Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
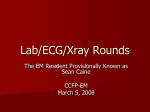
Advances in Cardiovascular Imaging Imaging Phenotype Versus Genotype in Hypertrophic Cardiomyopathy Milind Y. Desai, MD; Steve R. Ommen, MD; William J. McKenna, MD; Harry M. Lever, MD; Perry M. Elliott, MD H Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 ypertrophic cardiomyopathy (HCM) is a common monogenetic cardiac disease with a prevalence of 0.2%1 that usually is inherited as an autosomal dominant trait with variable penetrance and expression. Clinically, HCM is defined by the presence of left ventricular (LV) hypertrophy (LVH) unexplained by abnormal loading conditions.1 The natural history varies from an asymptomatic course to drugrefractory angina/dyspnea, sudden cardiac death (SCD), and end-stage heart failure. The incidence of HCM-related SCD is approximately 1% to 2% in children and adolescents and 0.5% to 1% in adults.2,3 In this review, we examine the impact of advanced diagnostic imaging technologies on HCM, with particular emphasis on the detection of particular genetic subtypes. only a single functional copy of a gene, the other being inactivated by the mutation) also may be important. It is suggested that hypertrophy results from reduced contractile function, but studies of myocyte function in patients with mutations in sarcomere protein genes are contradictory. Nevertheless, murine models of sarcomeric mutations show increased calcium sensitivity and altered calcium cycling between sarcomere and sarcoplasmic reticulum. In vitro studies using purified myosin filaments and skinned papillary muscle have reported increased calcium sensitivity of force development that results in impaired ventricular relaxation in vivo.17,18 Z-discs are lateral boundaries of the sarcomere that play a fundamental role in mechanical stretch sensing. Several mutations in genes coding for Z-disc proteins have been implicated in HCM, including ␣-actinin (mediates the interaction between actin and titin) and telethonin (interacts with muscle LIM protein and titin).19,20 More recently, melusin, a muscle-specific signaling protein required for compensatory hypertrophy response in the pressure-overloaded heart, also has been implicated.21 A detailed description of metabolic cardiomyopathies that mimic HCM is described in the later part of this article. State-of-the Art in Genetics of HCM In ⬇60% of cases, HCM is inherited as an autosomal dominant trait caused by mutations in genes coding for cardiac sarcomere proteins (Figure 1).4 –7 Mutations in genes encoding Z-disc proteins and proteins involved in calcium regulation account for ⬍5% of cases. The absence of sarcomeric gene mutations can be explained by limitations of current mutation detection techniques or mutations in as yet unidentified genes, but in some cases, hypertrophy is caused by other diseases that mimic the phenotype of sarcomeric protein disease. Table 1 lists genetic disorders associated with HCM. State-of-the-Art in Imaging in HCM In recent years, a comprehensive approach incorporating multiple imaging modalities has been used to determine mechanisms of symptoms and prognosis and to plan therapy. The utility and limitations of each imaging modality are listed in Table 2; current recommendations for use of different imaging modalities are listed in Table 3. Sarcomere and Z-disc Protein Gene Mutations More than 600 different sarcomeric gene mutations are reported in patients with HCM.8 –16 The majority are missense mutations, but nonsense, frameshift, and in-frame insertion/ deletion mutations also occur. Most mutations are characterized by incomplete penetrance and variable clinical expression likely due to locus heterogeneity and the effect of mutations at different locations within the same gene. Most mutations probably have a dominant negative effect on sarcomere function, but in some cases, haploinsufficiency (ie, Assessment of Morphology LV Geometry Echocardiography is the initial modality of choice for evaluation of cardiac morphology. Although asymmetrical upperseptal hypertrophy is the most commonly observed morphological pattern (Figure 2A and 2B),22 midventricular, apical Received May 5, 2010; accepted November 18, 2010. From the Heart and Vascular Institute (M.Y.D.), Cleveland Clinic, and Cleveland Clinic Foundation (H.M.L.), Cleveland, OH; Department of Cardiovascular Medicine (S.R.O.), Mayo Clinic, Rochester, MN; and Department of Cardiovascular Medicine (W.J.M., P.M.E.), The Heart Hospital, University College, London, England. The online-only Data Supplement is available at http://circimaging.ahajournals.org/cgi/content/full/CIRCIMAGING/4/2/156/DC1. Correspondence to Milind Y. Desai, MD, Heart and Vascular Institute, Desk J1–5, Cleveland Clinic, 9500 Euclid Ave, Cleveland, OH 44195. E-mail [email protected] (Circ Cardiovasc Imaging. 2011;4:156-168.) © 2011 American Heart Association, Inc. Circ Cardiovasc Imaging is available at http://circimaging.ahajournals.org 156 DOI: 10.1161/CIRCIMAGING.110.957936 Desai et al Hypertrophic Cardiomyopathy 157 Figure 1. A schematic illustration of a cardiac sarcomere. Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 (Figure 3A and 3B), posterolateral, concentric, and biventricular hypertrophy also occur. Three-dimensional echocardiography quantifies and characterizes myocardial hypertrophy, LV volumes, LV ejection fraction, and LV mass more accurately than traditional 2D echocardiography.23 Cardiac magnetic resonance (CMR) is especially useful in identifying the varied phenotypic presentations of HCM, particularly when hypertrophy involves the anterolateral free wall24 and apical variant,25 which often are poorly visualized on echocardiography. In 1 study,24 CMR accurately identified Table 1. HCM missed on echocardiography in 6% of the patients. CMR is the gold standard for measurement of LV mass, which might have some prognostic utility.26 Recently, a high prevalence of apical aneurysms, missed by echocardiography in 43% cases (albeit, without the use of contrast), was demonstrated using CMR.27 Currently, CMR cannot be used in most patients with pacemakers or implanted defibrillators; however, this may change as newer safety data emerge. As an alternative to CMR, cardiac CT can be used for morphological charac- Currently Known Genes Implicated in HCM Protein Frequency in Patients With HCM Phenotype Associated Phenotype MYH7 -myosin heavy chain 25%–35% Variable MYBPC3 Variable, late onset Gene Sarcomeric mutations Myosin-bindingproteinC 20%–30% TNNT2 Troponin T 3%–5% Sudden death TNNI3 Troponin I ⬍5% Extreme heterogeneity TPM1 Tropomyosin 1␣ ⬍5% Variable prognosis, sudden death MYL2 Regulatory myosin light chain 2 ⬍5% Skeletal myopathy MYL3 Essential myosin light chain 3 Rare Skeletal myopathy ACTC ␣-Cardiac actin 1 Rare Apical hypertrophy TTN Titin Rare Typical TNNC1 Troponin C, slow skeletal and cardiac muscles Rare Typical MYH6 ␣-Myosin heavy chain Rare Late onset CSRP3 Muscle LIM protein Rare Late onset MYLK2 Myosin light chain kinase 2 Rare Early onset LDB3 LIM binding domain 3 Rare Mainly sigmoidal TCAP Telethonin Rare Typical, variable VCL Vinculin/metavinculin Rare Obstructive midventricular hypertrophy Nonsarcomeric mutations ACTN2 PLN MYOZ2 JPH2 ␣-Actinin 2 Rare Mainly sigmoidal Phospholamban Rare Typical, variable Myozenin 2 Rare Typical Junctophilin 2 Rare Typical 158 Table 2. Circ Cardiovasc Imaging March 2011 Potential Utilities and Pitfalls of Different Imaging Modalities in Diagnosis and Management of HCM Imaging Technique Potential Diagnostic Utility Limitations TTE (M-mode and 2D) Assessment of LV thickness, mitral valve, LVOT gradients, and global and regional LV mechanics ● ● ● ● 3D echocardiography (TTE and TEE) Assessment of mitral valve and papillary muscles, LV volumes, and geometry ● Limited spatial resolution and adequacy of windows (TTE) ● Operator dependent and limited temporal resolution (TTE and TEE) ● Full Doppler capability not available TEE (2D) Exercise echocardiography Assessment of mitral valve and subvalvular pathology and periprocedural assessment Assessment of functional capacity, postexercise LVOT gradients, mitral valve pathology, and blood pressure response to exercise Operator dependent Limited acoustic windows Suboptimal images limit accuracy and reproducibility of measurements Suboptimal assessment of subvalvular apparatus ● Semi-invasive ● Operator dependent ● Limited acoustic windows ● Operator dependent Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 ● Limited availability ● Expensive ● High radiation exposure PET Assessment of coronary flow reserve and microvascular ischemia CMR Unlimited imaging planes to assess anatomy and assessment of LV and papillary muscle morphology, myocardial fibrosis, regional myocardial mechanics, and aortic pathology and flow characteristics ● Limited availability ● Multiple device-related contraindications ● Prognostic value of fibrosis assessment not firmly established Cardiac CT Assessment of LV morphology and coronary artery disease, including myocardial bridging ● Radiation exposure ● Risk of nephrotoxicity due to iodinated contrast TTE indicates transthoracic echocardiography. terization and adds the ability to assess coronary artery anatomy.28 Evaluation of Mitral Valve and Subvalvular Apparatus Mitral valve abnormalities are common in HCM. The most frequent is systolic anterior motion (SAM) of the anterior (less commonly posterior) leaflet of the mitral valve in systole, but other structural abnormalities frequently are seen, including calcification of the mitral valve annulus and elongation of 1 or more cusps of either leaflet. Echocardiographic studies also have demonstrated reduced mobility and length of the posterior mitral leaflet, leading to a shorter coaptation length.29 This results in a longer free segment of the anterior leaflet that is susceptible to drag forces, leading to SAM.30 The direction of MR jet is an important clue in identifying the underlying mechanism31 because an anteriorly/medially directed jet is most likely due to primary posterior leaflet pathology, whereas SAM usually results in a posterior jet. Surface and transesophageal echocardiography (TEE) (including 3D) (online-only Data Supplement Movie 1) may be required to understand mitral valvular and chordal morphology when the direction of the MR jet is not posteriorly directed.32 Compared with normal controls, studies using 3D CMR have demonstrated a higher frequency of papillary muscle abnormalities (anteroapical displacement and hypermobile bifid papillary muscles) in patients with HCM.33,34 These patients have a high prevalence of SAM and elevated LV outflow tract (LVOT) gradients independent of septal thickness. There is increasing recognition that a subset of patients with dynamic LVOT obstruction (LVOTO) have normal thickness or minimal LVH, and the only abnormality noted involves abnormal orientation and hypermobility of papillary muscles (online-only Data Supplement Movie 2).33,35 Evaluation of Myocardial Perfusion The degree of microvascular dysfunction identified by dipyridamole PET is an independent predictor of hard outcomes.36 Following vasodilator challenge, the hyperemic blood flow response is substantially lower in patients with HCM than in controls as assessed by CMR.37 Evaluation of Myocardial Fibrosis Gadolinium-enhanced CMR provides an accurate method for detection of myocardial fibrosis.38 In patients with HCM, myocardial fibrosis is patchy, midmyocardial, and most commonly found in regions of hypertrophy, especially in the interventricular septum at the right ventricular insertion point (Figures 2C and 2D and 3C and 3D). The pattern and amount of fibrosis correlates closely with histopathology39,40 and coronary arteriole dysplasia.40 Fibrosis, defined by CMR, is detectable in 75% to 80% of patients with HCM and correlates with wall thickness and inversely with regional function.41– 43 The long-term clinical significance of fibrosis is uncertain. Extent of fibrosis, particularly in patients aged ⬍40 years, is associated with clinical markers of SCD, whereas in older patients, it is associated with progressive ventricular dysfunction.44 Furthermore, studies have demonstrated an association between degree of myocardial fibrosis and ventricular arrhythmia.42,43,45,46 Emerging data demonstrate incremental prognostic value of myocardial fibrosis assessment in pre- Desai et al Table 3. Recommendations for Different Imaging Modalities in HCM Modality Recommendations TTE 1. Initial detailed morphologic evaluation of patients with suspected HCM, including assessing severity of LVOT obstruction and diastolic assessment 2. Screening of first-degree relatives of the affected proband 3. Periodic follow-up in echocardiography in affected individuals to assess progression, especially with change in symptoms 4. Periodic screening of children of patients with HCM, according to established guideline 5. Assessment of septal perforator anatomy following contrast administration as an adjunct to alcohol septal ablation Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 6. Differential diagnosis of increased LV wall thickness Stress echocardiography 1. Stress echocardiography to assess postexercise LVOT gradient (stress exercise also helps to assess blood pressure response at peak stress) TEE 1. TEE used if TTE is not conclusive 2. TEE for intraoperative guidance of surgery CMR 1. In patients with suspected HCM in the setting of inconclusive echocardiography 2. In patients with apical or lateral variants and suspected apical aneurysms 3. In further evaluation of LV morphology (including papillary muscles), especially in presence of LVOTO and absence of significant LVH 4. Emerging role of delayed postgadolinium imaging for risk stratification of SCD 5. Differential diagnosis of various cardiomyopathies 6. Emerging role in detection of preclinical HCM Cardiac CT 1. In cases of inconclusive echocardiography where CMR is contraindicated 2. Assessment of concomitant coronary artery abnormalities in a symptomatic patient or preoperatively in lieu of invasive angiography Myocardial perfusion scintigraphy 1. Not recommended for routine assessment of coronary flow reserve or myocardial ischemia dicting hard outcomes.47,48 However, long-term prospective studies establishing the association between fibrosis and SCD are needed. Functional Assessment Evaluation of LV Cavity Obstruction Approximately 70% of patients with HCM with asymmetrical septal hypertrophy have evidence of resting or provocable LV Hypertrophic Cardiomyopathy 159 cavity obstruction,49 which can occur at multiple levels and is dynamic, varying with changes in heart rate, afterload, contractility, and intravascular volume.50 LVOTO is associated with worse clinical outcomes, including progression to heart failure and death.49 LVOTO usually is caused by SAM of the mitral valve leaflet. The mechanism is complex but involves narrowing of the LVOT by septal hypertrophy, elongation of mitral leaflets, and anterior displacement of the mitral apparatus and papillary muscles. SAM may be complete, incomplete, or chordal. The location and severity of obstruction is best assessed by pulsed Doppler and continuous-wave Doppler echocardiography, taking care to distinguish the Doppler envelope from mitral regurgitation. Care also should be taken to exclude other causes of LVOTO, including subaortic membrane and accessory mitral valve tissue. Obstruction also occurs at the midcavity level and the ventricular apex. Recently, 3D quantification of LVOT area has been shown to have added utility in the assessment of LVOTO.51 Many patients without outflow obstruction at rest develop it during physiological and pharmacological interventions that reduce LV end-diastolic volume or increase LV contractility (eg, amyl nitrate inhalation, Valsalva maneuver, and administration of intravenous inotropic agents). In patients with exertional symptoms, provocative maneuvers are recommended when the resting LVOT gradient is ⬍30 mm Hg. If the resting gradient is ⬎50 mm Hg, then provocation may not be necessary. Valsalva is the simplest maneuver but has low sensitivity, and pharmacological provocation needs to be done with careful imaging to ensure that the observed Doppler signal is not due to cavity obliteration. However, neither Valsalva nor pharmacological stress reliably reproduce the physiological circumstances in which latent obstruction is likely to occur, and gradients produced during such maneuvers correlate poorly with those induced by exercise. Consequently, exercise stress echocardiography is now the preferred method for provoking gradients. The safety of exercise stress echocardiography has been established previously.52 It provides crucial information about exerciseinduced LVOT gradient, functional capacity, and blood pressure response to exercise.53 In very few patients, lowdose infusions of isoproterenol in conjunction with real-time 2D assessment for SAM and dynamic LVOTO, using TEE is necessary. Identifying and treating provocable obstruction results in significant overall improvement in patients with HCM.54 Phase velocity flow mapping on CMR also can be used to determine the peak LVOT velocity. One study demonstrated the feasibility of identifying patients with obstructive physiology based on the LVOT area measured by CMR.55 However, because of many technical limitations of CMR, Doppler echocardiography remains the method of choice for determining LVOT gradients in clinical practice. Evaluation of Systolic and Diastolic LV Function Multiple mechanisms, including hypertrophy, myocyte disarray, fibrosis, and abnormal calcium metabolism, contribute to diastolic dysfunction. Integrated assessment of several echocardiographic diastolic indices, including pulmonary vein 160 Circ Cardiovasc Imaging March 2011 Figure 2. A 27-year-old man with HCM. A, Two-dimensional echocardiographic image demonstrating asymmetrical basal septal hypertrophy. B, Doppler across the LVOT demonstrating the latepeaking gradient. C, Cine CMR image confirming severe septal hypertrophy. D, Delayed hyperenhancement CMR image demonstrating fibrosis in the hypertrophied septum. Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 flow,56 tissue Doppler imaging, and transmitral inflow, can provide reasonably accurate predictions of filling pressures.56 E/Ea ratio correlates weakly with exercise capacity, and changes in E/Ea ratio have been demonstrated after alcohol septal ablation57,58 and cardiac surgery.58 Septal Ea is an independent predictor of death and ventricular dysrhythmia in children with HCM.59 Although these observations have been made in smaller cohorts, larger cross-sectional studies have failed to significantly correlate Doppler filling patterns, extent of LVH, and invasive indexes of diastolic function.60,61 Figure 3. A 35-year-old man with HCM. A, Two-dimensional echocardiographic image demonstrating severe apical hypertrophy. B, Doppler measurement across the LVOT demonstrating absence of obstruction. C, Two-chamber cine CMR image confirming severe apical hypertrophy. D, Delayed hyperenhancement CMR image demonstrating fibrosis in the hypertrophied myocardium. Desai et al Although assessment of systolic function generally is performed by measuring LV ejection fraction (which can be measured by different imaging techniques), it does not reflect the true systolic function in HCM. CMR studies have demonstrated reduced circumferential shortening in hypertrophied segments that was inversely related to local thickness, with most shortening occurring in early systole.62,63 Another recent study demonstrated reduced LV strain (measured by speckle tracking echocardiography) in patients with HCM, even in the absence of fibrosis. Myocardial fibrosis was associated with further reduction in longitudinal strain.64 Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 Ventricular-Vascular Interactions It was demonstrated recently that LVOT and aortic root are oriented at a steeper angle to the LV in patients with HCM versus normal controls65 and that the angle is independently associated with maximal LVOT gradient. Recently,66 pulsewave velocity using phase-contrast CMR demonstrated stiffer aortas in patients with HCM versus controls and that aortic stiffness was greater in patients with HCM with myocardial fibrosis versus those without. Further work has demonstrated that aortic stiffness is associated with exercise capacity independent of LV morphology, diastolic function, and LVOT gradients.67 Risk Stratification for SCD SCD is a relatively uncommon, but catastrophic complication of HCM, often occurring during mild-moderate exertion.1,2,4,68 –71 A thorough history (including extended family history), physical examination, and imaging evaluation are essential to determine SCD risk. Maximal LV thickness ⱖ3 cm is a major risk factor for SCD.2,70 LVOT gradients ⬎30 mm Hg have been associated with increased risk of SCD, progression to heart failure, arrhythmia, and stroke.49,72 However, the variable nature of LVOT gradients represents a significant limitation to its use as a risk marker of SCD. Other major risk factors include an abnormal blood pressure response during exercise,53 nonsustained ventricular tachycardia, unexplained syncope, and a family history of premature SCD. Previous data from CMR studies have suggested an association between myocardial fibrosis and ventricular arrhythmia.42,43,45,46 Additionally, emerging data demonstrate incremental prognostic value of myocardial fibrosis assessment in predicting hard outcomes.47,48 The role of genetic analysis in risk stratification remains controversial. MYH7-R403Q mutation was associated with increased mortality, whereas a neutral substitution (V606M) was associated with normal survival.73 Early data on the clinical expression from MYBPC mutation indicated a later onset and milder disease74 and that mutations in TNNT2 (troponin T) were associated with less severe hypertrophy and fibrosis but severe disarray and a higher incidence of SCD.75,76 More recently, a larger study has shown an increased risk of composite cardiovascular events with a positive HCM genetic test involving any sarcomeric genes compared with patients with a negative test.77 Additionally, patients with multiple mutations, detected in about 3% to 5% of genotype-positive patients, had a more severe phenotype and increased incidence of SCD.78,79 However, family studies Hypertrophic Cardiomyopathy 161 show that expression of mutations is heterogeneous, even between individuals within families. Further, the majority of diseases causing mutations are rare, making it difficult to determine the SCD risk associated with particular genetic variants in an adequate number of patients. For these reasons, detection of specific mutations is insufficient to implant an implantable cardioverter defibrillator in the absence of other major risk factors. Clinical and Imaging-Based Differential Diagnosis of HCM In routine clinical practice, a systematic approach to the assessment of family pedigree, symptoms, and physical examination in combination with a detailed imaging evaluation and, in some cases, biochemical testing, is central to differential diagnosis of HCM. In some patients, there may be clinical clues that suggest a particular etiology (eg, facial dysmorphia in Noonan syndrome). There also may be clues on the ECG (ventricular preexcitation in storage diseases and mitochondrial disorders). There are few, if any, diseasespecific changes on echocardiography, but in context, a number of features can point to possible diagnoses. For example, concentric hypertrophy tends to be more common in metabolic and storage disorders than in patients with sarcomeric gene mutations. Similarly, biatrial dilatation, restrictive physiology, and an abnormal texture of the interventricular septum (granular sparkling) should suggest amyloidosis. Recently, it has been suggested that septal morphology is preferentially sigmoidal in patients with Z-disc mutations in contrast to myofilament HCM, which generally has a reverse septal curvature.80 Metabolic Cardiomyopathies In ⬍10% of infants and children and an even smaller proportion of adults, HCM is caused by inborn errors of metabolism, neuromuscular disorders, and malformation syndromes. Anderson-Fabry disease is an X-linked lysosomal storage disorder caused by mutations in the ␣-galactosidase A gene that causes progressive accumulation of glycosphingolipid in various organs, including the heart. Cardiac manifestations include progressive wall thickening (Figure 4), valve disease, conduction abnormalities, and arrhythmias. Disease expression typically begins after adolescence.81 Danon disease, an X-linked lysosomal storage disorder caused by mutations in the gene encoding the lysosomeassociated membrane protein 2,82 is characterized by cardiomyopathy, skeletal myopathy, and developmental delay. Other features include Wolff-Parkinson-White syndrome, elevated serum creatine kinase, and retinitis pigmentosa. Males develop symptoms during childhood and adolescence, whereas females develop cardiomyopathy during adulthood. The prognosis is poor, with most patients dying from cardiac failure, although SCD is reported. Pompe disease is an autosomal recessive disorder caused by a deficiency in the lysosomal enzyme acid maltase. The infantile form presents in the first few months, with severe skeletal muscle hypotonia, cardiomegaly, hepatomegaly, and macroglossia, and usually is fatal before 2 years without treatment. Mutations in the gene encoding the ␥2 162 Circ Cardiovasc Imaging March 2011 Figure 4. A 42-year-old woman with Fabry disease. A, Two-dimensional echocardiographic image demonstrating concentric LVH. B, Doppler measurement demonstrating a late-peaking gradient. C, Four-chamber cine CMR image confirming concentric LVH. D, Delayed hyperenhancement CMR image demonstrating inferolateral basal fibrosis. Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 subunit of the AMP-activated protein kinase (PRKAG2) cause a syndrome of HCM, conduction abnormalities, and Wolff-Parkinson-White syndrome.83 Respiratory chain disorders (mitochondrial cardiomyopathies) are caused by sporadic or inherited mutations in nuclear or mitochondrial DNA transmitted as autosomal dominant, recessive, X-linked, or maternal traits.84 These disorders vary in age at onset, symptoms, and range and severity of organ involvement. The phenotype usually is concentric LVH without outflow tract obstruction, often with rapid progression to LV dilatation and heart failure. Noonan syndrome is characterized by short stature, facial dysmorphia, skeletal malformations, and a webbed neck.22 Cardiac involvement is present in up to 90% of patients (pulmonary valve stenosis and HCM). It is inherited as an autosomal dominant trait with variable penetrance and expression. Mutations in PTPN11 gene, encoding the protein tyrosine phosphatase SHP-2, account for ⬇50% of cases, but only 5% to 9% of all individuals with mutations in the PTPN11 gene have HCM.85 LEOPARD (lentigines, ECG abnormalities, ocular hypertelorism, pulmonary stenosis, abnormal genitalia, growth retardation, and deafness) syndrome shares many features with Noonan syndrome and is also caused by mutations in the PTPN11 gene.23 Noonan syndrome and LEOPARD syndrome are examples of neurocardio-facial-cutaneous syndromes. Many are caused by germline mutations in key components of the highly conserved RAS-MAPK cascade.86 Missense PTPN11, KRAS, SOS1, RAF1, MEK1, and BRAF gene mutations have been associated with HCM. CMR and Different Cardiomyopathies Some patterns of myocardial late-gadolinium enhancement on CMR have been reported more frequently in particular cardiomyopathies, for example, midmyocardial posterolateral scarring in the LV (Fabry disease in Figure 4D, glycogen storage disease)87 and diffuse myocardial pattern in cardiac amyloidosis.88 However, these patterns are not specific and must be interpreted in light of the clinical presentation. Hypertensive Heart Disease A common clinical dilemma is the diagnosis of HCM in patients with hypertension. Hypertension typically produces concentric remodeling of the LV rather than asymmetrical hypertrophy. Moderate to severe hypertrophy (ⱖ15 mm) is rare in whites with mild to moderate hypertension, and the presence of a family history of cardiac hypertrophy in a nonhypertensive relative or a positive gene test increases the likelihood of HCM. SAM and LVOTO are recognized but are less common in hypertensive heart disease. Finally, in hypertension but not HCM, treatment with antihypertensives can regress LVH. Recently, deformation imaging has been shown to distinguish between patients with HCM and those with hypertension.89 In one of the earliest efforts to discern the morphology of HCM, the septal contour was divided into reverse curvature, sigmoid shape, apical predominance, and concentric, although observing that the sigmoid shape was more predominant in elderly patients with hypertensive heart disease90 and that this sigmoid shape was less likely to be the result of an underlying sarcomeric mutation.91 Athlete’s Heart Differentiation of physiological hypertrophy from HCM in elite athletes also can pose a problem, but in many cases, analysis of ECG, echocardiography, and CMR facilitates accurate diagnosis (Figure 5).92,93 In athletes’ hearts, LV cavities are typically enlarged, wall thickness is usually ⬍15 mm, and myocardial fibrosis is absent. In contrast, Desai et al Hypertrophic Cardiomyopathy 163 Figure 5. A 17-year-old subject with an athlete’s heart. A, Two-dimensional echocardiographic image demonstrating absence of LVH. B, Doppler measurement demonstrating normal diastology. C, Four-chamber cine CMR image confirming absence of LVH. D, Delayed hyperenhancement CMR image demonstrating no fibrosis. Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 patients with HCM usually have normal or reduced LV dimensions and no cavity dilatation (⬎ 55 mm common in athletes), except with disease progression and systolic dysfunction. In borderline cases, it is reasonable to recommend the cessation of exercise with repeat imaging in order to detect regression of physiological LVH. State-of-the-Art Imaging in Therapeutic Decision Making in HCM In a symptomatic patient with HCM, the goal of imaging is to characterize the mechanism of obstruction and the feasibility of different therapeutic interventions. Although 2D echocardiography (and in some cases TEE) are sufficient, 3D echocardiography and CMR are rapidly emerging as useful adjuncts, especially for assessment of mitral valve and papillary muscle morphology.33 In patients with LVOTO and septal hypertrophy that is not significant (typically ⬍1.8 cm), an extensive myectomy would not be indicated. In such cases, alternate surgical options, such as mitral valve repair/replacement and papillary muscle reorientation,94 need to be considered in addition to a minimyectomy (ⱕ5 mm muscle removal). Figure 6 demonstrates the different potential therapeutic approaches based on septal thickness, mitral valve, and papillary muscle pathology.94 After the decision has been made to proceed with surgery, intraoperative TEE plays an invaluable role95 because it helps to estimate the amount of myocardium that needs to be removed and the length of the anterior mitral leaflet. It is also important after surgery to determine whether residual SAM, LVOTO (measured either directly or with isoproterenol Figure 6. Potential schemata for management of symptomatic patients with significant LVOTO. ASA indicates alcohol septal ablation; MV, mitral valve; PM, papillary muscle; PMR, papillary muscle reorientation. 164 Circ Cardiovasc Imaging March 2011 Figure 7. Suggested schemata for screening of family members in a patient with documented HCM, incorporating genetic testing and clinical evaluation. Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 provocation), and MR are present, which may necessitate further intervention. On the other hand, if the decision is made to proceed with alcohol septal ablation, contrast echocardiography provides essential procedural guidance by identifying the myocardial territory perfused by the target vessel.96 Contrast opacification beyond the area of the basal anteroseptum precludes ethanol injection. CMR also can be used to assess the degree and unpredictable nature of septal regression after alcohol ablation.97 In addition, fibrosis assessment by CMR might have a future role in risk stratification, especially when there is clinical uncertainty about whether to recommend a defibrillator. Screening: Family Members and Asymptomatic Individuals Because HCM is a genetic disorder in many cases, relatives of an index case (proband) can be at risk for developing the disease. The primary aim of family screening, therefore, is to identify relatives who have the same disease as the proband in order to prevent complications and inform life choices. In some cases, assessment of the family also may assist in diagnosing a borderline clinical phenotype. There generally are 2 approaches to family screening. The first is a clinical strategy based on the use of simple noninvasive tests, such as an ECG and echocardiogram. In addition to standard echocardiography, tissue Doppler echocardiography has shown reduced myocardial Doppler velocities in genotype-positive subjects without LVH.98 –100 Tagging by CMR also may have a role in early detection of diastolic dysfunction or morphological changes (prehypertrophic crypts), where LVH has not yet manifested.101,102 In a recent study, high levels of serum C-terminal propeptide of type I procollagen (even before presence of overt fibrosis on CMR) were demonstrated in subjects with HCM mutations without LVH compared with controls.103 If a relative has tests consistent with the suspected clinical diagnosis, then screening can be offered to other first-degree relatives (cascade or stepwise screening). A limitation of this approach is that most genetic forms of HCM have age-related penetrance (ie, the HCM phenotype develops during adolescence and adult life), which means that normal clinical tests cannot exclude future risk of disease development and must be repeated at regular intervals throughout life. An alternative strategy is to identify the causative genetic abnormality in the proband and then offer genetic testing to relatives at risk of developing disease.104,105 The advantage of this approach is that relatives who do not carry the mutation can be spared from further clinical screening, whereas those with the mutation can be monitored and advised appropriately. In practice, both strategies are necessary in particular circumstances. For example, when molecular screening fails to identify a mutation or demonstrates a genetic variant of uncertain significance, clinical evaluation of family members should still be considered. A suggested schema, incorporating genetic and clinical screening, based on the current guidelines and position statements is shown in Figure 7.104,105 There are a couple caveats that need to be considered. First, in a gene-negative first-degree relative of a gene-positive proband (who has multiple risk factors for SCD), it might be prudent to consider imaging in that relative, irrespective of the genotype status. Second, imaging generally is more readily (and in most cases, rapidly) available than genetic testing. It might be prudent to perform cardiac evaluation (including ECG and echocardiography) in all first-degree relatives of the gene-positive proband while waiting for the results of the genetic test. Follow-up imaging in such circumstances could be dictated by the results of the genetic test, as outlined in Figure 7. Conclusions Improved cardiac imaging and advances in our understanding of a genetic basis for HCM have dramatically increased our ability to diagnose and manage patients with HCM. In the future, integration of structural and functional information with detailed Desai et al molecular analysis will provide the basis for new therapeutic interventions that improve quality of life and protect patients and families from disease-related complications. Disclosures None. References Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 1. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH, III, Spirito P, Ten Cate FJ, Wigle ED. American College of Cardiology/European Society of Cardiology clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines J Am Coll Cardiol. 2003; 42:1687–1713. 2. Elliott PM, Poloniecki J, Dickie S, Sharma S, Monserrat L, Varnava A, Mahon NG, McKenna WJ. Sudden death in hypertrophic cardiomyopathy: identification of high risk patients. J Am Coll Cardiol. 2000;36: 2212–2218. 3. Elliott PM, Gimeno JR, Thaman R, Shah J, Ward D, Dickie S, Tome Esteban MT, McKenna WJ. Historical trends in reported survival rates in patients with hypertrophic cardiomyopathy. Heart. 2006;92:785–791. 4. Elliott P, McKenna WJ. Hypertrophic cardiomyopathy. Lancet. 2004; 363:1881–1891. 5. Seidman JG, Seidman C. The genetic basis for cardiomyopathy: from mutation identification to mechanistic paradigms. Cell. 2001;104: 557–567. 6. Marian AJ, Roberts R. The molecular genetic basis for hypertrophic cardiomyopathy. J Mol Cell Cardiol. 2001;33:655– 670. 7. Van Driest SL, Vasile VC, Ommen SR, Will ML, Tajik AJ, Gersh BJ, Ackerman MJ. Myosin binding protein C mutations and compound heterozygosity in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2004;44:1903–1910. 8. Jarcho JA, McKenna W, Pare JA, Solomon SD, Holcombe RF, Dickie S, Levi T, Donis-Keller H, Seidman JG, Seidman CE. Mapping a gene for familial hypertrophic cardiomyopathy to chromosome 14q1. N Engl J Med. 1989;321:1372–1378. 9. Geisterfer-Lowrance AA, Kass S, Tanigawa G, Vosberg HP, McKenna W, Seidman CE, Seidman JG. A molecular basis for familial hypertrophic cardiomyopathy: a beta cardiac myosin heavy chain gene missense mutation. Cell. 1990;62:999 –1006. 10. Poetter K, Jiang H, Hassanzadeh S, Master SR, Chang A, Dalakas MC, Rayment I, Sellers JR, Fananapazir L, Epstein ND. Mutations in either the essential or regulatory light chains of myosin are associated with a rare myopathy in human heart and skeletal muscle. Nat Genet. 1996; 13:63– 69. 11. Watkins H, Conner D, Thierfelder L, Jarcho JA, MacRae C, McKenna WJ, Maron BJ, Seidman JG, Seidman CE. Mutations in the cardiac myosin binding protein-C gene on chromosome 11 cause familial hypertrophic cardiomyopathy. Nat Genet. 1995;11:434 – 437. 12. Thierfelder L, Watkins H, MacRae C, Lamas R, McKenna W, Vosberg HP, Seidman JG, Seidman CE. Alpha-tropomyosin and cardiac troponin T mutations cause familial hypertrophic cardiomyopathy: a disease of the sarcomere. Cell. 1994;77:701–712. 13. Kimura A, Harada H, Park JE, Nishi H, Satoh M, Takahashi M, Hiroi S, Sasaoka T, Ohbuchi N, Nakamura T, Koyanagi T, Hwang TH, Choo JA, Chung KS, Hasegawa A, Nagai R, Okazaki O, Nakamura H, Matsuzaki M, Sakamoto T, Toshima H, Koga Y, Imaizumi T, Sasazuki T. Mutations in the cardiac troponin I gene associated with hypertrophic cardiomyopathy. Nat Genet. 1997;16:379 –382. 14. Landstrom AP, Parvatiyar MS, Pinto JR, Marquardt ML, Bos JM, Tester DJ, Ommen SR, Potter JD, Ackerman MJ. Molecular and functional characterization of novel hypertrophic cardiomyopathy susceptibility mutations in TNNC1-encoded troponin C. J Mol Cell Cardiol. 2008;45: 281–288. 15. Mogensen J, Klausen IC, Pedersen AK, Egeblad H, Bross P, Kruse TA, Gregersen N, Hansen PS, Baandrup U, Borglum AD. Alpha-cardiac actin is a novel disease gene in familial hypertrophic cardiomyopathy. J Clin Invest. 1999;103:R39 – 43. 16. Bos JM, Towbin JA, Ackerman MJ. Diagnostic, prognostic, and therapeutic implications of genetic testing for hypertrophic cardiomyopathy. J Am Coll Cardiol. 2009;54:201–211. Hypertrophic Cardiomyopathy 165 17. Blanchard E, Seidman C, Seidman JG, LeWinter M, Maughan D. Altered crossbridge kinetics in the alphaMHC403/⫹ mouse model of familial hypertrophic cardiomyopathy. Circ Res. 1999;84:475– 483. 18. Miller T, Szczesna D, Housmans PR, Zhao J, de Freitas F, Gomes AV, Culbreath L, McCue J, Wang Y, Xu Y, Kerrick WG, Potter JD. Abnormal contractile function in transgenic mice expressing a familial hypertrophic cardiomyopathy-linked troponin T (I79N) mutation. J Biol Chem. 2001;276:3743–3755. 19. Gerull B, Gramlich M, Atherton J, McNabb M, Trombitas K, SasseKlaassen S, Seidman JG, Seidman C, Granzier H, Labeit S, Frenneaux M, Thierfelder L. Mutations of TTN, encoding the giant muscle filament titin, cause familial dilated cardiomyopathy. Nat Genet. 2002;30: 201–204. 20. Geier C, Perrot A, Ozcelik C, Binner P, Counsell D, Hoffmann K, Pilz B, Martiniak Y, Gehmlich K, van der Ven PF, Furst DO, Vornwald A, von Hodenberg E, Nurnberg P, Scheffold T, Dietz R, Osterziel KJ. Mutations in the human muscle LIM protein gene in families with hypertrophic cardiomyopathy. Circulation. 2003;107:1390 –1395. 21. Palumbo V, Segat L, Padovan L, Amoroso A, Trimarco B, Izzo R, Lembo G, Zagrosek VR, Knoll R, Brancaccio M, Tarone G, Crovella S. Melusin gene (ITGB1BP2) nucleotide variations study in hypertensive and cardiopathic patients. BMC Med Genet. 2009;10:140. 22. Wigle ED, Sasson Z, Henderson MA, Ruddy TD, Fulop J, Rakowski H, Williams WG. Hypertrophic cardiomyopathy. The importance of the site and the extent of hypertrophy. A review. Prog Cardiovasc Dis. 1985; 28:1– 83. 23. Bicudo LS, Tsutsui JM, Shiozaki A, Rochitte CE, Arteaga E, Mady C, Ramires JA, Mathias W Jr. Value of real time three-dimensional echocardiography in patients with hypertrophic cardiomyopathy: comparison with two-dimensional echocardiography and magnetic resonance imaging. Echocardiography. 2008;25:717–726. 24. Rickers C, Wilke NM, Jerosch-Herold M, Casey SA, Panse P, Panse N, Weil J, Zenovich AG, Maron BJ. Utility of cardiac magnetic resonance imaging in the diagnosis of hypertrophic cardiomyopathy. Circulation. 2005;112:855– 861. 25. Moon JC, Fisher NG, McKenna WJ, Pennell DJ. Detection of apical hypertrophic cardiomyopathy by cardiovascular magnetic resonance in patients with non-diagnostic echocardiography. Heart. 2004;90: 645– 649. 26. Olivotto I, Maron MS, Autore C, Lesser JR, Rega L, Casolo G, De Santis M, Quarta G, Nistri S, Cecchi F, Salton CJ, Udelson JE, Manning WJ, Maron BJ. Assessment and significance of left ventricular mass by cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2008;52:559 –566. 27. Maron MS, Finley JJ, Bos JM, Hauser TH, Manning WJ, Haas TS, Lesser JR, Udelson JE, Ackerman MJ, Maron BJ. Prevalence, clinical significance, and natural history of left ventricular apical aneurysms in hypertrophic cardiomyopathy. Circulation. 2008;118:1541–1549. 28. Hendel RC, Patel MR, Kramer CM, Poon M, Hendel RC, Carr JC, Gerstad NA, Gillam LD, Hodgson JM, Kim RJ, Kramer CM, Lesser JR, Martin ET, Messer JV, Redberg RF, Rubin GD, Rumsfeld JS, Taylor AJ, Weigold WG, Woodard PK, Brindis RG, Hendel RC, Douglas PS, Peterson ED, Wolk MJ, Allen JM, Patel MR. ACCF/ACR/SCCT/ SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006;48:1475–1497. 29. Schwammenthal E, Nakatani S, He S, Hopmeyer J, Sagie A, Weyman AE, Lever HM, Yoganathan AP, Thomas JD, Levine RA. Mechanism of mitral regurgitation in hypertrophic cardiomyopathy: mismatch of posterior to anterior leaflet length and mobility. Circulation. 1998;98: 856 – 865. 30. Flores-Ramirez R, Lakkis NM, Middleton KJ, Killip D, Spencer WH III, Nagueh SF. Echocardiographic insights into the mechanisms of relief of left ventricular outflow tract obstruction after nonsurgical septal reduction therapy in patients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol. 2001;37:208 –214. 31. Yu EH, Omran AS, Wigle ED, Williams WG, Siu SC, Rakowski H. Mitral regurgitation in hypertrophic obstructive cardiomyopathy: rela- 166 32. 33. 34. 35. 36. Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. Circ Cardiovasc Imaging March 2011 tionship to obstruction and relief with myectomy. J Am Coll Cardiol. 2000;36:2219 –2225. Sugeng L, Coon P, Weinert L, Jolly N, Lammertin G, Bednarz JE, Thiele K, Lang RM. Use of real-time 3-dimensional transthoracic echocardiography in the evaluation of mitral valve disease. J Am Soc Echocardiogr. 2006;19:413– 421. Kwon DH, Setser RM, Thamilarasan M, Popovic ZV, Smedira NG, Schoenhagen P, Garcia MJ, Lever HM, Desai MY. Abnormal papillary muscle morphology is independently associated with increased left ventricular outflow tract obstruction in hypertrophic cardiomyopathy. Heart. 2008;94:1295–1301. Harrigan CJ, Appelbaum E, Maron BJ, Buros JL, Gibson CM, Lesser JR, Udelson JE, Manning WJ, Maron MS. Significance of papillary muscle abnormalities identified by cardiovascular magnetic resonance in hypertrophic cardiomyopathy. Am J Cardiol. 2008;101:668 – 673. Austin BA, Kwon DH, Smedira NG, Thamilarasan M, Lever HM, Desai MY. Abnormally thickened papillary muscle resulting in dynamic left ventricular outflow tract obstruction: an unusual presentation of hypertrophic cardiomyopathy. J Am Soc Echocardiogr. 2009;22:105.e5– e6. Cecchi F, Olivotto I, Gistri R, Lorenzoni R, Chiriatti G, Camici PG. Coronary microvascular dysfunction and prognosis in hypertrophic cardiomyopathy. N Engl J Med. 2003;349:1027–1035. Petersen SE, Jerosch-Herold M, Hudsmith LE, Robson MD, Francis JM, Doll HA, Selvanayagam JB, Neubauer S, Watkins H. Evidence for microvascular dysfunction in hypertrophic cardiomyopathy: new insights from multiparametric magnetic resonance imaging. Circulation. 2007;115:2418 –2425. Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM, Finn JP, Judd RM. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001;218:215–223. Moon JC, Sheppard M, Reed E, Lee P, Elliott PM, Pennell DJ. The histological basis of late gadolinium enhancement cardiovascular magnetic resonance in a patient with Anderson-Fabry disease. J Cardiovasc Magn Reson. 2006;8:479 – 482. Kwon DH, Smedira NG, Rodriguez ER, Tan C, Setser R, Thamilarasan M, Lytle BW, Lever HM, Desai MY. Cardiac magnetic resonance detection of myocardial scarring in hypertrophic cardiomyopathy: correlation with histopathology and prevalence of ventricular tachycardia. J Am Coll Cardiol. 2009;54:242–249. Choudhury L, Mahrholdt H, Wagner A, Choi KM, Elliott MD, Klocke FJ, Bonow RO, Judd RM, Kim RJ. Myocardial scarring in asymptomatic or mildly symptomatic patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002;40:2156 –2164. Teraoka K, Hirano M, Ookubo H, Sasaki K, Katsuyama H, Amino M, Abe Y, Yamashina A. Delayed contrast enhancement of MRI in hypertrophic cardiomyopathy. Magn Reson Imaging. 2004;22:155–161. Kwon DH, Setser RM, Popovic ZB, Thamilarasan M, Sola S, Schoenhagen P, Garcia MJ, Flamm SD, Lever HM, Desai MY. Association of myocardial fibrosis, electrocardiography and ventricular tachyarrhythmia in hypertrophic cardiomyopathy: a delayed contrast enhanced MRI study. Int J Cardiovasc Imaging. 2008;24:617– 625. Moon JC, McKenna WJ, McCrohon JA, Elliott PM, Smith GC, Pennell DJ. Toward clinical risk assessment in hypertrophic cardiomyopathy with gadolinium cardiovascular magnetic resonance. J Am Coll Cardiol. 2003;41:1561–1567. Adabag AS, Maron BJ, Appelbaum E, Harrigan CJ, Buros JL, Gibson CM, Lesser JR, Hanna CA, Udelson JE, Manning WJ, Maron MS. Occurrence and frequency of arrhythmias in hypertrophic cardiomyopathy in relation to delayed enhancement on cardiovascular magnetic resonance. J Am Coll Cardiol. 2008;51:1369 –1374. Rubinshtein R, Glockner JF, Ommen SR, Araoz PA, Ackerman MJ, Sorajja P, Bos JM, Tajik AJ, Valeti US, Nishimura RA, Gersh BJ. Characteristics and clinical significance of late gadolinium enhancement by contrast-enhanced magnetic resonance imaging in patients with hypertrophic cardiomyopathy. Circ Heart Fail. 2009;3:51–58. O’Hanlon R, Grasso A, Roughton M, Moon JC, Clark S, Wage R, Webb J, Kulkarni M, Dawson D, Sulaibeekh L, Chandrasekaran B, Bucciarelli-Ducci C, Pasquale F, Cowie MR, McKenna WJ, Sheppard MN, Elliott PM, Pennell DJ, Prasad SK. Prognostic significance of myocardial fibrosis in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2010;56:867– 874. Bruder O, Wagner A, Jensen CJ, Schneider S, Ong P, Kispert EM, Nassenstein K, Schlosser T, Sabin GV, Sechtem U, Mahrholdt H. Myocardial scar visualized by cardiovascular magnetic resonance 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. 62. 63. imaging predicts major adverse events in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2010;56:875– 887. Maron MS, Olivotto I, Betocchi S, Casey SA, Lesser JR, Losi MA, Cecchi F, Maron BJ. Effect of left ventricular outflow tract obstruction on clinical outcome in hypertrophic cardiomyopathy. N Engl J Med. 2003;348:295–303. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH III, Spirito P, Ten Cate FJ, Wigle ED. American College of Cardiology/European Society of Cardiology Clinical expert consensus document on hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines. Eur Heart J. 2003;24: 1965–1991. Fukuda S, Lever HM, Stewart WJ, Tran H, Song JM, Shin MS, Greenberg NL, Wada N, Matsumura Y, Toyono M, Smedira NG, Thomas JD, Shiota T. Diagnostic value of left ventricular outflow area in patients with hypertrophic cardiomyopathy: a real-time threedimensional echocardiographic study. J Am Soc Echocardiogr. 2008; 21:789 –795. Drinko JK, Nash PJ, Lever HM, Asher CR. Safety of stress testing in patients with hypertrophic cardiomyopathy. Am J Cardiol. 2004;93: 1443–1444, A12. Olivotto I, Maron BJ, Montereggi A, Mazzuoli F, Dolara A, Cecchi F. Prognostic value of systemic blood pressure response during exercise in a community-based patient population with hypertrophic cardiomyopathy. J Am Coll Cardiol. 1999;33:2044 –2051. Lakkis N, Plana JC, Nagueh S, Killip D, Roberts R, Spencer WH III. Efficacy of nonsurgical septal reduction therapy in symptomatic patients with obstructive hypertrophic cardiomyopathy and provocable gradients. Am J Cardiol. 2001;88:583–586. Schulz-Menger J, Abdel-Aty H, Busjahn A, Wassmuth R, Pilz B, Dietz R, Friedrich MG. Left ventricular outflow tract planimetry by cardiovascular magnetic resonance differentiates obstructive from nonobstructive hypertrophic cardiomyopathy. J Cardiovasc Magn Reson. 2006;8:741–746. Nagueh SF, Lakkis NM, Middleton KJ, Spencer WH III, Zoghbi WA, Quinones MA. Doppler estimation of left ventricular filling pressures in patients with hypertrophic cardiomyopathy. Circulation. 1999;99: 254 –261. Nagueh SF, Lakkis NM, Middleton KJ, Killip D, Zoghbi WA, Quinones MA, Spencer WH III. Changes in left ventricular filling and left atrial function six months after nonsurgical septal reduction therapy for hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol. 1999;34: 1123–1128. Sitges M, Shiota T, Lever HM, Qin JX, Bauer F, Drinko JK, Agler DA, Martin MG, Greenberg NL, Smedira NG, Lytle BW, Tuzcu EM, Garcia MJ, Thomas JD. Comparison of left ventricular diastolic function in obstructive hypertrophic cardiomyopathy in patients undergoing percutaneous septal alcohol ablation versus surgical myotomy/myectomy. Am J Cardiol. 2003;91:817– 821. McMahon CJ, Nagueh SF, Pignatelli RH, Denfield SW, Dreyer WJ, Price JF, Clunie S, Bezold LI, Hays AL, Towbin JA, Eidem BW. Characterization of left ventricular diastolic function by tissue Doppler imaging and clinical status in children with hypertrophic cardiomyopathy. Circulation. 2004;109:1756 –1762. Nishimura RA, Appleton CP, Redfield MM, Ilstrup DM, Holmes DR Jr, Tajik AJ. Noninvasive Doppler echocardiographic evaluation of left ventricular filling pressures in patients with cardiomyopathies: a simultaneous Doppler echocardiographic and cardiac catheterization study. J Am Coll Cardiol. 1996;28:1226 –1233. Geske JB, Sorajja P, Nishimura RA, Ommen SR. Evaluation of left ventricular filling pressures by Doppler echocardiography in patients with hypertrophic cardiomyopathy: correlation with direct left atrial pressure measurement at cardiac catheterization. Circulation. 2007;116: 2702–2708. Dong SJ, MacGregor JH, Crawley AP, McVeigh E, Belenkie I, Smith ER, Tyberg JV, Beyar R. Left ventricular wall thickness and regional systolic function in patients with hypertrophic cardiomyopathy. A threedimensional tagged magnetic resonance imaging study. Circulation. 1994;90:1200 –1209. Kramer CM, Reichek N, Ferrari VA, Theobald T, Dawson J, Axel L. Regional heterogeneity of function in hypertrophic cardiomyopathy. Circulation. 1994;90:186 –194. Desai et al Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 64. Popovic ZB, Kwon DH, Mishra M, Buakhamsri A, Greenberg NL, Thamilarasan M, Flamm SD, Thomas JD, Lever HM, Desai MY. Association between regional ventricular function and myocardial fibrosis in hypertrophic cardiomyopathy assessed by speckle tracking echocardiography and delayed hyperenhancement magnetic resonance imaging. J Am Soc Echocardiogr. 2008;21:1299 –1305. 65. Kwon DH, Smedira NG, Popovic ZB, Lytle BW, Setser R, Thamilarasan M, Schoenhagen P, Flamm SD, Lever HM, Desai MY. Steep left ventricle to aortic root angle and hypertrophic obstructive cardiomyopathy: study of a novel association using 3-dimensional multi-modality imaging. Heart. 2009;95:1784 –1791. 66. Boonyasirinant T, Rajiah P, Setser RM, Lieber ML, Lever HM, Desai MY, Flamm SD. Aortic stiffness is increased in hypertrophic cardiomyopathy with myocardial fibrosis: novel insights in vascular function from magnetic resonance imaging. J Am Coll Cardiol. 2009;54: 255–262. 67. Austin BA, Popovic Z, Kwon D, Thamilarasan M, Boonyasirinant T, Flamm SD, Lever H, Desai MY. Aortic stiffness independently predicts exercise capacity in hypertrophic cardiomyopathy: a multimodality imaging study. Heart. 2010;96:1303–1310. 68. Spirito P. The management of hypertrophic cardiomyopathy. N Engl J Med. 1997;336:775–785. 69. Elliott P. Relation between the severity of left ventricular hypertrophy and prognosis in patients with hypertrophic cardiomyopathy. Lancet. 2001;357:420 – 424. 70. Spirito P, Bellone P, Harris KM, Bernabo P, Bruzzi P, Maron BJ. Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyopathy. N Engl J Med. 2000;342:1778 –1785. 71. Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002;287:1308 –1320. 72. Kofflard MJ, Ten Cate FJ, van der Lee C, van Domburg RT. Hypertrophic cardiomyopathy in a large community-based population: clinical outcome and identification of risk factors for sudden cardiac death and clinical deterioration. J Am Coll Cardiol. 2003;41:987–993. 73. Watkins H, Rosenzweig A, Hwang DS, Levi T, McKenna W, Seidman CE, Seidman JG. Characteristics and prognostic implications of myosin missense mutations in familial hypertrophic cardiomyopathy. N Engl J Med. 1992;326:1108 –1114. 74. Niimura H, Bachinski LL, Sangwatanaroj S, Watkins H, Chudley AE, McKenna W, Kristinsson A, Roberts R, Sole M, Maron BJ, Seidman JG, Seidman CE. Mutations in the gene for cardiac myosin-binding protein C and late-onset familial hypertrophic cardiomyopathy. N Engl J Med. 1998;338:1248 –1257. 75. Moolman JC, Corfield VA, Posen B, Ngumbela K, Seidman C, Brink PA, Watkins H. Sudden death due to troponin T mutations. J Am Coll Cardiol. 1997;29:549 –555. 76. Watkins H, McKenna WJ, Thierfelder L, Suk HJ, Anan R, O’Donoghue A, Spirito P, Matsumori A, Moravec CS, Seidman JG, Seidman CE. Mutations in the genes for cardiac troponin T and alpha-tropomyosin in hypertrophic cardiomyopathy. N Engl J Med. 1995;332:1058 –1064. 77. Olivotto I, Girolami F, Ackerman MJ, Nistri S, Bos JM, Zachara E, Ommen SR, Theis JL, Vaubel RA, Re F, Armentano C, Poggesi C, Torricelli F, Cecchi F. Myofilament protein gene mutation screening and outcome of patients with hypertrophic cardiomyopathy. Mayo Clin Proc. 2008;83:630 – 638. 78. Ingles J, Doolan A, Chiu C, Seidman J, Seidman C, Semsarian C. Compound and double mutations in patients with hypertrophic cardiomyopathy: implications for genetic testing and counselling. J Med Genet. 2005;42:e59. 79. Ho CY, Lever HM, DeSanctis R, Farver CF, Seidman JG, Seidman CE. Homozygous mutation in cardiac troponin T: implications for hypertrophic cardiomyopathy. Circulation. 2000;102:1950 –1955. 80. Theis JL, Bos JM, Bartleson VB, Will ML, Binder J, Vatta M, Towbin JA, Gersh BJ, Ommen SR, Ackerman MJ. Echocardiographicdetermined septal morphology in Z-disc hypertrophic cardiomyopathy. Biochem Biophys Res Commun. 2006;351:896 –902. 81. Linhart A, Kampmann C, Zamorano JL, Sunder-Plassmann G, Beck M, Mehta A, Elliott PM. Cardiac manifestations of Anderson-Fabry disease: results from the international Fabry outcome survey. Eur Heart J. 2007;28:1228 –1235. 82. Arad M, Benson DW, Perez-Atayde AR, McKenna WJ, Sparks EA, Kanter RJ, McGarry K, Seidman JG, Seidman CE. Constitutively active AMP kinase mutations cause glycogen storage disease mimicking hypertrophic cardiomyopathy. J Clin Invest. 2002;109:357–362. Hypertrophic Cardiomyopathy 167 83. Blair E, Redwood C, Ashrafian H, Oliveira M, Broxholme J, Kerr B, Salmon A, Ostman-Smith I, Watkins H. Mutations in the gamma(2) subunit of AMP-activated protein kinase cause familial hypertrophic cardiomyopathy: evidence for the central role of energy compromise in disease pathogenesis. Hum Mol Genet. 2001;10:1215–1220. 84. DiMauro S, Schon EA. Mitochondrial respiratory-chain diseases. N Engl J Med. 2003;348:2656 –2668. 85. Chen B, Bronson RT, Klaman LD, Hampton TG, Wang JF, Green PJ, Magnuson T, Douglas PS, Morgan JP, Neel BG. Mice mutant for Egfr and Shp2 have defective cardiac semilunar valvulogenesis. Nat Genet. 2000;24:296 –299. 86. Tidyman WE, Rauen KA. The RASopathies: developmental syndromes of Ras/MAPK pathway dysregulation. Curr Opin Genet Dev. 2009;19: 230 –236. 87. Mahrholdt H, Wagner A, Judd RM, Sechtem U, Kim RJ. Delayed enhancement cardiovascular magnetic resonance assessment of nonischaemic cardiomyopathies. Eur Heart J. 2005;26:1461–1474. 88. Austin BA, Tang WH, Rodriguez ER, Tan C, Flamm SD, Taylor DO, Starling RC, Desai MY. Delayed hyper-enhancement magnetic resonance imaging provides incremental diagnostic and prognostic utility in suspected cardiac amyloidosis. J Am Coll Cardiol Cardiovasc Imaging. 2009;2:1369 –1377. 89. Kato TS, Noda A, Izawa H, Yamada A, Obata K, Nagata K, Iwase M, Murohara T, Yokota M. Discrimination of nonobstructive hypertrophic cardiomyopathy from hypertensive left ventricular hypertrophy on the basis of strain rate imaging by tissue Doppler ultrasonography. Circulation. 2004;110:3808–3814. 90. Lever HM, Karam RF, Currie PJ, Healy BP. Hypertrophic cardiomyopathy in the elderly. Distinctions from the young based on cardiac shape. Circulation. 1989;79:580 –589. 91. Binder J, Ommen SR, Gersh BJ, Van Driest SL, Tajik AJ, Nishimura RA, Ackerman MJ. Echocardiography-guided genetic testing in hypertrophic cardiomyopathy: septal morphological features predict the presence of myofilament mutations. Mayo Clin Proc. 2006;81:459 – 467. 92. Spirito P, Pelliccia A, Proschan MA, Granata M, Spataro A, Bellone P, Caselli G, Biffi A, Vecchio C, Maron BJ. Morphology of the “athlete’s heart” assessed by echocardiography in 947 elite athletes representing 27 sports. Am J Cardiol. 1994;74:802– 806. 93. Scharhag J, Urhausen A, Schneider G, Rochette V, Kramann B, Kindermann W. [Left ventricular mass in endurance-athletes with athlete’s heart and untrained subjects— comparison between different echocardiographic methods and MRI]. Z Kardiol. 2003;92:309 –318. 94. Kwon DH, Smedira NG, Thamilarasan M, Lytle BW, Lever H, Desai MY. Characteristics and surgical outcomes of symptomatic patients with hypertrophic cardiomyopathy with abnormal papillary muscle morphology undergoing papillary muscle reorientation. J Thorac Cardiovasc Surg. 2010;140:317–324. 95. Ommen SR, Park SH, Click RL, Freeman WK, Schaff HV, Tajik AJ. Impact of intraoperative transesophageal echocardiography in the surgical management of hypertrophic cardiomyopathy. Am J Cardiol. 2002;90:1022–1024. 96. Nagueh SF, Lakkis NM, He ZX, Middleton KJ, Killip D, Zoghbi WA, Quinones MA, Roberts R, Verani MS, Kleiman NS, Spencer WH III. Role of myocardial contrast echocardiography during nonsurgical septal reduction therapy for hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol. 1998;32:225–229. 97. Valeti US, Nishimura RA, Holmes DR, Araoz PA, Glockner JF, Breen JF, Ommen SR, Gersh BJ, Tajik AJ, Rihal CS, Schaff HV, Maron BJ. Comparison of surgical septal myectomy and alcohol septal ablation with cardiac magnetic resonance imaging in patients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol. 2007;49:350 –357. 98. Nagueh SF, Bachinski LL, Meyer D, Hill R, Zoghbi WA, Tam JW, Quinones MA, Roberts R, Marian AJ. Tissue Doppler imaging consistently detects myocardial abnormalities in patients with hypertrophic cardiomyopathy and provides a novel means for an early diagnosis before and independently of hypertrophy. Circulation. 2001;104: 128 –130. 99. Ho CY, Sweitzer NK, McDonough B, Maron BJ, Casey SA, Seidman JG, Seidman CE, Solomon SD. Assessment of diastolic function with Doppler tissue imaging to predict genotype in preclinical hypertrophic cardiomyopathy. Circulation. 2002;105:2992–2997. 100. Nagueh SF, McFalls J, Meyer D, Hill R, Zoghbi WA, Tam JW, Quinones MA, Roberts R, Marian AJ. Tissue Doppler imaging predicts the development of hypertrophic cardiomyopathy in subjects with subclinical disease. Circulation. 2003;108:395–398. 168 Circ Cardiovasc Imaging March 2011 101. Ennis DB, Epstein FH, Kellman P, Fananapazir L, McVeigh ER, Arai AE. Assessment of regional systolic and diastolic dysfunction in familial hypertrophic cardiomyopathy using MR tagging. Magn Reson Med. 2003;50:638 – 642. 102. Germans T, Wilde AA, van Echteld CJ, Kamp O, Pinto YM, van Rossum AC. Structural abnormalities of the left ventricle in hypertrophic cardiomyopathy mutation carriers detectable before the development of hypertrophy. Neth Heart J. 2007;15:161–163. 103. Ho CY, Lopez B, Coelho-Filho OR, Lakdawala NK, Cirino AL, Jarolim P, Kwong R, Gonzalez A, Colan SD, Seidman J, Dietz J, Seidman C. Myocardial fibrosis as an early manifestation of hypertrophic cardiomyopathy. N Engl J Med. 2010:552–563. 104. Hershberger RE, Lindenfeld J, Mestroni L, Seidman CE, Taylor MR, Towbin JA. Genetic evaluation of cardiomyopathy—a Heart Failure Society of America practice guideline. J Card Fail. 2009;15:83–97. 105. Charron P, Arad M, Arbustini E, Basso C, Bilinska Z, Elliott P, Helio T, Keren A, McKenna W, Monserrat L, Seggewiss H, van Langen I, Tavazzi L. Genetic counselling and testing in cardiomyopathies: a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2010;31: 2715–2726. KEY WORDS: cardiomyopathy 䡲 hypertrophy 䡲 imaging 䡲 genetics Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 Imaging Phenotype Versus Genotype in Hypertrophic Cardiomyopathy Milind Y. Desai, Steve R. Ommen, William J. McKenna, Harry M. Lever and Perry M. Elliott Downloaded from http://circimaging.ahajournals.org/ by guest on May 13, 2017 Circ Cardiovasc Imaging. 2011;4:156-168 doi: 10.1161/CIRCIMAGING.110.957936 Circulation: Cardiovascular Imaging is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2011 American Heart Association, Inc. All rights reserved. Print ISSN: 1941-9651. Online ISSN: 1942-0080 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circimaging.ahajournals.org/content/4/2/156 Data Supplement (unedited) at: http://circimaging.ahajournals.org/content/suppl/2011/03/17/4.2.156.DC1 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation: Cardiovascular Imaging can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation: Cardiovascular Imaging is online at: http://circimaging.ahajournals.org//subscriptions/