Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
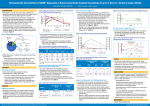
USED IN MORE THAN 1 MILLION PAT I E N T S SET A SMOOTH RECOVERY IN MOTION Reduce the need for opioids while providing long-lasting postsurgical pain control…all from a single dose Please refer to accompanying full Prescribing Information. 1 Opioid burden Postsurgical pain management: an important part of recovery Current treatment strategy leaves room for improvement Although as many as 99% of postsurgical patients receive an opioid 2 74 % of patients reported moderate to extreme pain after discharge3 57 % of patients preferred a nonopioid3 30 % of patients worried about becoming addicted3 Source: Postsurgical patient survey of patients who had undergone surgery in the past 5 years (N=300).3 Opioids: effective, yet pose concerns for patients and health care providers 2,4-6 •A dverse events increase risk of morbidity, delay ambulation, can increase length of stay, and may lead to hospital readmissions2,5 —O pioids are not recommended in several high-risk patient populations4 —O pioid-related issues can have a negative impact on patient satisfaction and reimbursement3,5,6 A high potential for misuse, dependency, or diversion creates a societal burden 7-9 • 1 in 15 patients prescribed opioids will go on to long-term use or abuse7,8 • In a study (N=250), the average patient consumed 1/3 of their opioid prescription, resulting in 4,639 leftover pills that could be diverted9 • In 2010, approximately 5 million people were classified as opioid abusers10 2 A multimodal strategy is recommended to reduce opioid reliance11-13 • American Society of Anesthesiologists (2012): Guideline Recommendations for Acute Pain Management “ ” Whenever possible, anesthesiologists should use multimodal pain management therapy. 11 • The Centers for Disease Control and Prevention and The Joint Commission support an opioid-reducing strategy12,13 should reflect a [patient]-centered approach and consider the patient’s current “Strategies presentation, the health care providers’ clinical judgment, and the risks and benefits associated with the strategies, including potential risk of dependency, addiction, and abuse. ” 12 The challenges of implementing an opioid-reducing strategy • T he short duration of most local anesthetics (≤8 hours) limits their effectiveness when postsurgical pain is at its worst 5,14 •S upplementation is often needed with catheters and pumps, which can15-20 — Limit mobility — Introduce risk of infection — Cause variable infusion rates and concentrations — Migrate or dislodge • T he average cost of catheter and pump maintenance, monitoring, and materials adds up to >$60020,21 3 DepoFoam® Cutting-edge technology sets EXPAREL apart With a unique drug delivery system, EXPAREL is designed to extend postsurgical analgesia • Indicated for single-dose administration into the surgical site to produce postsurgical analgesia •D epoFoam uniquely delivers bupivacaine over time to extend pharmacologic effect — Encapsulates bupivacaine via a multivesicular liposomal drug delivery technology22 — R eleases bupivacaine over time as lipid membranes reorganize22 Plasma levels of bupivacaine may persist for 96 hours23,* 300 Plasma bupivacaine concentration (ng/mL) Reliable release of a low dose of bupivacaine over time1 • L onger duration provides coverage when postsurgical pain 250 *Data from TKA study. 200 is at its worst 150 • E liminates the need for titration with a single dose 100 • E liminates the need for external devices to prolong analgesia • E XPAREL dosing is not weight based 50 — Different formulations of bupivacaine are not bioequivalent 0 even if the milligram dosage is the same; therefore, it is not 24 48 0 possible to convert dosing from any other formulation of Time (h) bupivacaine to EXPAREL and vice versa •O ther formulations of bupivacaine should not be administered within 96 hours following administration of EXPAREL 4 EXPAREL 266 mg 72 96 Pharmacokinetics Low systemic exposure to bupivacaine EXPAREL Cmax values fell below adverse event thresholds in clinical trials EXPAREL Cmax (ng/mL) 4,500 Cardiac threshold 4,000 Cmax (ng/mL) 3,500 3,000 2,500 CNS threshold 2,000 1,500 1,000 500 0 Bony model (Bunionectomy; 106 mg) n=26 Soft-tissue model (Hemorrhoidectomy; 266 mg) n=25 • T he blood plasma level where CNS effects are typically seen with traditional bupivacaine: >2,000 ng/mL • T he blood plasma level where cardiac effects are typically seen with traditional bupivacaine: >4,000 ng/mL • T he rate of systemic absorption of bupivacaine is dependent on the total dose, the route of administration, and the vascularity of the administration site Please refer to accompanying full Prescribing Information. 5 Set a smooth recovery in motion with EXPAREL EXPAREL: significant long-lasting pain control that reduces the need for opioids 1,5 Cumulative reductions in pain and opioid use through 72 hours1,5 0 Percentage reduction compared with placebo N=189 10 20 30% 30 40 50 Reduction in cumulative pain scores P<0.0001 45% Reduction in opioid consumption P=0.0006 •S ignificant reductions in pain intensity up to 24 hours (P<0.0001) with a 45% decrease in opioid consumption through 72 hours; the clinical benefit of the decrease in opioid consumption was not demonstrated1 6 Studies demonstrating the safety and efficacy of EXPAREL were conducted in hemorrhoidectomy and bunionectomy. Set a smooth recovery in motion with EXPAREL Significantly longer time to first opioid rescue 5 Median time to first opioid use5 EXPAREL Placebo N=189 P<0.0001 14.3 hours 1.2 hours 0 2 4 6 8 10 12 14 16 Time (h) • 2 8% of patients were opioid free at 72 hours with EXPAREL vs 10% with placebo (P<0.0008)5 Soft-tissue (hemorrhoidectomy) trial design1,5 •P hase 3 trial of patients undergoing a 2- or 3-column excisional hemorrhoidectomy (N=189) randomized to receive single administration of 266 mg of EXPAREL or placebo for postsurgical analgesia •P rimary endpoint was cumulative pain scores as reflected in the AUC of NRS through 72 hours •P lacebo was preservative-free saline for injection •O pioid rescue medication (up to 10 mg IM morphine) was available to all patients Please refer to accompanying full Prescribing Information. 7 Set a smooth recovery in motion with EXPAREL Assessing the full value of EXPAREL: pain reduction + opioid reduction Significantly lower AUC NRS scores vs placebo1,24 AUC NRS scores 6 5 EXPAREL Placebo P<0.0001 N=189 P<0.0001 4 P<0.0001 3 P=0.0007 P=0.0388 2 P=0.1361 P=0.5371 24 36 P=0.5289 P=0.9094 P=0.8383 48 60 72 1 0 1 2 4 8 12 Time (h) • 0 -24 hours: EXPAREL demonstrated significant reductions in pain intensity scores vs placebo24 Significantly less cumulative opioid consumption vs placebo1,24 Opioid consumption (mg) 20 16 EXPAREL Placebo N=189 P<0.0001 12 P=0.0003 48 60 P=0.0006 P<0.0001 P<0.0001 8 4 0 12 24 36 Time (h) 8 P<0.0001 72 contrast to looking at pain “Inscores alone, the use of multiple outcome measures [including the use of postsurgical opioid rescue medication] may provide a more meaningful assessment of the therapeutic effects of an analgesic medication in a clinical study setting. 24 ” —Schmidt Set a smooth recovery in motion with EXPAREL EXPAREL: meeting the need for lasting efficacy while reducing opioid reliance 0-24 hours: EXPAREL demonstrated a significant reduction in pain intensity scores •D ifferences in scores diminished over time due to use of rescue medication24 • In the placebo group, median time to first rescue medication was 1.2 hours; use of rescue medication led to equalization in pain control beginning at 24 hours1,24 — Rescue medication (up to 10 mg IM morphine) was available every 4 hours as needed over the first 72 hours — By 24 hours postsurgery, 88% of placebo patients had used opioid rescue medication Cumulative difference in opioid consumption was maintained through 72 hours •R eduction in cumulative pain intensity scores was maintained with less cumulative opioid use through 72 hours24 Please refer to accompanying full Prescribing Information. 9 Set a smooth recovery in motion with EXPAREL EXPAREL: tolerability and safety profile similar to placebo 1 In clinical trials •S afety evaluated in 21 clinical trials (1,307 patients received EXPAREL)1 — 1 0 wound infiltration trials: 823 patients —N umerous procedures; EXPAREL doses ranged from 66 mg to 532 mg •W ell tolerated; most common adverse events (incidence ≥10%) were nausea, constipation, and vomiting • E XPAREL demonstrated a favorable cardiac safety profile25,26 —N o detectable cardiac toxicity signal —N o QTc prolongation, even at supratherapeutic doses In clinical practice • L ow incidences of adverse events (0.04%) reported in postmarketing integrated safety analysis following 600,000 exposures1 More than 1 million patients have received EXPAREL since 2012 1 10 Set a smooth recovery in motion with EXPAREL A single dose of EXPAREL delivers long-lasting pain control1 •D ose EXPAREL based on the administration site and the volume required to cover the area — C an be administered undiluted or expanded up to a total volume of 300 mL with normal (0.9%) saline for injection or lactated Ringer’s solution to accommodate the size of the surgical site •A vailable as 266 mg, 1.3%/20 mL single-use vials •M aximum dose of EXPAREL should not exceed 266 mg (one 20 mL vial) •N o dosage adjustment needed for mild to moderate hepatic impairment, renal impairment, or elderly patients Important Safety Information Monitoring of cardiovascular and neurological status, as well as vital signs should be performed during and after injection of EXPAREL as with other local anesthetic products. Because amide-type local anesthetics, such as bupivacaine, are metabolized by the liver, EXPAREL should be used cautiously in patients with hepatic disease. Patients with severe hepatic disease, because of their inability to metabolize local anesthetics normally, are at a greater risk of developing toxic plasma concentrations. Please refer to accompanying full Prescribing Information. 11 Set a smooth recovery in motion with EXPAREL EXPAREL administration • Inject EXPAREL slowly into soft tissues of the surgical site with frequent aspiration to check for blood and minimize the risk of intravascular injection Epidermis 1 2 3 4 Dermis Nociceptors Subcutaneous tissue Fascia Muscle Administration precautions •W ait 20 minutes after administering other non-bupivacaine-based local anesthetics before administering EXPAREL into the same surgical site •A llow topical antiseptics to dry before administering EXPAREL into the same surgical site •W hen using bupivacaine HCl before EXPAREL, the dose of bupivacaine HCl should be ≤50% the dose of EXPAREL. As a reference: — One 20 mL vial of EXPAREL contains 266 mg of free base bupivacaine; 266 mg of free base bupivacaine is equivalent to 300 mg of bupivacaine HCl — One 30 mL vial of 0.5% bupivacaine HCl contains 150 mg bupivacaine HCl — Toxic effects of these drugs are additive and their administration should be used with caution, including monitoring for neurological and cardiovascular effects •D o not admix EXPAREL with other drugs prior to administration 12 Set a smooth recovery in motion with EXPAREL EXPAREL stays more precisely where placed, requiring more injections to cover the same area Technique and distribution are important when administering into the surgical site • Inject EXPAREL slowly into the soft tissue of the surgical site Bupivacaine EXPAREL using a deep-tissue infiltration technique —Administer EXPAREL with a 25-gauge or larger needle • E XPAREL is best administered using a series of injections to effectively cover the surgical area since it does not diffuse throughout tissues in the same manner as traditional bupivacaine Note: Graphic is for illustrative purposes only. Please refer to accompanying full Prescribing Information. 13 Important Safety Information EXPAREL is contraindicated in obstetrical paracervical block anesthesia. EXPAREL has not been studied for use in patients younger than 18 years of age. Non-bupivacaine-based local anesthetics, including lidocaine, may cause an immediate release of bupivacaine from EXPAREL if administered together locally. The administration of EXPAREL may follow the administration of lidocaine after a delay of 20 minutes or more. Other formulations of bupivacaine should not be administered within 96 hours following administration of EXPAREL. Monitoring of cardiovascular and neurological status, as well as vital signs should be performed during and after injection of EXPAREL as with other local anesthetic products. Because amide-type local anesthetics, such as bupivacaine, are metabolized by the liver, EXPAREL should be used cautiously in patients with hepatic disease. Patients with severe hepatic disease, because of their inability to metabolize local anesthetics normally, are at a greater risk of developing toxic plasma concentrations. In clinical trials, the most common adverse reactions (incidence ≥10%) following EXPAREL administration were nausea, constipation, and vomiting. Please refer to accompanying full Prescribing Information. 14 Blank Inside Of Pocket Blank Inside Of Pocket References: 1. Data on file. Parsippany, NJ: Pacira Pharmaceuticals, Inc.; February 2015. 2. Kessler ER, Shah M, Gruschkus SK, Raju A. Cost and quality implications of opioid-based postsurgical pain control using administrative claims data from a large health system: opioid-related adverse events and their impact on clinical and economic outcomes. Pharmacotherapy. 2013;33(4):383-391. 3. Gan TJ, Habib AS, Miller TE, White W. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin. Published online: November 15, 2013. Accessed March 4, 2015. 4. The Joint Commission. Safe use of opioids in hospitals. Sentinel Event Alert; August 8, 2012; Issue 49. 5. Gorfine SR, Onel E, Patou G, Krivokapic Z. Bupivacaine extendedrelease liposome injection for prolonged postsurgical analgesia in patients undergoing hemorrhoidectomy: a multicenter, randomized, double-blind, placebo-controlled trial. Dis Colon Rectum. 2011;54(12):1552-1559. 6. Survey of patients’ experiences. Medicare.gov website. http://www.medicare.gov/HospitalCompare/Data/PatientSurvey/Overview.aspx. Accessed January 5, 2015. 7. Alam A, Gomes T, Zheng H, Mamdani MM, Juurlink DN, Bell CM. Long-term analgesic use after low-risk surgery: a retrospective cohort study. Arch Intern Med. 2012;172(5):425-430. 8. Carroll I, Barelka P, Wang CK, Wang BM, et al. A pilot cohort study of the determinants of longitudinal opioid use after surgery. Anesth Analg. 2012;115(3):694-702. 9. Rodgers J, Cunningham K, Fitzgerald K, Finnerty E. Opioid consumption following outpatient upper extremity surgery. J Hand Surg Am. 2012;37(4):645-650. 10. Popping pills: prescription drug abuse in America. National Institute on Drug Abuse website. http://www.drugabuse.gov/related-topics/trends-statistics/infographics/popping-pills-prescription-drug-abuse-in-america. Accessed March 4, 2015. 11. American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2004;100(6):1573-1581. 12. The Joint Commission. Clarification of the Pain Management Standard PC.01.02.07. Joint Commission Perspectives. 2014;34(11):11. http://www.jointcommission.org/assets/1/18/Clarification_of_the_Pain_Management__Standard.pdf. Accessed March 4, 2015. 13. Centers for Disease Control and Prevention. Common elements in guidelines for prescribing opioids for chronic pain. http://www.cdc.gov/drugoverdose/prescribing/common-elements.html. Updated April 1, 2015. Accessed June 12, 2015. 14. Golf M, Daniels SE, Onel E. A phase 3, randomized, placebo-controlled trial of DepoFoam® bupivacaine (extended-release bupivacaine local analgesic) in bunionectomy. Adv Ther. 2011;28(9):776-788. 15. Ilfeld BM, Loland VJ, Sandhu NS, Suresh PJ, Bishop MJ, Donohue MC. Continuous femoral nerve blocks: the impact of catheter tip location relative to the femoral nerve (anterior versus posterior) on quadriceps weakness and cutaneous sensory block. Anesth Analg. 2012;115(3):721-727. 16. Kinder R, Hsiung R. Overview of peripheral nerve blocks. In: Chu LF, Fuller A, eds. Manual of Clinical Anesthesiology. Philadelphia, PA: Lippincott Williams & Wilkins; 2011. https://www.inkling.com/read/manual-clinical-anesthesiology-chu-fuller-1st/chapter-34/overview-of-peripheral-nerve. Accessed October 7, 2014. 17. Process for handling elastomeric pain relief balls (ON-Q PainBuster and others) requires safety improvements. Institute for Safe Medication Practices website. https://www.ismp.org/newsletters/acutecare/ articles/20090716.asp. Accessed June 3, 2015. 18. I-Flow ON-Q pump with ONDEMAND bolus button. US Food and Drug Administration website. http://www.fda.gov/MedicalDevices/Safety/ ListofRecalls/ucm317826.htm. Accessed January 5, 2015. 19. Continuous peripheral nerve blocks in outpatients. NYSORA–The New York School of Regional Anesthesia website. http://www.nysora.com/ regional-anesthesia/foundations-of-ra/3055-continuous-peripheral-nerve-blocks-in-outpatients.html. Accessed January 5, 2015. 20. Frost & Sullivan. New opportunities for hospitals to improve economic efficiency and patient outcomes: the case of EXPAREL™, a long-acting, non-opioid local analgesic. http://www.frost.com/prod/servlet/cpo/252218999. Accessed January 5, 2015. 21. White PF, Kehlet H, Neal JM, Schricker T, Carr DB, Carli F; Fast-Track Surgery Study Group. The role of the anesthesiologist in fast-track surgery: from multimodal analgesia to perioperative medical care. Anesth Analg. 2007;104(6):1380-1396. 22. How DepoFoam® works. Pacira Pharmaceuticals, Inc. website. http://www.pacira.com/depofoam-platform/how-it-works.php. Accessed January 8, 2015. 23. Bramlett K, Onel E, Viscusi ER, Jones K. A randomized, double-blind, dose-ranging study comparing wound infiltration of DepoFoam bupivacaine, an extended-release liposomal bupivacaine, to bupivacaine HCl for postsurgical analgesia in total knee arthroplasty. Knee. 2012;19(5):530-536. 24. Schmidt WK, Patou G, Joshi GP. Evaluating therapeutic benefit in postsurgical analgesia requires global assessment: an example from liposome bupivacaine in hemorrhoidectomy. Hosp Pract (1995). 2012;40(1):160-165. 25. Bergese SD, Onel E, Morren M, Morganroth J. Bupivacaine extended-release liposome injection exhibits a favorable cardiac safety profile. Reg Anesth Pain Med. 2012;37(2):145-151. 26. Naseem A, Harada T, Wang D, et al. Bupivacaine extended release liposome injection does not prolong QTc interval in a thorough QT/QTc study in healthy volunteers. J Clin Pharmacol. 2012;52(9):1441-1447. 15 In the management of postsurgical pain A smooth start to recovery begins with EXPAREL Reduce the need for opioids while providing long-lasting postsurgical pain control… all from a single dose • Indicated for single-dose administration into the surgical site to produce postsurgical analgesia •D epoFoam® drug delivery system slowly delivers bupivacaine over time to extend the pharmacologic effect of EXPAREL22 •S ignificantly reduces opioid consumption1,5 • E liminates the need for catheters and pumps that may hinder recovery 2,5,15-20 • Safety and tolerability profile similar to placebo1 Used in more than 1 million patients Please refer to accompanying full Prescribing Information. For complete information related to EXPAREL, call 1-855-RX-EXPAREL (793-9727) or visit www.EXPAREL.com. ©2015 Pacira Pharmaceuticals, Inc. Parsippany, NJ 07054 PP-EX-US-0665 06/15 since 2012 1