Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
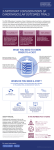
STRENGTHEN YOUR PRODUCT VALUE STORY ONE PHASE AT A TIME: A roadmap for gathering the evidence that regulators and payers want BY MANU SEHGAL, VICE PRESIDENT PAREXEL® INTERNATIONAL One in ten new drug applications (NDAs) submitted to the FDA fail to gain approval, according to the Tufts Center for the Study of Drug Development (TCSDD). While that may not seem high, these failures occur at the end of a process that TCSDD estimates takes more than a decade and costs up to $2.5 billion. Clearly, regulatory risk is not always eliminated as products advance. Of course, neither is commercial risk. Many drugs approved by regulators fail to win reimbursement from payers. According to the UK’s National Institute of Health and Care Excellence (NICE) website, of 382 appraisals conducted by NICE between 2000 and 2016, only 61 percent were recommended for reimbursement. The top reasons (in descending order) NICE gave were: non-robust economics; uncertain clinical benefits; inappropriate trial design, comparators, or patient populations; price, and safety concerns. How can a product license application land on the desk of FDA reviewers after years of development only to be rejected for insufficient safety, efficacy or quality (i.e. CMC data)? Why, after all the sponsors work, does NICE deem almost two-fifths of products economically unconvincing, clinically questionable, or questionably tested? One problem is that the traditional approach to building an evidence platform is fractured and sequential: regulatory teams seek to meet regulatory goals in each phase; commercial teams work on access considerations, usually waiting until a product is near launch before they begin their work in earnest. The endgame scramble that results when these two trajectories meet at the end of a lengthy development process impairs the product value story. Rarely is there a plan to integrate clinical and commercial perspectives at the various stages of a product’s journey, so that regulators and payers alike can find the value evidence they seek. Your phase-dependent evidence plan The solution is to staple clinical development and evidence generation together at the wrist. Developers should generate data to support the value story at each stage, from Phase I through post-authorization. Integrating all forms of value-generation activities at all phases of development requires detailed planning (Figure 1). A sound plan combines regulatory and reimbursement objectives, and pairs primary research, such as randomized clinical trials (RCTs), with secondary healthcare data assets (HDAs) such as patient registries, health insurance claims data, and medical literature reviews. PHASE I: SAFETY AND SURVEYING THE LANDSCAPE Although the primary goal of first-in-human trials is safety, companies should begin to leverage other types of data at this early stage. In the event a compound does not advance past Phase I, landscape assessment data about a therapeutic area or pharmaceutical class can be re-purposed for other assets in the portfolio, saving time and money. Evidence planning for every asset should include phasedependent primary and secondary research protocols to ensure optimal utilization of the two approaches while saving costs. In Phase I, the primary goals of clinical trials include: •E stablishing safety in humans (often healthy volunteers) • Determining dose escalation and tolerability • Determining treatment duration • Selecting outcomes/endpoints for subsequent testing. FIGURE 1. ALIGNING REGULATORY AND REIMBURSEMENT OBJECTIVES IN A SINGLE EVIDENCE PLAN: PHASE BY PHASE REGULATORY OBJECTIVES Disease epidemiology, treatment paradigm, and defining standard of care Phase II Phase I Value proposition development encompassing disease area and treatment landscape assessment including disease epidemiology, treatment paradigm, unmet need, defining standard of care Broader landscape Assessment for selection of appropriate patient reported outcomes in clinical trials Optimization of clinical trial endpoints, benchmarking efficacy and safety, and other trial design parameters Phase III Comparative effectiveness research for clinical efficacy and safety of the molecule and comparators Quantification of comparative effectiveness for value story demonstration per HTA requirements Cost-benefit value story development based on the economic evidence to form part of cost-effectiveness assessment Phase IV Focused positioning of the product addressing safety regulations and informing benefit/risk evaluations Value maintenance Adherence rates Therapy line expansion PLAN Preclinical Outcome selection, dose selection, Duration of follow-up Supporting PASS design, supporting Medical information needs, Risk management planning EVIDENCE Toxicology profile Pharmacological class assessment Pharmacokinetic evidence Trial design Sample size Justify comparators Duration of follow-up Adverse events Withdrawal rate Specific sub-groups Trial design Sample size Justify comparators Duration of follow-up Adverse events Withdrawal rate MULTI-ASSEST EVIDENCE PLANNING Specific sub-group based on histology type Specific sub-group based on mutation status LEADS TO Specific sub-group based on receptor status Customization of comparator list Customization of other products in same treatment class REIMBURSEMENT OBJECTIVES At the same time, secondary research should help to develop the value proposition and guide the overall evidence generation plan. A landscape assessment of the target disease area and treatment paradigm should cover: •D isease epidemiology (establishing incidence/ prevalence rates by geography) • Disease burden, especially unmet needs • Current standard of care (SOC), benchmark safety • Pharmacological class Secondary research, if used effectively and validated, can offer high-quality intelligence about market needs and a product’s potential early in the development journey. For example, recently a PAREXEL client with a rheumatoid arthritis (RA) biologic drug candidate wanted to understand the current key efficacy parameters for the disease, as well as the association between cognitive impairment (CI) and RA, to choose the best scoring instrument for measuring cognitive outcomes in Phase II and III clinical trials. We conducted a literature review of published RCTs, single arm studies and evidence published from registeries to summarize: 1) the effectiveness of current biologics in treating RA; 2) the association between CI and RA; and 3) the scientific validity and clinical relevance of various instruments, such as the MiniMental State Exam (MMSE) score and other cognitive battery scores, that could be used to assess cognition in an RA trial. Using that information, our client selected the most suitable instrument for future studies. In Phase I, secondary research can inform the design of prospective studies and help companies estimate the probability of success for a given molecule, leading to more informed go/no go decisions and pipeline prioritization. PHASE II: SHOULD THIS MOLECULE ADVANCE TO PHASE III? A primary goal of Phase II evidence collection is to ensure that investment in a given molecule is warranted before advancing to Phase III. Will the molecule address the needs of regulators, payers, and patients? For drugs that do, the sponsors’s central challenge is to learn enough to design and conduct the best possible trials for regulatory approval and beyond (i.e. reimbursement). In the “learning-confirming” continuum of drug development, Phase II trials are designed to: • Establish safety in the target patient population • Provide proof of concept for a drug’s mechanism of action • Select and justify sample sizes, and identify comparators, determine duration of follow-up, study adverse events and withdrawal rates, etc., for confirmatory trials • Capture preliminary efficacy signals that can inform go/no go decisions In Phase II, evidence plans must include secondary research to broaden and deepen the landscape assessment. For example, data from national patient registries can break out regional, national, and local disparities in disease incidence and prevalence, while country- and/or region-specific claims data can reveal differences in the current SOC for a given condition. Interviewing local affiliates can also be a rich source of data on geographic variation in healthcare delivery. Phase II is also when developers select appropriate patient-reported outcomes (PROs) for clinical trials. PROs are self-reported, and are often measured by responses to a questionnaire; they are increasingly used to provide evidence of value, especially for oncology drugs. For example, in 2013, the lung cancer drug, Xalkori (crizotinib), won the second highest benefit rating possible from IQWiG (the German agency responsible for assessing the quality and efficiency of medical treatments) even though it showed no advantage in overall survivial (OS, the regulatory/RCT gold standard of efficacy). The PRO measures used convinced German evaluators that the drug’s impact on morbidities in the target patient group was “considerable.” Quality of life (QoL) metrics showed significant improvements not only in patient well-being, but also in symptoms such as coughing and pain, illustrating that a disease-specific and standardized QoL instrument tracking common symptoms could be used as a powerful secondary endpoint. Other ways secondary research can contribute in Phase II include optimizing Phase III trial endpoints based on efficacy and safety benchmarks found in literature reviews, evaluating which trial design parameters may provide cost effectiveness data based on a review of previous submissions (both successful and unsuccessful), and defining the exact threshold for clinical differentiation versus Phase III comparator drugs. PHASE III: CONFIRMING THE VALUE PROPOSITION If Phase II trials have been conducted properly, Phase III trials should have a high probability of success. They should be designed to produce data that clear regulatory and reimbursement evidence thresholds for safety, clinical benefits, and medical value. Phase III (aka pivotal) trials: • Confirm efficacy of the molecule in the target population (including sub-groups) • Confirm appropriateness/performance of chosen comparators • Characterize safety profile: adverse events, withdrawal rates (including sub-groups) • Confirm duration of follow-up (clinical relevance, etc.) • Have large enough sample sizes to produce statistically valid data In Phase III, secondary research can strengthen the value proposition by filling in the cost-benefit ratio of a product based on economic evidence (such as health care utilization statistics) and quantifying product value and cost effectiveness for Health Technology Assessment (HTA) agencies. HDAs can often fill evidence gaps, as well. POST-AUTHORIZATION: DATA-DRIVEN MAINTENANCE OF THE VALUE STORY A PHASE-DEPENDENT EVIDENCE PLAN CAN CUT COSTS AND MITIGATE RISK Many of the clinical trials conducted post-authorization are mandated by regulatory agencies. Challenges in this phase often involve: Addressing evidence generation in a phase-specific manner provides mutually reinforcing benefits: trials contribute to the value argument and the value data inform the design of the trials. In this way, utilizing the best available secondary research to inform primary research can reduce the risk of regulatory and reimbursement rejections. • Optimizing post-authorization safety study (PASS) protocols for both mandated and non-mandated trials, and aligning those protocols with a risk management plan (RMP). • Satisfying medical information needs • Devising an RMP that meets pharmacovigilance requirements globally In today’s healthcare market, evidence of a product’s value is demanded long after it has been approved by regulators, and reimbursed by payers. Evidence planning continues to support activities postauthorization. Secondary research helps to generate long-term safety and compliance evidence that maintains and defends a product’s value story. For example, recently, a PAREXEL client needed an RMP for a biosimilar per EMA requirements. We conducted an SLR using specific safety terms to gather the latest published evidence for the new molecule. Our client used this data to construct an RMP for submission. Because the searches we conducted were systematic, they were reproducible, and could be repeated when the RMP needed updating. Similarly, we recently utilized meta-analysis techniques to demonstrate the safety of a client’s oral contraceptive in order to respond to EMA concerns about post-authorization adverse events. A phase-dependent approach has potential to cut costs by avoiding investing in riskier assets, utilizing secondary evidence for multiple assets (thereby using resources more efficiently) , and creating payer value while simultaneously meeting regulatory requirements. The best way to plan evidence generation for the value story is from the beginning. But if you didn’t do that already, the sooner you start the better. Addressing evidence generation in a phase-specific manner provides mutually reinforcing benefits: trials contribute to the value argument and the value data inform the design of the trials. PAREXEL® ACCESS POSITIONING YOUR PRODUCTS FOR MARKET SUCCESS. For more information, please contact: Elizabeth Thomae +1-720-935-4089 To find out more visit: www.PAREXEL.com/Access