be- tween these two diseases in Lithuania. Therefore, the aim of the present study was to evaluate the risk of stroke during the first three years after an index myocardial infarction on the basis of the ischemic heart disease and stroke registers’ data. Material and methods Both Kaunas community-based ischemic heart disease register, which is underway since 1983, and the community-based stroke register, which is underway since 1986, and are covering the entire population of Kaunas city aged 25-64 years, were used as the primary sources of data. The methods used for data collection were those applied by the WHO for the international MONICA (MONItoring of trends and determinants in CArdiovascular disease) project (5) and were described in detail elsewhere (6-9). The diagnosis of AMI and stroke was based on the criteria proposed by the WHO (5). Diagnostic criteria of AMI or coronary death were based on: 1) symptoms of a coronary event, 2) ECG findings, 3) serum cardiac enzymes, Correspondence to D.Šopagienė, Institute of Cardiology, Kaunas University of Medicine, Sukilėlių 17, 3007 Kaunas, Lithuania. E-mail: [email protected] Long-term risk of stroke after a first-ever myocardial infarction 4) necropsy findings (6-7). Allocation to the following epidemiological diagnostic categories was performed: 1 - define AMI; 2 – possible AMI or coronary death; 4 – no AMI or coronary death; 9 – fatal cases with insufficient data. Stroke was defined as rapidly developed clinical sings of focal or global disturbance of cerebral function lasting more than 24 hours (except in cases of sudden death or if the development of symptoms was interrupted by a surgical intervention) with no apparent cause other than a vascular origin (5, 10). According to the MONICA protocol, multiple AMI or stroke attacks occurring within 28 days from the onset of the symptoms of the first attack were considered as one event. The AMI or stroke event was defined fatal if the death occurred within the first 28 days from the onset of AMI or stroke. If the patient was alive after 28 days from the onset of the attack, the case was classified as non-fatal. All records on non-fatal AMI cases recorded among the persons aged 25-61 years and assigned to the diagnostic categories “1”, “2” or “9” were extracted from the IHD data-base. All residents of Kaunas city aged 25-64 years, who experienced their stroke during 1986 to 1999, were included into the stroke register database. Using the patient’ gender and date of birth as the identification code, and the computed search system, all new stroke cases that occurred among the AMI survivors during the first three years from the onset of AMI, were identified. Statistical analysis. Actuarial life tables (KaplanMeier method) were used to analyze risk of stroke (11). Log-Rank test was used to estimate reliability. Differences in rates at the p< 0.05 level were reported as statistically significant. Results During the 11-year study period (1986 through 1996), 4,201 persons aged 25-61 years experienced and survived their first-ever AMI: 3368 (80.2%) of them were men and 833 (19.8%) - women. During the first three years after the index AMI, 82 (2.0%) patients had a first-ever stroke: 68 (82.9%) of them were men and 14 (17.1%) - women. Of all patients, 71 (1.7%) (59 (83.1%) men and 12 (16.9%) women) had suffered an ischemic stroke. Frequency of stroke among AMI survivors during the 3-year follow-up is presented in Table 1. The highest frequency of stroke was observed among men aged 45-54 years (2.3%) and among women aged 55-61 years (2.4%). Strokes were more prevalent among male AMI survivors aged 45-54 years than among MEDICINA (2002) Vol. 38, No. 5 - http://medicina.kmu.lt 567 females of the same age (2.3% and 0.4%, respectively, p = 0.04). Similar results were obtained looking at the frequency of ischemic stroke only. However, there were no statistically significant differences observed between men and women of no one of the age groups analyzed in respect of the following ischemic stroke. The risk of stroke during the 3 years form onset of AMI is presented in Table 2. Although due to relatively young age of our patients and rather few new stroke events among them statistical significance has not been reached, the highest absolute risk of stroke was during the first 3 months after ictus, 0.43%: 0.51% among men and 0.12% among women. Among male AMI survivors, the risk of stroke has decreased twice (to 0.25%) during the next 3 months (3 to 6 months time period) and remained rather stable during other 3-month time-periods (Table 2). Among female AMI survivors, risk of stroke has decreased a little bit during the second half of the first year compared to the first 3 months. Compared to the first year after the index AMI, risk of stroke had an increasing tendency (Table 2). The risk of stroke was slightly higher among women than among men during the third year after AMI (1.49% and 1.13%, respectively). Cumulative risk of stroke by 3 years among male AMI survivors was 1.3-fold higher compared to that among female AMI survivors (3.37% and 2.5%, respectively). The curves of cumulative stroke risk among male and female AMI survivors have not differed statistically significantly during the 3-year follow-up (Log-Rank = 1.22; p = 0.3) (Figure 1). Similar results were obtained analyzing the risk of ischemic stroke among AMI survivors during the first 3 years of the follow-up (Table 3). Discussion The main cause of ischemic heart disease is processes of atherosclerosis in the vessels wall. Because atherosclerosis is a generalized process that involves the heart, brain, and peripheral arteries, it is related with many other clinical manifestations and syndromes. A substantial proportion of AMI survivors are under the increased risk of stroke, which leads to a poor clinical prognosis. According to a number of clinical studies, during the first 2 weeks ischemic stroke occurs in 15% of AMI patients (12-18). According to the data reported by Kaarisalo M. et al., the risk of stroke was identified as the highest during the first 2 weeks after AMI and accounted for 0.7% (19). In our present study, the risk of stroke among AMI survivors aged 25-61 568 Daiva Rastenytė, Diana Šopagienė, Ričardas Radišauskas Table 1. Frequency of stroke among the survivors of acute myocardial infarction (AMI) during the 3-year follow-up Sex Age group, years AMI survivors free of stroke AMI survivors with of stroke Total ischemic stroke hemorrhagic stroke1 all strokes n (%) n (%) n (%) n (%) n (%) Men 25–44 45–54 55–61 25–61 506 (99.2) 1354 (97.7) 1440 (97.8) 3300 (98.0) 4 (0.8) 29 (2.1) 26 (1.8) 59 (1.7) 0 3 (0.2) 6 (0.4) 9 (0.3) 4 (0.8) 32 (2.3)* 32 (2.2) 68 (2.0) 510 (100) 1386 (100) 1472 (100) 3368 (100) Women 25–44 45–54 55–61 25–61 50 (98.0) 276 (99.6) 493 (97.6) 819 (98.3) 1 (2.0) 1 (0.4) 10 (2.0) 12 (1.5) 0 0 2 (0.4) 2 (0.2) 1 (2.0) 1 (0.4) 12 (2.4) 14 (1.7) 51 (100) 277 (100) 505 (100) 833 (100) Total 25–44 45–54 55–61 25–61 556 (99.1) 1630 (98.0) 1933 (97.8) 4119 (98.0) 5 (0.9) 30 (1.8) 36 (1.8) 71 (1.7) 0 3 (0.2) 8 (0.4) 11 (0.3) 5 (0.9) 33 (2.0) 44 (2.2) 82 (2.0) 561 (100) 1663 (100) 1977 (100) 4201 (100) – both intracerebral hemorrhage and subarachnoid hemorrhage included. *p=0.04 men compared with women. 1 Table 2. Risk of stroke in the survivors of acute myocardial infarction during 3-year follow-up Sex Period less than 3 months 3-6 months 6 - 12 months 12 - 24 months 24 - 36 months Men Absolute risk (%) 95 % CI1 Number of stroke patients Cumulative risk (%) 95 % CI 0.51 0.24–0.78 13 0.51 0.22–0.80 0.25 0.03–0.47 5 0.76 0.41–1.11 0.55 0.22–0.88 11 1.31 0.82–1.80 0.93 0.50–1.36 19 2.24 1.59–2.89 1.13 0.64–1.62 20 3.37 2.54–4.17 Women Absolute risk (%) 95 % CI Number of stroke patients Cumulative risk (%) 95 % CI 0.12 0–0.38 1 0.12 0–0.36 0.18 0–0.53 1 0.30 0–0.71 0.18 0–0.53 1 0.48 0–1.03 0.54 0–1.15 3 1.02 0.2–1.84 1.49 0.46–2.52 8 2.51 1.22–3.80 Total Absolute risk (%) 95 % CI Number of stroke patients Cumulative risk (%) 95 % CI 0.43 0.21–0.65 14 0.43 0.19–0.67 0.23 0.05–0.41 6 0.66 0.37–0.95 0.47 0.20–0.74 12 1.13 0.74–1.52 0.85 0.49–1.21 22 1.98 1.45–2.51 1.21 0.77–1.65 28 3.19 2.50–3.88 1 – 95% CI - 95% confidence interval. years was the highest one during the first 3 months after ictus (0.43%). As it is reported, after an initial AMI, strokes and congestive heart failure (CHF) occur at a rate that is 3 to 6-fold that of the general population (20). CHF developed in approximately 30% of patients who had experienced an AMI, which represents a 4 to 6-fold increase in risk. CHF and coronary heart disease may predispose patients to strokes by producing emboli or decreasing cardiac output and may predispose patients to occur stroke (20). MEDICINA (2002) Vol. 38, No. 5 - http://medicina.kmu.lt Long-term risk of stroke after a first-ever myocardial infarction 569 Table 3. Risk of ischemic stroke in the survivors of acute myocardial infarction during 3-year follow-up Sex Period less than 3 months 3-6 months 6 - 12 months 12 - 24 months 24 - 36 months Men Absolute risk (%) 95 % CI1 Number of stroke patients Cumulative risk (%) 95 % CI 0.33 0.11–0.55 8 0.33 0.09–0.57 0.25 0.03–0.47 5 0.58 0.27–0.89 0.50 0.19–0.81 10 1.08 0.63–1.53 0.94 0.51–1.37 18 2.02 1.41–2.63 0.97 0.52–1.42 18 2.99 2.23–3.75 Women Absolute risk (%) 95 % CI Number of stroke patients Cumulative risk (%) 95 % CI 0.12 0–0.38 1 0.12 0–0.36 0.18 0–0.53 1 0.30 0–0.71 0.18 0–0.53 1 0.48 0–1.03 0.54 0–1.15 3 1.02 0.2–1.84 1.12 0.22–2.02 6 2.14 0.94–3.34 Total Absolute risk (%) 95 % CI Number of stroke patients Cumulative risk (%) 95 % CI 0.29 0.11–0.47 9 0.29 0.09–0.49 0.23 0.05–0.41 6 0.52 0.25–0.79 0.43 0.18–0.68 11 0.95 0.58–1.32 0.85 0.49–1.21 21 1.80 1.29–2.31 1.00 0.6–1.4 24 2.80 2.15–3.45 1 – 95% CI - 95% confidence interval. Probability of stroke 0,04 Log-Rank=1,22; p=0,3 Men 0,03 Women 0,02 0,01 0 0 4 8 12 16 20 Months 24 28 32 36 Fig. 1. Cumulative risk of stroke among the acute myocardial infarction survivals aged 25-61 years during 3-year follow-up The frequency of stroke varies according to the age of AMI patients, the severity and location of AMI, and complications, and duration of the follow-up. In the prethrombolytic era, stroke was associated with a large anterior AMI and poor left ventricular function. MEDICINA (2002) Vol. 38, No. 5 - http://medicina.kmu.lt It was reported, that about 50% of all post-AMI strokes were associated with anterior AMI (17, 21), however, some other studies have not found any association between the occurrence of stroke and site of AMI (22-23). 570 Daiva Rastenytė, Diana Šopagienė, Ričardas Radišauskas There are only a few studies on the occurrence of stroke during a longer follow-up after MI attack. The annual incidence of stroke is reported between 0.7% and 3% in different studies (18, 21, 24-28). Cumulative risk of stroke during one year after an index AMI was 1.13% in our study, which is in accordance with previous findings; although it was almost twice lower than compared to Finnish study (2.2%) (19). It should be noted, however, that our study population was younger than Finnish one (25-61 yrs vs. 25-74 yrs.). Arterial fibrillation (AF) may also occur after AMI as an independent risk factor for post-MI stroke (16). Also cholesterol reduction with statins has been found to reduce stroke incidence after AMI (29). As far as we know, there are no previous studies on whether diabetes mellitus (DM) is a risk factor for post-MI stroke, although DM is an independent risk factor for thromboembolic stroke (30). Abnormalities of coagulation may also increase the risk of post-MI stroke (31). Thrombolysis is more and more often used for AMI treatment, although thrombolytic therapy is associated with an increased risk of intracranial hemorrhage that usually occurs within the first day of therapy. The rate of post-MI hemorrhagic strokes with thrombolysis is reported to be 0.3% to 1.1% (13-14, 32-34). The increased risk of hemorrhagic stroke is associated with advanced age, hypertension, previous stroke, head trauma, intracranial tumor, arteriovenous malformations and use of tissue plasminogen activator (14, 35). In our present study, the risk of hemorrhagic stroke was identified as the highest early after ictus among male AMI survivors, i.e., during the first 3 months. Despite the attention focused on the occurrence of hemorrhagic stroke in the context of thrombolytic therapy of AMI, nonhemorrhagic stroke remains a more frequent complication after AMI. There are only a few community-based studies on the frequency of ischemic strokes in the thrombolytic era (17, 34). The frequency of ischemic strokes during hospitalization has decreased with thrombolytic therapy. Thrombolytic agents administered soon after AMI might affect the development of left ventricular thrombus, since early laminar thrombus, invisible to the echocardiographer, could have dissolved (17, 34). Another possible explanation for the decreased frequency of ischemic strokes in AMI patients treated with thrombolysis is that thrombolytic therapy reduces the amount of myocardial damage and, consequently, left ventricular dysfunction develops less frequently (36). Conclusion Among AMI survivors aged 25-61 years the risk of stroke was identified as the highest one early after the AMI, i.e., during the first 3 months after ictus. Galvos smegenų insulto rizika persirgus ūminiu miokardo infarktu Daiva Rastenytė, Diana Šopagienė, Ričardas Radišauskas Kauno medicinos universiteto Kardiologijos institutas Raktažodžai: galvos smegenų insultas, miokardo infarktas, rizika, suminė rizika. Santrauka. Darbo tikslas – nustatyti galvos smegenų insulto riziką ligoniams, sirgusiems miokardo infarktu. Darbo apimtis ir metodai. Duomenų šaltiniai – Kauno išeminės širdies ligos bei galvos smegenų insulto registrai, kaupiantys informaciją apie visus miokardo infarkto bei galvos smegenų insulto atvejus. Analizuojamąją grupę sudarė 25–61 metų 4201 Kauno gyventojas, kurį 1986–1996 metais ištiko pirmasis miokardo infarktas. Kiekvienas asmuo, sirgęs miokardo infarktu, stebėtas trejus metus. Tyrimo galinis taškas buvo galvos smegenų insultas arba mirtis nuo bet kurios priežasties. Galvos smegenų insulto rizika bei suminė galvos smegenų insulto rizika apskaičiuota remiantis Kaplan-Meier’io išgyvenamumo lentelėmis. Rezultatai. Tarp 4201 stebėto asmens, sirgusio pirmuoju miokardo infarktu, per trejus metus nuo ligos pradžios užregistruoti 82 galvos smegenų insulto (visi klinikiniai tipai) atvejai. Trejų metų suminė galvos smegenų insulto rizika vyrams, sirgusiems miokardo infarktu, buvo 1,3 karto didesnė negu moterims (atitinkamai – 3,37 (95 proc. pasikliautinasis intervalas 2,54–4,17) ir 2,51 proc. (95 proc. pasikliautinasis intervalas 1,22–3,80)). Didžiausia galvos smegenų insulto rizika po miokardo infarkto buvo nustatyta per pirmuosius tris mėnesius ir siekė 0,43 proc. (95 proc. pasikliautinasis intervalas 0,21–0,65): vyrams ši rizika siekė 0,51 proc. (95 proc. pasikliautinasis intervalas 0,24–0,78), moterims – 0,12 proc. (95 proc. pasikliautinasis intervalas 0,0–0,38). Per MEDICINA (2002) Vol. 38, No. 5 - http://medicina.kmu.lt Long-term risk of stroke after a first-ever myocardial infarction 571 kitus 3 mėnesius (3–6 mėn. laikotarpis) vyrams, persirgusiems pirmuoju miokardo infarktu, galvos smegenų insulto rizika sumažėjo du kartus (atitinkamai nuo 0,51 (95 proc. pasikliautinasis intervalas 0,24–0,78) iki 0,25 proc. (95 proc. pasikliautinasis intervalas 0,03–0,47) ir vėliau ši rizika nekito. Moterims rizika susirgti galvos smegenų insultu pradėjo mažėti praėjus 6 mėnesiams nuo miokardo infarkto. Lyginant su pirmaisiais metais, antraisiais ir trečiaisiais metais galvos smegenų insulto rizika po miokardo infarkto moterims toliau didėjo. Trečiaisiais metais moterų rizika susirgti galvos smegenų insultu buvo kiek didesnė negu vyrų tuo pačiu laikotarpiu – atitinkamai 1,49 (95 proc. pasikliautinasis intervalas 0,46–2,52) ir 1,13 proc. (95 proc. pasikliautinasis intervalas 0,64–1,62). Išvada. Galvos smegenų insulto rizika buvo didžiausia ankstyvuoju poinfarktiniu laikotarpiu, nors statistiškai reikšmingų skirtumų dėl santykinai mažo atvejų skaičiaus nerasta. Adresas susirašinėjimui: D.Šopagienė, KMU Kardiologijos institutas, Sukilėlių 17, 3007 Kaunas References 1. Qizilbash N. Are risk factor for stroke and coronary disease the same? Curr Opin Lipidol 1998;9:325-8. 2. Sen S, Oppenheimer SM. Cardiac disorders and stroke. Curr Opin Lipidol 1998;11:51-6. 3. Petty GW, Khandheria BK, Whisnant JP, Sicks JoRean D, O’Fallon WM, Wiebers DO. Predictors of cerebrovascular events and death among patients with valvular heart disease. Stroke 2000;31:2628-35. 4. Mohr JP, Albers GW, Amarenco P, Babikian VL, Biller J, Brey RL, Coull B, Easton JD, Gomez CR, Helgason CM, Kase CS, Pullicino PM, Turpie AG. American Heart Association Prevention Conference. IV. Prevention and Rehabilitation of Stroke. Etiology of stroke. Stroke 1997;28:1501-6. 5. World Health Organization MONICA project. MONICA Manual. Geneva; 1990. 6. Rastenienė D, Rastenytė D, Adomavičienė I. Klinikinės ir epidemiologinės ūmaus miokardo infarkto diagnostikos būklė Kaune. (Clinical and epidemiological diagnosis of acute myocardial infarction Kaunas.) Medicina 1993;29:47-8. 7. Rastenienė D, Rastenytė D, Radišauskas R, Blužas J. Išeminės širdies ligos registras: 35-64 m. Kauno gyventojų sergamumo ir mirtingumo rodiklių pokyčiai 1971-1993 m. (Ischemic heart disease Register: morbidity and mortality trends in Kaunas inhabitants aged 35-64 years from 1971 to 1993.) Medicina 1995;31:88-91. 8. Rastenytė D. Kauno gyventojų mirtingumas nuo galvos smegenų insulto 1986-1993 metais: galvos smegenų insulto registro duomenys. (Stroke mortality trends in the Kaunas population during 1986-1993: Data from the Kaunas Stroke register.) Medicina 1995;31:6-10. 9. Rastenytė D. Sergamumas ir mirštamumas nuo galvos smegenų insulto 1986-1993 metais: Kauno galvos smegenų insulto registro duomenys. (Trends in incidence and case-fatality of stroke in Kaunas population during 1986-1993: Data from the Kaunas Stroke register.) Medicina 1995;31:536-40. 10. Asplund K, Tuomilehto J, Stegmayr B, Westwr PO, TunstallPedoe H. Diagnostic criteria and quality control of the registration of stroke events in the MONICA project. Acta Med Scand Supl 1988;728:26-39. 11. Norusis MJ. SPSS Advanced Statistics 6.1. Chicago; 1984. p.257-90. 12. Behar S, Tanne D, Abinader E, Agmon J, Barzilai J, Friedman Y, Kaplinsky E, Kauli N, Kishon Y, Palant A, et al. Cerebrovascular accident complicating acute myocardial infarction: incidence, clinical significance and short- and long-term mor- MEDICINA (2002) Vol. 38, No. 5 - http://medicina.kmu.lt 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. tality rates. The SPRINT Study Group. Am J Med 1991;91:45-50. Maggioni AP, Franzosi MG, Farina ML, Santoro E, Celani MG, Ricci S, Tognoni G. Cerebrovascular events after myocardial infarction: analysis of the GISSI trial. BMJ 1991;302: 1428-31. Maggioni AP, Franzosi MG, Santoro E, White H, Van de Werf F, Tognoni G. The risk of stroke in patients with acute myocardial infarction after thrombolytic and antithrombotic treatment. N Engl J Med 1992;327:1-6. Hess DC, D’Cruz IA, Adams RJ, Nichols FT. 3rd. Coronary artery disease, myocardial infarction, and brain embolism. Neurol Clin 1993;11:399-417. Komrad MS, Coffey CE, Coffey KS, McKinnis R, Massey EW, Califf RM. Myocardial infarction and stroke. Neurology 1984;34:1403-9. Mooe T, Eriksson P, Stegmayr B. Ischemic stroke after acute myocardial infarction. A population-based study. Stroke 1997;28:762-7. Mooe T, Olovson BO, Stegmayr B, Eriksson P. Ischemic stroke. Impact of a recent myocardial infarction. Stroke 1999;30:997-1001. Kaarisalo MM, Immonen-Räļhä PI, Marttila RJ, Salomaa V, Torppa J, Tuomilehto J. Stroke after myocardial infarction. CVD Prevention 1998;1:200-6. Kannel WB. Overview of atherosclerosis. Clinical therapeutics 1998;20:B2-5. Tanne D, Reicher-Reiss H, Boyko V, Behar S. for the the SPRINT Study Group. Stroke risk after anterior wall acute myocardial infarction. Am J Cardiol 1995;76:825-6. Asinger RW, Mikell FL, Elsperger J, Hodges M. Incidence of left-ventricular thrombosis after acute transmural myocardial infarction. Serial evaluation by two-dimensional echocardiography. N Engl J Med 1981;305:297-302. Nadareishvili ZG, Choudary Z, Joyner C, Brodie D, Norris JW. Cerebral microembolism in acute myocardial infarction. Stroke 1999;30:2679-82. Mooe T, Teien D, Karp K, Eriksson P. Left ventricular thrombosis after anterior myocardial infarction with and without thrombolytic treatment. J Intern Med 1995;237:563-9. Tanne D, Goldbourt U, Zion M, Reicher-Reiss H, Kaplinsky E, Behar S and the SPRINT Study Group. Frequency and prognosis of stroke/TIA among 4808 survivors of acute myocardial infarction. Stroke 1993;24:1490- 572 Daiva Rastenytė, Diana Šopagienė, Ričardas Radišauskas 5. 26. Bodenheimer MM, Saer D, Shareef B, Brown MW, Fleiss JL, Moss AJ. Relation between myocardial infarction location and stroke. J Am Coll Cardiol 1994;24:61-6. 27. Loh E, John Sutton M, Chuan-Chuan CW, Rouleau JL, Flaker GC, Gottlieb SS, Lamas GA, Moye LA, Goldhaber SZ, Pfeffer MA. Ventricular dysfunction and risk of stroke after myocardial infarction. N Engl J Med 1997;336:251-7. 28. Firstenberg MS, Thomas JD. Stroke-distance measurement after acute myocardial infarction. Lancet 2000;355:1240. 29. Plehn JF, Davis BR, Sacks FM, Rouleau JL, Pfeffer MA, Bernstein V, Cuddy E, Moyé LA, Piiler LB, Rutherford J, Simpson LM, Braunwald E. Reduction of stroke incidence after myocardial infarction with pravastatin. The cholesterol and recurrent events (CARE) study. Circulation 1999;99:21623. 30. Kuller LH, Velentgas P, Barzilay J, Beauchamp NJ, O’Leary DH, Savage PJ. Diabetes mellitus: subclinical cardiovascular disease and risk of incident cardiovascular disease and allcause mortality. Arterioscler Thromb Vasc Biol 2000;20:823- 9. 31. Koening W, Trust E. The possible role of hemorrhagia in atherothrombogenesis. Atherosclerosis 1992;94:93-107. 32. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. Lancet. 1988;2(8607):349-60. 33. ISIS-3 (Third International Study of Infarct Survival) Collaborative Group.A randomised comparison of streptokinase vs tissue plasminogen activator vs anistreplase and of aspirin plus heparin vs aspirin alone among 41,299 cases of suspected acute myocardial infarction. Lancet. 1992;339:753-70. 34. Longstreth WT Jr, Litwin PE, Weaver WD. Myocardial infarction, thrombolytic therapy, and stroke. A community-based study. The MITI Project Group Stroke 1993;24:587-90. 35. Vaitkus PT, Berlin JA, Schwartz JS, Barnathan ES. Stroke complicating acute myocardial infarction. A meta-analysis of risk modification by anticoagulation and thrombolytic therapy. Arch Intern Med 1992;152:2020-4. Received 15 February 2002, accepted 3 April 2002 MEDICINA (2002) Vol. 38, No. 5 - http://medicina.kmu.lt