Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
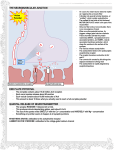
Human Health and Disease Lecture 3 The series of steps involved in signal transduction pathway 2 General elements of GPCRs Most abundant class of receptors Found in organisms from yeast to man 1. A receptor with 7 membrane-spanning domains 2. A coupled trimeric G protein 3. A membrane bound effector protein 4. Feedback regulation and desensitization of the signalling pathway 5. A 2nd messenger present in many GPCRs. Second messengers are molecules that relay signals from receptors on the cell surface to target molecules inside the cell, in the cytoplasm or nucleus. These components of GPCRs can be mixed and matched to achieve an astonishing number of different pathways GPCR pathways usually have short term effects in the cells Allow the cells to respond rapidly to a variety of signals like environmental stimuli (light) or hormonal stimuli (epinephrine) General features GPCRs have same orientation in the membrane , 7 transmembrane alphahelical regions, 4 extra cellular segments, 4 cytosolic segments G Protein •Guanine nucleotide-binding proteins, family of proteins involved in transmitting chemical signals originating from outside a cell into the inside of the cell. •G proteins function as molecular switches. Their activity is regulated by their ability to bind to and hydrolyze guanosine triphosphate (GTP) to guanosine diphosphate (GDP). •When they bind GTP, they are 'on', and, when they bind GDP, they are 'off'. •G proteins belong to the larger group of enzymes called GTPases. Gβ§ Involvement of G- Protein in Cell Signaling Opening of ion channels What do we know about ion channels? ‘’Ion channels are responsible for the transmembrane flux of ions that lead to the generation of action potentials. There is a stunning array of different types of channels that can be activated by different stimuli. Biophysical studies have begun to reveal the fundamental mechanisms responsible for the selectivity of a channel for one ion over another. And, both physicians and scientists are learning much about the role of ion channels in normal physiology from the discovery of human mutations. Nevertheless, the functions of many ion channels remain unknown, and their structure-function relationships are still undefined. Despite being very small structures, ion channels have large functions; they control the beating of a heart, the perception of sound or sight, or storage of a memory. Ultimately, these biological processes depend not on a single ion channel, but on all the ion channels in a cell and tissue network functioning in a coordinated manner. How this happens will continue to capture our imagination and attention for decades to come.’’ http://www.nature.com/scitable/topicpage/ion-channels-and-excitablecells-14406097 Signal amplification occurs in many signaling pathways Receptors are low abundance proteins The binding of few signaling molecules to available receptors require production of tens of thousands or even millions of second messenger or activated enzyme molecules per cell. Substantial signal amplification must occur in order for a hormone signal to induce a significant cellular response. For example, a single epinephrine-GPCR complex causes conversion of up to 100 inactive Gαs molecules to the active form before epinephrine dissociate from the receptor. •Binding of a single epinephrine molecule to the receptor induces synthesis of a large number of cAMP molecules, first level of amplification. •2 molecules of cAMP activate 1 molecule of protein kinase A. •Each activated PKA phosphorylates and activates multiple product molecules, second level of activation. How does the signaling terminate? The Gα-GTP state is short-lived because the bound GTP is hydrolyzed to GDP in minutes. The GPCR signal-transduction system contains a built-in feedback mechanism that ensures the effector protein becomes activated only for a few seconds or minutes following receptor activation. Gα the switches back to Gα-GDP state blocking any further activation of effector proteins. The resulting Gα-GDP reassociates with Gβγ and the complex becomes ready to interact with an activated receptor to stop the process. Acetylcholine induces different responses in different target cells Cardiac Cycle LA: Left Atrium RA: Right Atrium LV: Left ventricle RV: Right Ventricle Ao: Aorta SVC: Superior vena cana IVC: Inferior vena cava PA: Pulmonary Artry 1. Atrial Systole 2. Ventricle Diastole 3. Ventricle Systole Diastole represents the period of time when the ventricles are relaxed (not contracting). Systole represents the time during which the left and right ventricles contract and eject blood into the aorta and pulmonary artery, respectively. http://www.cvphysiology.com/Heart%20Disease/HD002.htm Action Potential of Heart Muscles An action potential is the transient, rapid rise and fall of the membrane voltage. The voltage difference across the cell membrane is about -70mV at rest, and there is a greater concentration of Na outside the cell than inside. So, when the cell reaches a certain threshold potential, the Na channels open, and Na rushes into the cell resulting in a potential of about +30mV. The cell is said to be "depolarized.“ Then, K channels open, and since the concentration of K is higher inside the cell, K rushes out. This brings the polarity back down to -70mV, and then a little bit past it to -90mV. At this point the cell is said to be "hyperpolarized." The Na/K pump then gradually restores the potential back to the resting -70mV, and the cell can then transmit another action potential. If the cell's potassium channels do not open, the cell will be constantly depolarized, and therefore be unable to conduct an action potential. Decreased release of neurotransmitter acetylcholine contributes to heart failure It reduces the cardiomyocytes demand of oxygen rendering them more resistant to the reduced oxygen supply which may result from the obstruction of coronary arteries by atherosclerosis. The area of experimental infarction was reduced by ~50% in animals in which cardiomyocytes acetylcholine synthesis was largely increased by genetic manipulations. It controls growth of cardiomyocytes. They increase their volume (hypertrophy) in animals in which acetylcholine synthesis has been eliminated. Cardiomyocytes are hypertrophied when the heart is mechanicaly overloaded for example in arterial hypertension. Cardiomyocytes of animals devoid of acetylcholine synthesis are more susceptible to the overload. Hypertrophy of cardiomyocytes may lead to the heart failure. So the non-neuronal acetylcholine contributes to prevention of heart failure. It is necessary for the balance between parasympathetic and sympathetic heart innervation. In the heart failure parasympathetic tone is decreased, and sympathetic increased. Iron uptake in different cells MCF hephaestin or ceruloplasmin Fe3+ Fe2+ Haem Haem Diferric Tf HCP1 DMT1 Dcytb FPN1 STEAP 3 HO Fe-Tf-TFR1 Ferritin Duodenal enterocyte Diferric Tf in serum HO Endosome pH < 6 Ferritin Hepatocyte Haem from RBCs Apo Tf in serum Ferritin Macrophage Lecture prepared from The Cell: A Molecular Approach. 2nd edition http://www.ncbi.nlm.nih.gov/books/NBK989 8/ Molecular Cell Biology, Lodish and co 5Edition, Chapter 15 Assignment 1 Role of acetylcholine in the body. Heart diseases related to abnormal levels of acetylcholine. http://neuroscience.uth.tmc.edu/s1/chapte r11.html