Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Review
Dose-Adjusting Capecitabine Minimizes Adverse
Effects While Maintaining Efficacy: A
Retrospective Review of Capecitabine for
Metastatic Breast Cancer
Robert Leonard,1 Bryan T. Hennessy,2 Joanne L. Blum,3 Joyce O’Shaughnessy3
Abstract
Capecitabine monotherapy is considered standard treatment in anthracycline- and taxane-pretreated metastatic
breast cancer and has proven efficacy in this setting. Randomized studies and retrospective analyses have shown
that, in patients who received capecitabine monotherapy, or in combination with docetaxel, dose modification of
capecitabine is effective in the management of adverse events without compromising efficacy. Dose adjustment of
capecitabine is easy to implement due to its twice-daily oral administration. This article reports the findings of a
retrospective review of a large data set to consolidate the information about the impact of capecitabine dose
modification on efficacy and safety outcomes in patients with metastatic breast cancer. Data on dose modification
and outcomes were available from 4 phase II capecitabine monotherapy trials, 1 phase III capecitabine/docetaxel
combination trial, and an analysis of consecutive patients who received capecitabine outside of a clinical trial (n !
971). Dose reductions were required in 41% of patients who received monotherapy (n ! 131) and 65% of patients
who received capecitabine/docetaxel (80% of these required dose reductions of both agents) (n ! 163). Time to
disease progression and overall survival were similar, or even slightly longer, among patients who received lower vs.
full-dose capecitabine in all of the studies reviewed. Reduced capecitabine doses were associated with a lower
incidence of treatment-related adverse events, specifically hand-foot syndrome, diarrhea, and stomatitis. Together,
these data support the practice of dose-reducing capecitabine, including the possibility of starting at a lower dose
("1250 mg/m2 twice daily), to reduce the incidence of adverse events without compromising efficacy.
Clinical Breast Cancer, Vol. 11, No. 6, 349-56 © 2011 Published by Elsevier Inc.
Keywords: Advanced breast cancer, Docetaxel, Dose modification, Safety
Introduction
The effectiveness of numerous cytotoxic agents has been evaluated in patients with anthracycline- and/or taxane-pretreated
metastatic breast cancer (MBC), both as monotherapy and in
various combination regimens. Capecitabine (Xeloda), one of the
1
Division of Cancer and Surgery, Imperial College Healthcare NHS Trust, London, UK
Department of Gynecological Medical Oncology, MD Anderson Cancer Center,
Houston, TX
3
Department of Oncology, Baylor-Sammons Cancer Center, Texas Oncology, US
Oncology, Dallas, TX
2
Submitted: Feb 03, 2011; Revised: Jun 15, 2011; Accepted: Jun 19, 2011
Address for correspondence: Robert Leonard, MD, Cancer Services, Imperial College
Healthcare NHS Trust, 3rd Fl N, Charing Cross Hospital, Fulham Palace Road,
London, W6 8RF, UK
Tel: #44 208 846 7237; fax: #44 208 846 7454; e-mail contact: Robert.
[email protected]
1526-8209/$ - see frontmatter © 2011 Published by Elsevier Inc.
doi: 10.1016/j.clbc.2011.06.005
most extensively appraised agents, is regarded as standard treatment in this patient group, having demonstrated consistent efficacy and safety as monotherapy in several large, multicenter clinical trials.1,2 The coadministration of capecitabine and docetaxel in a
randomized phase III trial by O’Shaughnessy et al3 was the first combination regimen to demonstrate a significant survival advantage over a
single agent (14.5 vs. 11.5 months, hazard ratio [HR] 0.775; P ! .0126)
in patients with anthracycline-pretreated MBC, as well as being associated with a manageable safety profile. A retrospective analysis of the
impact of poststudy therapy on survival in this trial revealed that the
median overall survival (OS) was most improved in patients initially
randomized to docetaxel who then received poststudy capecitabine
(21.0 vs. 12.3 months, HR 0.50; P ! .0046), compared with any other
poststudy chemotherapy.4
In the MBC setting, capecitabine is approved as monotherapy,
and in combination with docetaxel, at a starting dose of 1250 mg/m2
Clinical Breast Cancer December 2011
349
Capecitabine Dose Modification
Table 1 Phase II Studies of Capecitabine Monotherapy in MBC
Patients Who
Received
Capecitabine, n
Capecitabine
Dose, mg/m2
Prior
Chemotherapy
for MBC
ORR, %
Median TTP,
mo
Median OS,
mo
Blum 1999 (SO14697)18
162
1255a
A and paclitaxel
20 (n ! 32)
8.1
12.8
Blum 2001 (NO15542)13,17
74
1255a
A and paclitaxel/
docetaxel
26 (n ! 19)
3.2
12.2
O’Shaughnessy 2001
(SO14799)16
61
1255a
None
30 (n ! 18)
4.1
19.6
Talbot 2002 (SO15179)19
22
1255a
A
36 (n ! 8)
3.0
7.6
a
Tx
15 (n ! 20)
3.5
10.1
Study
45
Reichardt 2003
136
1250
Fumoleau
200446/Largillier 200647
126
1250a
A and Tx
28 (n ! 35)
–
15.2
Kusama 201040
50
825b
A
28 (n ! 14)
5.3
20.2
33
b
None
18 (n ! 6)
6.9
24.8
41
Taguchi 2010
825
Abbreviations: A ! anthracyclines; MBC ! metastatic breast cancer; ORR ! overall response rate; OS ! overall survival; TTP ! time to progression; Tx ! taxane.
a
All capecitabine doses are twice daily over 14 days on a 3 weekly treatment cycle.
b
All capecitabine doses are twice daily over 14 days continuous.
twice daily (b.i.d.) for 14 days, orally followed by a 7-day drug-free
period, every 3 weeks. In the United States, FDA approval of the
combination regimen was granted in 2001, with the monotherapy
approval dating back to 1998. In the decade that has since elapsed,
physicians have gained substantial experience of using capecitabine,
both at the registered dose and at a reduced dose, as a successful
means of managing common treatment-related adverse events,
such as hand-foot syndrome (HFS), diarrhea, and nausea and/or
vomiting. The twice-daily oral administration of capecitabine, a
more convenient and preferred route than intravenous drug delivery for many patients,5-7 creates several opportunities for dose
adjustment and thereby allows immediate treatment adaptation.
Indeed, many phase II-III clinical trials of capecitabine use a
predefined dose-modification scheme for the onset of NCICCTC (National Cancer Institute of Canada Common Toxicity
Criteria) grade 2 and above adverse events that are likely to become life threatening.3 Dose interruption or reduction of capecitabine at the first appearance of an adverse event permits prompt
resolution of the event, and prevents its recurrence,8,9 which enables patients to continue therapy longer and thereby potentially
gain maximum clinical benefit. In addition to considering tolerability, each individual’s capecitabine dose also should be tailored
according to patient and disease characteristics, when taking into
account factors such as race, age, sex, and concomitant medications,10 because these can greatly affect the metabolism of the
drug.
A number of randomized studies11,12 and retrospective analyses9,13-15 have shown that, in patients who receive capecitabine
monotherapy, or capecitabine in combination with docetaxel, dose
modification of capecitabine minimizes the incidence and severity of
adverse events without compromising efficacy. This article reports
the findings of a retrospective review of a large data set to reinforce
available information on the effect of dose modification on the efficacy and safety of capecitabine in patients with MBC. It also addresses the use of a lower initial oral dose of capecitabine ("1250
350
Clinical Breast Cancer December 2011
mg/m2) to reduce the incidence of treatment-related adverse events
while maintaining efficacy.
Patients and Methods
Several phase II trials of capecitabine monotherapy have been
conducted in patients with MBC, in both the first-line and second-line treatment settings (Table 1). Data on capecitabine dose
modification and outcomes were available for us to analyze from
4 of these trials (SO14799, NO15542, SO14697, and
SO15179)13,16-19 as well as the phase III capecitabine/docetaxel
combination trial and a retrospective analysis of unselected patients who received capecitabine off protocol, which totaled 971
patients.
Study SO14799 was a randomized, open-label comparison of oral
capecitabine (n ! 61) compared with i.v. CMF (cyclophosphamide
600 mg/m2, methotrexate 40 mg/m2, 5-fluorouracil 600 mg/m2,
once every 3 weeks) (n ! 33) as first-line therapy for advanced breast
cancer or MBC.16 Open-label studies, NO15542 (n ! 74)17 and
SO14697 (n ! 162),13,18 examined the efficacy of capecitabine in
patients with MBC who had failed prior anthracyclines and taxanes.
Study SO15179 randomized patients with MBC pretreated with
anthracycline to oral capecitabine (n ! 22) or i.v. paclitaxel 175
mg/m2 (n ! 20) every 3 weeks.19 The phase III combination trial
randomized patients with anthracycline-pretreated MBC to a starting dose of 1250 mg/m2 b.i.d. capecitabine, orally days 1-14, plus
docetaxel 75 mg/m2 i.v. day 1 (n ! 255) or to docetaxel 100 mg/m2
i.v. alone (n ! 256) every 3 weeks.3 Capecitabine dose modification
was initiated in each of these clinical trials for recurrent treatmentrelated adverse events of NCIC-CTC grade 2 or above.3 The dose of
capecitabine was initially reduced by 25% and subsequently by 50%.
We also considered data published by Hennessy et al15 from a
retrospective analysis of 141 consecutive patients with MBC,
identified from the University of Texas MD Anderson Cancer
Center pharmacy database, who received capecitabine outside of a
clinical trial. The patients were grouped according to capecitabine
Robert Leonard et al
starting dose, with each group analyzed for the frequency of toxicity, dose
reduction, and response rate. The most frequent dose reduction was 20% of
the approved dose, with many patients having received a reduction of approximately 10%. The 3 groups received oral capecitabine twice daily for 14
days, every 3 weeks, as follows: group A (1250 mg/m2 $ 5%), group B
(1125 mg/m2 $ 5%), and group C (1000 mg/m2 # 5%).
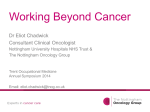
Figure 1 Dose Modification of Capecitabine (from a starting
dose of 1,255 mg/m2 twice daily, days 1-14, every
3 weeks) Prevented the Recurrence of Adverse
Events, and the Development of More Severe
Toxicities, in Study SO14697 in Patients With
Metastatic Breast Cancer Who Had Failed Prior
Anthracyclines and Taxanes
Phase II Monotherapy Trials
Phase III Capecitabine/Docetaxel Combination Trial
Baseline characteristics of patients in the capecitabine/docetaxel
combination trial were well balanced across the treatment groups, as
were the treatment histories.3 The majority of patients had !3 metastatic sites, with the lymph nodes, liver, and bone representing the
most frequent sites of metastasis. Anthracyclines were received by
two thirds of all patients in the metastatic setting and by half of all
patients in the adjuvant and/or neoadjuvant setting. Compared with
single-agent docetaxel, capecitabine/docetaxel combination therapy
was associated with greater median TTP (6.1 vs. 4.2 months, HR
0.652; P ! .0001), median OS (14.5 vs. 11.5 months, HR 0.775;
P ! .0126) and ORR (42% [n ! 107] vs. 30% [n ! 77]; P !
.006).3,4
Improved
Stable
Worsened
100
80
Patients (%)
Patients in the phase II monotherapy trials were aged ! 18 years,
with advanced breast cancer or MBC and a Karnofsky performance
status !70.20 Objective response rates (ORR) achieved with capecitabine ranged from 20% (n ! 27) (95% confidence interval [CI]:
14%-28%) in study SO14697, based on 135 patients with measurable disease, to 36% (n ! 8) (95% CI, 17%-59%) in study SO15179
(Table 1). The median time to progression (TTP) was approximately
3 months with capecitabine across the 4 studies, whereas the median
OS ranged from 7.6 to 19.6 months.16-19
Of the 319 patients who received capecitabine in these trials, 131
(41%) required a 25% reduction in dose, to a mean dose of 941.25
mg/m2, primarily due to the occurrence of adverse events (mainly
HFS). In most patients, one dose reduction of capecitabine prevented the recurrence of the adverse event. However, in 28 patients
(9%), a further reduction to 50% of the starting dose was necessary,
to 627.5 mg/m2. The ORR in patients with first or second capecitabine dose reduction was 32% compared with 15% in those without
dose reduction. Dose reductions tended to favor a longer duration of
response (220 vs. 211 days, respectively), a greater time to treatment
failure (234 vs. 218 days, respectively), and a longer survival (350 vs.
243 days, respectively).
In study SO14697, a post hoc analysis revealed that adverse events
were improved after capecitabine dose modification, whereas efficacy
was maintained.13 Dose reductions for adverse events were necessary
in 54 patients (33%), with a median time to dose reduction of 1.5
months (range, 1.0-2.3 months). Doses were reduced to 75% of the
starting dose in 27% (n ! 44) of patients and to 50% of the starting
dose in 11% (n ! 18) of patients (6% [n ! 10] required 2 dose
reductions). HFS (27% [n ! 44]), diarrhea (18% [n ! 29]), nausea
(9% [n ! 15]), and vomiting (8% [n ! 13]) were the most frequent
cause of dose reductions. However, the incidence of grade 2-4 diarrhea, grade 3 HFS and grade 2-3 stomatitis was improved after dose
modification (Figure 1). Patients who required capecitabine dose
reductions in this study had a similar risk of disease progression as
those who remained on full dose (HR 1.02; P ! .935).
60
40
20
0
Diarrhea Diarrhea Diarrhea HFS
HFS Stomatitis Stomatitis
(Grade 2) (Grade 3) (Grade 4) (Grade 2) (Grade 3) (Grade 2) (Grade 3)
Reproduced with permission from Blum et al. Capecitabine in 162 patients with paclitaxelpretreated MBC: updated results and analysis of dose modification. Eur J Cancer 2001;
37(suppl):190 (abstract 693)
During the study period, 65% (n ! 166) of patients in the capecitabine group required dose reductions compared with 35% (n !
90) in the single-agent docetaxel arm.3 In the combination arm,
doses of both agents were reduced in the majority of patients (51%
[n ! 130] overall); docetaxel only was reduced in 10% (n ! 26) of
patients and capecitabine only in 4% (n ! 10). The combination
group had a longer median time to dose reduction than the singleagent docetaxel group (1.4 vs. 0.8 months for the first dose reduction: 2.8 vs. 2.1 months for the second dose reduction). As expected,
HFS (11.1% [n ! 28]), diarrhea (8.5% [n ! 22]) and stomatitis
(4.6% [n ! 12]) were the adverse events most frequently associated
with capecitabine treatment interruption. However, the recurrence
of these adverse events was effectively managed through capecitabine
dose reduction.3
No negative impact of capecitabine dose reduction on efficacy or
safety was found in a retrospective analysis of this study published by
Leonard et al.14 Kaplan-Meier curves of TTP and OS were compared
in each treatment group for patients who received reduced doses of
both agents from cycle 2 onward (n ! 33) and those who received
full doses of both agents for at least the first 4 cycles (n ! 53). Median
TTP (6.4 vs. 6.7 months) and OS (13.1 vs. 16.3 months) were
similar in both groups (Figure 2).14 The incidence of grade 3/4
adverse events was retrospectively analyzed in relation to the doses of
capecitabine and docetaxel administered at the start of each cycle.
The proportion of treatment cycles with grade 3/4 treatment-related
adverse events was approximately halved when the dose of capecitabine and docetaxel was reduced to 75% of the starting dose (34% vs.
17%); in particular, grade 3/4 HFS (45 cycles full dose vs. 16 cycles
reduced dose), diarrhea, stomatitis, and neutropenic fever occurred
in fewer treatment cycles at this reduced dose level (Figure 3).
Clinical Breast Cancer December 2011
351
Capecitabine Dose Modification
Figure 2 Kaplan-Meier Curves of (A) Time to Progression and
(B) Overall Survival for Patients in the Capecitabine/
Docetaxel Combination Trial, Requiring Dose
Reduction of Capecitabine and Docetaxel From Cycle 2
Onward (“both reduced”) (n ! 33) vs. Those Who
Received Full Starting Doses of Both Agents for at
Least the First 4 Cycles (“both full dose”) (n ! 53)
A
Estimated Probability
0.8
0.6
Cycle 4: Both Full Dose
(Capecitabine 1250 mg/m2 b.i.d.,
Docetaxel 75 mg/m2)
Median
0.4
0.2
6.4
0
5
6.7
10
15
20
25
30
Months
B
Estimated Probability
1.0
0.6
Both Full Dose
Both Reduced Dose
(670 Cycles Administered)
(450 Cycles Administered)
40
30
20
10
0
Stomatitis
HFS
Neutropenic
Fever
Median
0.4
Reproduced with permission from Leonard et al. Detailed analysis of a randomized phase III trial:
can the tolerability of capecitabine plus docetaxel be improved without compromising its survival
advantage? Ann Oncol 2006; 17:1379-85.
0.2
13.1
0
5
10
16.3
15
20
25
30
35
40
45
50
Months
Reproduced with permission from Leonard et al. Detailed analysis of a randomized phase III trial:
can the tolerability of capecitabine plus docetaxel be improved without compromising its survival
advantage? Ann Oncol 2006; 17:1379-85.
Retrospective Analysis of Consecutive Patients Who
Received Capecitabine Outside a Clinical Trial
Of the 141 patients who received capecitabine consecutively, 113
were evaluable for response or tolerability, including one male patient. Baseline characteristics were generally well balanced (Table 2),
although patients who received 1000 mg/m2 b.i.d. oral capecitabine
were younger than those in the other 2 dose groups. In addition,
patients who received the lower doses (1000 mg/m2 and 1125 mg/
m2) tended to be more heavily pretreated, 38% (n ! 17) and 41%
(n ! 7) of patients, respectively, had received !3 prior regimens for
metastatic disease, compared with 24% (n ! 12) of patients in the
1250 mg/m2 dose group.15
The mean starting dose of capecitabine was 1110 mg/m2 b.i.d.,
and a median of 4 therapy cycles (range, 1-19) was administered.
Overall, the mean tolerated dose of capecitabine was approximately
20% lower than the licensed dose, at 1020 mg/m2. No clear dosetoxicity relationship was observed, with dose reductions required by
41% (n ! 21) of patients at the 1250 mg/m2 dose level and 63%
(n ! 11) at the 1125 mg/m2 dose level. At the 1000 mg/m2 b.i.d.
dose, 28% (n ! 13) of patients required capecitabine dose modification. As expected, incidences of the most recurrent adverse events
352
50
Diarrhea
0.8
0
Number of Cycles
Reporting Adverse Events
Cycle 2: Both Reduced
(Capecitabine 950 mg/m2 b.i.d.,
Docetaxel 55 mg/m2)
1.0
0
Figure 3 Impact of Capecitabine and Docetaxel Dose
Reduction on the Proportion of Treatment Cycles
With Grade 3/4 Treatment-related Adverse Events in
Patients Who Required Dose Reduction of
Capecitabine and Docetaxel (“both reduced dose”)
(capecitabine 950 mg/m2 twice daily, days 1-14,
every 3 weeks; docetaxel 55 mg/m2 day 1, every 3
weeks) vs. Those Who Received Full Starting Doses
of Both Agents (“both full dose”) (capecitabine
1250 mg/m2 twice daily, days 1-14, every 3 weeks,
docetaxel 75 mg/m2 day 1, every 3 weeks).
Clinical Breast Cancer December 2011
were lower in patients who had capecitabine initiated at the lowest
dose level. Grade 3 HFS, the most frequently reported adverse event
(33% [n ! 35] of all patients), occurred in 20% (n ! 8) of patients
who received 1000 mg/m2 b.i.d. capecitabine compared with 33%
(n ! 17) of patients who received the highest dose. Similarly, grade
3/4 diarrhea (13% [n ! 7] vs. 3% [n ! 1]) and grade 3/4 stomatitis
(8% [n ! 4] vs. 3% [n ! 1]) were more frequent with the 1250
mg/m2 b.i.d. capecitabine dose than with the lowest dose. The lower
doses of capecitabine did not compromise efficacy, in terms of ORR
or TTP, vs. the standard 1250 mg/m2 b.i.d. dose (Table 2).15
Efficacy of Lower-Dose Capecitabine in Prospective
Clinical Trials
Given that the median capecitabine dose delivered in the phase III
capecitabine/docetaxel combination trial was approximately 960
mg/m2,14 more recent studies of capecitabine have used, or are using,
a reduced starting dose of between 825 and 1000 mg/m2 to reduce
the incidence of adverse events, with the aim also of not compromising the efficacy of the drug.21
A lower starting dose of capecitabine is highly effective in the
first-line MBC setting.11,22 In the randomized, phase III ANZBCTG 0001 (Australia and New Zealand Breast Cancer Trials
Group) trial, Stockler et al11 compared classic i.v. CMF and 2-dose
schedules of oral capecitabine (1000 mg/m2 b.i.d. for 14 days every 3
weeks, and 625 mg/m2 b.i.d. without interruption) in women with
MBC unsuitable for intensive chemotherapy (n ! 352). Overall
response rates were similar across the treatment groups: 22% (n !
24), 20% (n ! 21), and 18% (n ! 20) with 1000 mg/m2 capecitabine, 625 mg/m2 capecitabine and CMF, respectively, as was me-
Robert Leonard et al
Table 2 Baseline Characteristics and Response to Capecitabine in a Retrospective Analysis of Patients with MBCa
All
n ! 113
1250 mg/m2
n ! 51
1125 mg/m2
n ! 17
1000 mg/m2
n ! 45
52.5 (26-77)
54 (30-77)
56 (40-75)
49 (26-70)
Soft Tissue/Bone
33 (29)
14 (27)
5 (29)
15 (33)
Visceral
21 (19)
11 (22)
3 (18)
8 (18)
Combination
59 (52)
26 (51)
9 (53)
22 (49)
Positive
51 (45)
22 (43)
7 (41)
22 (49)
Negative
50 (44)
24 (47)
8 (47)
18 (40)
!3 Regimens
36 (32)
12 (24)
7 (41)
17 (38)
Anthracycline
109 (96)
45 (88)
15 (88)
44 (98)
Taxane
102 (90)
49 (96)
17 (100)
40 (89)
Anthracycline and Taxane
101 (89)
46 (90)
14 (82)
40 (89)
105
49
15
41
Dose Group No.
Patients
Median (Range) Age, y
Metastatic Sites, n (%)
ER status, n (%)
Prior therapy for metastatic disease, n (%)
No. Patients Evaluable for Response
ORR, n (%)
22 (21)
9 (18)
3 (20)
10 (24)
Stable disease, n (%)
39 (37)
17 (35)
7 (47)
15 (37)
Progressive disease, n (%)
44 (42)
23 (47)
5 (33)
16 (39)
Median (95% CI) TTP, mo
3.2 (0.7-19)
2.8 (0.7-19)
4.6 (1.4-9.4)
3.5 (1.3-12.6)
Abbreviations: CI ! confidence interval; ER ! estrogen receptor; ORR ! objective response rate; TTP ! time to progression.
a
All doses are twice daily and based on a 3-weekly treatment cycle.
dian progression-free survival (PFS): 6 months in both of the capecitabine groups and 7 months with CMF. However, median OS was
significantly prolonged with capecitabine vs. CMF (22 vs. 18
months, HR 0.72; P ! .02). Capecitabine was generally well tolerated; the most frequently reported grade 3/4 adverse events in the
1000 mg/m2 and 625 mg/m2 dosing groups, respectively, were HFS
(15% [n ! 16] and 16% [n ! 17]), diarrhea (6% [n ! 6] and 8%
[n ! 9]), and infection (8% [n ! 9] and 4% [n ! 4]). Overall, the
safety profiles of the 2 capecitabine regimens were comparable. More
recently, Kaufmann et al22 conducted a multicenter, single-arm,
phase II study of first-line oral capecitabine monotherapy (1000
mg/m2 b.i.d.) in women with medium-risk negative human epidermal growth factor receptor 2 (HER2–) MBC (n ! 161). The ORR
was 26.1% (n ! 42), with a high disease control rate (ORR plus
stable disease !6 months) of 64% (n ! 103), and a median TTP of
7.3 months (95% CI, 6.2-8.4 months). A multivariate subgroup
analysis demonstrated particular benefit in patients aged %65 years
vs. those aged "65 years (TTP, 38.0 vs. 26.8 weeks; P ! .002), and
patients with vs. without HFS (TTP, 40.8 vs. 20.4 weeks [P !
.0542]; OS, 99.7 vs. 61.7 weeks [P ! .0209]). Note that patients
aged %65 years received a higher mean dose of capecitabine than
those aged "65 years (439 vs. 361 mg, respectively), as did those
with vs. without HFS (474 vs. 352 mg, respectively). First-line capecitabine showed a favorable tolerability profile in this study; the most
common grade 3/4 nonhematologic adverse event was HFS (7.5%
[n ! 12]).
Lower-dose capecitabine also is efficacious when combined with
biologic or targeted therapies.12,23-25 The randomized, placebo-con-
trolled, phase III RIBBON-1 trial evaluated the combination of bevacizumab with first-line chemotherapy (investigator’s choice of anthracyclines, taxanes, or 1000 mg/m2 b.i.d. oral capecitabine) in
patients with HER2– MBC (n ! 1237).12 After a median follow-up
of 19.2 months, analysis of median PFS revealed a significant benefit
in favor of the capecitabine/bevacizumab arm over the capecitabine/
placebo arm (8.6 vs. 5.7 months, HR 0.69; P ! .0002; investigator
assessment). This benefit was confirmed by an independent review
committee (9.8 vs. 6.2 months, HR 0.68; P ! .0011) and was found
to be independent of baseline patient risk factors.12
The combination of capecitabine (1000 mg/m2 b.i.d. orally) and
lapatinib was compared with single-agent capecitabine (1250 mg/m2
b.i.d. orally) in a randomized, open-label, multinational, phase III
trial by Geyer et al23 in women with progressive, HER2#, locally
advanced breast cancer or MBC (n ! 399). Patients in the combination arm had significantly prolonged median TTP (5.5 vs. 4.2
months, HR 0.72; P ! .008)23 and a higher ORR (24% [n ! 48] vs.
14% [n ! 28], P ! .017)24 than the monotherapy arm. Adverse
events were similar across both groups, with diarrhea, HFS, nausea,
fatigue, vomiting, and rash occurring most frequently. The randomized, open-label, phase II Capecitabine, Herceptin and Taxotere
(CHAT) study by Wardley et al25 evaluated the efficacy and safety of
first-line trastuzumab (6 mg/kg i.v. after a 8 mg/kg loading dose) plus
docetaxel (75 or 100 mg/m2 i.v.) with or without capecitabine (950
mg/m2 b.i.d. orally) in patients with HER2-overexpressing, inoperable, locally advanced breast cancer or MBC (n ! 222). After a
median follow-up of %23 months, the median PFS (17.9 vs. 12.8
months, HR 0.72; P ! .0402) and median TTP (18.6 vs. 13.6
Clinical Breast Cancer December 2011
353
Capecitabine Dose Modification
months, HR 0.70; P ! .029) were significantly higher in the capecitabine-containing arm than in the trastuzumab/docetaxel arm. The
safety profile of both regimens was manageable, with grade 3 HFS
(17% [n ! 19] vs. "1% [n ! 1]) and grade 3/4 diarrhea (11% [n !
12] vs. 4% [n ! 4]), more common with the triple combination
regimen.
Several studies in the MBC setting, which combined new and
established cytotoxic agents with capecitabine, had also chosen a
capecitabine starting dose of 1000 mg/m2 b.i.d.26-31 The Solid Tumor Intensification (SOLTI)-0701, double-blind, randomized,
phase IIb trial evaluated the combination of capecitabine (1000
mg/m2 b.i.d. orally for 14 days every 3 weeks) with sorafenib or
placebo in patients with HER2– locally advanced breast cancer or
MBC (n ! 229).26 Significant improvements in PFS were observed
in the capecitabine/sorafenib arm compared with the capecitabine/
placebo arm (6.4 vs. 4.1 months, respectively, HR 0.576; P !
.0006). This PFS benefit was maintained in all prespecified subgroup
analyses, including age ("65 vs. !65 years), hormone receptor status (positive vs. negative), measurable disease (yes vs. no), and visceral disease (yes vs. no).27 There was a low incidence of grade 3/4
adverse events in the study, with the exception of grade 3 HFS, which
was greatly increased in the capecitabine/sorafenib arm vs. the capecitabine/placebo arm (45% [n ! 52] vs. 13% [n ! 15], respectively).
Thomas et al28 conducted a randomized, open-label phase III study
that compared ixabepilone plus capecitabine (1000 mg/m2 b.i.d.
orally) with capecitabine alone (1250 mg/m2 b.i.d. orally) in patients
with locally advanced breast cancer or MBC pretreated with or resistant to anthracyclines and resistant to taxanes with (n ! 752). Patients who received combination therapy had significantly longer
median PFS than those in the monotherapy arm (5.8 vs. 4.2 months,
HR 0.75; P ! .0003) as well as greater ORR (35% [n ! 130] vs.
14% [n ! 54], respectively; P " .0001). Capecitabine-related adverse events were similar in both groups. These data suggest that
capecitabine 1000 mg/m2 b.i.d., as a single agent and as part of a
combination regimen, represent an effective and safe dose in patients
with MBC previously treated with an anthracycline or a taxane.
A number of key ongoing trials are using a capecitabine dose of 1000
mg/m2 b.i.d. orally; results of these trials are eagerly awaited. A phase III,
randomized, open-label Central European Cooperative Oncology
Group study will determine the efficacy of capecitabine/bevacizumab vs.
paclitaxel/bevacizumab as first-line therapy in patients with locally recurrent breast cancer or MBC. Interim safety subgroup analyses from
the study support the safety of these regimens.32 In addition, patients are
being recruited to a single-arm open-label, phase II study of capecitabine
in combination with bevacizumab and trastuzumab as first-line treatment of HER2# locally recurrent breast cancer or MBC; interim safety
data will be reported in 2011.
Even lower initial capecitabine doses have demonstrated efficacy,
in combination with a taxane, with manageable safety profiles.33-38
Blum et al34 conducted a multicenter phase II trial of 825 mg/m2
oral capecitabine b.i.d., plus 80 mg/m2 i.v. paclitaxel weekly, every 3
weeks, in patients with taxane-pretreated MBC (n ! 54). The regimen produced a high ORR of 59% (n ! 32) (95% CI, 46%-72%),
a median TTP of 10.1 months, and a median OS of 17 months.
There was a low rate of grade 3/4 treatment-related adverse events:
HFS 20% (n ! 11), neutropenia 13% (n ! 7), fatigue 7% (n ! 4),
354
Clinical Breast Cancer December 2011
diarrhea 4% (n ! 2), nausea/vomiting 4% (n ! 2), pain 2% (n ! 1),
and anemia 2% (n ! 1). Thirty patients required capecitabine dose
reductions, which were effective in allowing continued treatment. A
similar study by Gradishar et al35 by using a dose of 825 mg/m2 b.i.d.
oral capecitabine (n ! 47) in combination with paclitaxel, produced
an ORR of 51% (n ! 24) (95% CI, 3%8-64%), a median TTP of
10.6 months, and a median OS of 29.9 months. Neutropenia (15%
[n ! 7]), alopecia (13% [n ! 6]), and HFS (11% [n ! 5]) were the
most frequently reported grade 3/4 treatment-related adverse events.
Soto et al,36 on behalf of the Mexican Oncology Study Group, compared the effect of capecitabine (825 mg/m2 b.i.d. orally) plus taxane
combination therapy vs. capecitabine (1250 mg/m2 b.i.d. orally)
followed by taxane in patients with anthracycline-pretreated MBC
(n ! 277). The patients in the combination group had significantly
greater ORR (paclitaxel, 65% [n ! 62] [P ! .01]; docetaxel, 74%
[n ! 67] [P ! .0002]) than those who received capecitabine/taxane
sequentially (46% [n ! 42]). Median PFS and median OS were
similar across all treatment groups. Adverse events were as expected
in each arm, with alopecia the most frequently reported grade 3/4
event in the combination arms. Grade 3 HFS occurred in fewer than
20% (n " 19) of patients in each treatment arm.
Novel Capecitabine Dosing Schedules in MBC
As well as modifying the dose of capecitabine, investigators have
examined the use of novel dose schedules in an attempt to reduce
toxicity while maintaining the efficacy of the drug.21,39 In the phase
III trial by Stockler et al,11 similar efficacy and comparable safety was
seen with oral capecitabine 1000 mg/m2 b.i.d., days 1-14, every 3
weeks, and 625 mg/m2 b.i.d. without interruption. A number of
Japanese studies have demonstrated high clinical activity with a
4-week intermittent dosing schedule of 825 mg/m2 b.i.d. capecitabine, days 1-21 orally, followed by a 7-day rest period, with a safety
profile similar to that of the standard 3-weekly intermittent regimen.40,41 Furthermore, modest efficacy and an acceptable safety profile were reported with a 7/7 dosing schedule of oral capecitabine (7
days of treatment every 14 days), 1000 mg/m2 b.i.d., days 1-7, followed by a 7-day rest period, when administered in combination
with bevacizumab (n ! 41).42 After a median of 7 cycles (range,
1-32), 20% (n ! 8) of patients experienced a partial response,
whereas 35% (n ! 14) had stable disease that lasted !6 months.
Grade 3 HFS (20% of patients), grade 3/4 hypertension (10% [n !
4]), and grade 3/4 fatigue (2% [n ! 1]) were the most frequently
reported treatment-related adverse events. A number of ongoing trials are evaluating the 7/7 capecitabine regimen, both as monotherapy
and in combination regimens in patients with MBC. The patients
who received this dosing schedule as a result of toxicity should have
their capecitabine dose increased as described in the original Memorial Sloane Kettering Cancer Center (MSKCC) phase I study.43
More recently, results from a randomized phase II Grupo Español de
Investigación en Cáncer de Mama (GEICAM)-sponsored study suggest that the standard intermittent capecitabine regimen may be
more effective than a continuous regimen that uses a lower dose (800
mg/m2 b.i.d., orally days 1-21, every 3 weeks).44 Thus, although it
appears safe and effective to lower the capecitabine dose from 1250
mg/m2 b.i.d. to 1000 mg/m2 b.i.d., analysis of randomized data
Robert Leonard et al
suggests that it is important to maintain as high a dose as possible,
without compromising safety, on the standard intermittent schedule.
Conclusions
Data presented in this review demonstrate that the dose of capecitabine can be reduced, either when used as monotherapy or in
combination with docetaxel to minimize adverse events without
compromising efficacy in terms of TTP or OS. Results of the retrospective analysis of patients not in a clinical trial support a starting
dose of 1000 mg/m2 b.i.d. capecitabine, even as a single agent, due to
its superior therapeutic index compared with the licensed starting
dose. Prospective, randomized, phase III studies of patients with
MBC, such as the ANZBCTG 0001 and Regimens in Bevacizumab
for Breast Oncology (RIBBON)-1 trials, also have demonstrated the
efficacy of a 1000 mg/m2 b.i.d. oral initial dose of capecitabine. Data
from a number of ongoing trials will provide further evidence concerning the effectiveness of this regimen. To date, these data support
the feasibility of dose-reducing capecitabine, including the possibility of starting at a lower dose, to minimize the incidence of adverse
events and thereby allow patients to remain on effective therapy
longer.
Disclosure
Support for third-party writing assistance for this article was provided by F. Hoffmann-La Roche Ltd, Basel, Switzerland. Professor
Leonard has acted as a consultant for Roche Advisory Boards and has
received speaker honoraria from Roche. Dr. Blum has acted as a
consultant for Roche Advisory Boards. Dr. O’Shaughnessy has acted
as a consultant for Roche Advisory Boards. Dr. Hennessy has no
conflicts of interest to disclose.
References
1. Seidman AD, O’Shaughnessy J, Misset J-L. Single-agent capecitabine: a reference
treatment for taxane-pretreated metastatic breast cancer? Oncologist 2002; 7(suppl
6):20-8.
2. Ershler WB. Capecitabine monotherapy: safe and effective treatment for metastatic
breast cancer. Oncologist 2006; 11:325-35.
3. O’Shaughnessy J, Miles D, Vukelja S, et al. Superior survival with capecitabine plus
docetaxel combination therapy in anthracycline-pretreated patients with advanced
breast cancer: phase III trial results. J Clin Oncol 2002; 20:2812-23.
4. Miles D, Vukelja S, Moiseyenko V, et al. Survival benefit with capecitabine/docetaxel versus docetaxel alone: analysis of therapy in a randomized phase III trial.
Clin Breast Cancer 2004; 5:273-8.
5. Liu G, Franssen E, Fitch M, et al. Patient preferences for oral versus intravenous
palliative chemotherapy. J Clin Oncol 1997; 15:110-5.
6. Borner M, Schöffski P, de Wit R, et al. Patient preference and pharmacokinetics of
oral modulated UFT versus intravenous fluorouracil and leucovorin: a randomised
crossover trial in advanced colorectal cancer. Eur J Cancer 2002; 38:349-58.
7. Gǒrnaś M, Sczcylik C. Oral treatment of metastatic breast cancer with capecitabine:
what influences the decision-making process? Eur J Cancer Care 2010; 19:131-6.
8. Scheithauer W, Blum J. Coming to grips with hand-foot syndrome. Insights from
clinical trials evaluating capecitabine. Oncology 2004; 18:1161-84.
9. Cassidy J, Twelves C, Van Cutsem E, et al. First-line oral capecitabine therapy in
metastatic colorectal cancer: a favorable safety profile compared with intravenous
5-fluorouracil/leucovorin. Ann Oncol 2002; 13:566-75.
10. Midgley R, Kerr DJ. Capecitabine: have we got the dose right? Nat Clin Pract Oncol
2009; 6:17-24.
11. Stockler M, Sourjina T, Grimison P, et al. A randomized trial of capecitabine (C)
given intermittently (IC) rather than continuously (CC) compared to classical CMF
as first-line chemotherapy for advanced breast cancer (ABC). J Clin Oncol 2007;
25(suppl):39s (abstract 1031).
12. Robert NJ, Dieras V, Glaspy J, et al. RIBBON-1: randomized, double-blind, placebo-controlled, phase III trial of chemotherapy with or without bevacizumab for
first-line treatment of human epidermal growth factor receptor 2-negative, locally
recurrent or metastatic breast cancer J Clin Oncol 2011; 29:1252-60.
13. Blum JL, Jones SE, Buzdar AU, et al. Capecitabine in 162 patients with paclitaxelpretreated MBC: updated results and analysis of dose modification. Eur J Cancer
2001; 37(suppl):190 (abstract 693).
14. Leonard R, O’Shaughnessy J, Vukelja S, et al. Detailed analysis of a randomized
phase III trial: can the tolerability of capecitabine plus docetaxel be improved without compromising its survival advantage? Ann Oncol 2006; 17:1379-85.
15. Hennessy BT, Gauthier AM, Michaud LB, et al. Lower dose capecitabine has a
more favorable therapeutic index in metastatic breast cancer: retrospective analysis
of patients treated at M.D. Anderson Cancer Center and a review of capecitabine
toxicity in the literature. Ann Oncol 2005; 16:1289-96.
16. O’Shaughnessy JA, Blum J, Moiseyenko V, et al. Randomized, open-label, phase II
trial of oral capecitabine (Xeloda) vs. a reference arm of intravenous CMF (cyclophosphamide, methotrexate and 5-fluorouracil) as first-line therapy for advanced/
metastatic breast cancer. Ann Oncol 2001; 12:1247-54.
17. Blum JL, Dieras V, Lo Russo PM, et al. Multicenter, phase II study of capecitabine in taxane-pretreated metastatic breast carcinoma patients. Cancer 2001;
92:1759-68.
18. Blum JL, Jones SE, Buzdar AU, et al. Multicenter phase II study of capecitabine in
paclitaxel-refractory metastatic breast cancer. J Clin Oncol 1999; 17:485-93.
19. Talbot DC, Moiseyenko V, Van Belle S, et al. Randomised, phase II trial comparing
oral capecitabine (Xeloda) with paclitaxel in patients with metastatic/advanced
breast cancer pretreated with anthracyclines. Br J Cancer 2002; 86:1367-72.
20. O’Shaughnessy J, Blum J. A retrospective evaluation of the impact of dose reduction
in patients treated with Xeloda® (capecitabine). Proc Am Soc Clin Oncol 2000;
19(suppl):28s (abstract 400).
21. Zielinski C, Gralow J, Martin M. Optimising the dose of capecitabine in metastatic
breast cancer: confused, clarified or confirmed? Ann Oncol 2010; 21:2145-52.
22. Kaufmann M, Maass N, Costa SD, et al. First-line therapy with moderate dose
capecitabine in metastatic breast cancer is safe and active: results of the MONICA
trial. Eur J Cancer 2010; 46:3184-91.
23. Geyer CE, Forster J, Lindquist D, et al. Lapatinib plus capecitabine for HER2positive advanced breast cancer. N Engl J Med 2006; 355:2733-43.
24. Cameron D, Casey M, Press M, et al. A phase III randomized comparison of
lapatinib plus capecitabine versus capecitabine alone in women with advanced
breast cancer that has progressed on trastuzumab: updated efficacy and biomarker
analyses. Breast Cancer Res Treat 2008; 112:533-43.
25. Wardley AM, Pivot X, Morales-Vasquez F, et al. Randomized phase II trial of
first-line trastuzumab plus docetaxel and capecitabine compared with trastuzumab
plus docetaxel in HER2-positive metastatic breast cancer. J Clin Oncol 2010; 28:
976-83.
26. Baselga J, Segalla JGM, Roché H, et al. SOLTI-0701: a double-blind, randomized
phase 2b study evaluating the efficacy and safety of sorafenib (SOR) compared to
placebo (PL) when administered in combination with capecitabine (CAP) in patients (pts) with locally advanced (adv) breast cancer. Eur J Cancer 2009; 7(suppl):
3-4 (abstract 3LBA).
27. Baselga J, Grupo Español de Estudio Tratamiento y Otras Estrategias Experimentales en Tumores Sólidos, Roché H, et al. SOLTI-0701: A multinational doubleblind, randomized phase 2b study evaluating the efficacy and safety of sorafenib
compared to placebo when administered in combination with capecitabine in patients with locally advanced or metastatic breast cancer. Paper presented at: the 32nd
Annual San Antonio Breast Cancer Symposium; December 10-13, 2009; San Antonio, TX. Abstract 45.
28. Thomas ES, Gomez HL, Li RK, et al. Ixabepilone plus capecitabine for metastatic
breast cancer progressing after anthracycline and taxane treatment. J Clin Oncol
2007; 25:5210-7.
29. Jones A, O’Brien M, Sommer H, et al. Phase II study of oral vinorelbine in combination with capecitabine as second line chemotherapy in metastatic breast cancer
patients previously treated with anthracyclines and taxanes. Cancer Chemother Pharmacol 2010; 65:755-63.
30. Chew HK, Barlow WE, Albain K, et al. A phase II study of imatinib mesylate and
capecitabine in metastatic breast cancer: Southwest Oncology Group Study 0338.
Clin Breast Cancer 2008; 8:511-5.
31. Oksuzoglu B, Abali H, Havran M, et al. Capecitabine and cisplatin combination is
an active and well-tolerated doublet in the treatment of metastatic breast carcinoma
patients pretreated with anthracycline and taxanes. Chemotherapy 2008; 54:352-6.
32. Lang I, Inbar MJ, Greil R, et al. Safety subgroup analyses from the CECOG phase
III TURANDOT trial: first-line bevacizumab (Bev) in combination with capecitabine (X) or paclitaxel (P) for HER2-negative locally recurrent or metastatic breast
cancer (LR/MBC). Eur J Cancer 2010; 8(suppl):viii98 (abstract 281PD).
33. Blum JL, Dees EC, Chacko A, et al. Phase II trial of capecitabine and weekly
paclitaxel as first-line therapy for metastatic breast cancer. J Clin Oncol 2006; 24:
4384-90.
34. Blum JL, Claire Dees E, Vukelja SJ, et al. Phase II trial of capecitabine and weekly
paclitaxel in patients with metastatic breast cancer previously treated with every-3week taxane therapy. Clin Breast Cancer 2007; 7:465-70.
35. Gradishar WJ, Meza LA, Amin B, et al. Capecitabine plus paclitaxel as front-line
combination therapy for metastatic breast cancer: a multicenter phase II study.
J Clin Oncol 2004; 22:2321-7.
36. Soto C, Torrecillas L, Reyes S, et al. Capecitabine and taxanes in patients with
anthracycline-pretreated metastatic breast cancer: sequential vs. combined therapy
results from a Mexican Oncology Study Group (MOSG) randomized phase III trial.
J Clin Oncol 2006; 24(suppl):20s (abstract 570).
37. Perez EA, Hillman DW, Dentchev T, et al. North Central Cancer Treatment
Group (NCCTG) N0432: phase II trial of docetaxel with capecitabine and bevacizumab as first-line chemotherapy for patients with metastatic breast cancer. Ann
Oncol 2010; 21:269-74.
Clinical Breast Cancer December 2011
355
Capecitabine Dose Modification
38. Ghosn M, Kattan J, Farhat F, et al. Sequential vinorelbine-capecitabine followed by
docetaxel in advanced breast cancer: long-term results of a pilot phase II trial. Cancer
Chemother Pharmacol 2008; 62:11-8.
39. Naughton M. Evolution of capecitabine dosing in breast cancer. Clin Breast Cancer
2010; 10:130-5.
40. Kusama M, Nomizu T, Aogi K, et al. Phase II study of 4-weekly capecitabine
monotherapy in advanced/metastatic breast cancer. Breast Cancer 2010; 17:233-40.
41. Taguchi T, Nakayama T, Masuda N, et al. Study of low-dose capecitabine for
metastatic breast cancer. Chemotherapy 2010; 56:166-70.
42. Gajria D, Feigin K, Tan, LK, et al. Phase 2 trial of a novel capecitabine dosing
schedule in combination with bevacizumab for patients with metastatic breast cancer. Cancer 2011. [Epub ahead of print].
43. Traina TA, Theodoulou M, Feigin K, et al. Phase I study of a novel capecitabine
schedule based on the Norton-Simon mathematical model in patients with metastatic breast cancer. J Clin Oncol 2008; 26:1797-802.
356
Clinical Breast Cancer December 2011
44. Martín M, Martínez N, Ramos M, et al. Randomized, phase II trial comparing
continuous vs intermittent capecitabine (X) monotherapy for metastatic breast cancer (MBC): results from the GEICAM 2009-05 study. J Clin Oncol 2011; 29(suppl
15S):82s (abstract 1008).
45. Reichardt P, von Minckwitz G, Thuss-Patience PC, et al. Multicenter phase II
study of oral capecitabine (Xeloda®) in patients with metastatic breast cancer
relapsing after treatment with a taxane-containing therapy. Ann Oncol 2003;
14:1227-33.
46. Fumoleau P, Largillier R, Clippe C, et al. Multicentre, phase II study evaluating
capecitabine monotherapy in patients with anthracycline-and taxane-pretreated
metastatic breast cancer. Eur J Cancer 2004; 40:536-42.
47. Largillier R, Fumoleau P, Clippe C, et al. Capecitabine monotherapy after anthracycline and taxane failure in metastatic breast cancer (MBC): long-term survival
data. Ann Oncol 2006; 17(suppl 9):ix74.