Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
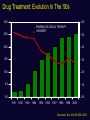
Terapia medica dell’IPB: focus su Silodosina Dr. Umberto Capitanio Department of Urology San Raffaele Scientific Institute, Milan, Italy Male LUTS EpiLUTS 14,139 men ≥ 40 years old 71% reported LUTS 46% storage symptoms Voiding symptoms only 12.1% 10.4% 24.3% Voiding + storage symptoms Storage symptoms only 10.3% Voiding + post micturition symptoms Post micturition symptoms only (3.0%) Voiding + storage + post micturition symptoms 9.1% Post micturition + storage symptoms (2.0%) Adapted from Sexton CC et al. BJU Int. 2009;103(Suppl3):12-23 LUTS: Treatment modality SURGICAL TREATMENT DRUG TREATMENT LIFESTYLE ADVICE Drug Treatment: Evolution In The ‘90s 30.0 6.0 PHARMACOLOGICAL THERAPY SURGERY 25.0 5.0 20.0 4.0 15.0 3.0 10.0 2.0 5.0 1.0 0.0 0.0 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 Souverein, Eur Urol 43:528, 2003 Alpha-blockers in daily practice 1 2 3 Recommendations LE GR α-blockers should be offered to men with moderate to severe LUTS Recommendations 1a LE A GR 1b A 1b B Combination treatment with α-blocker together with 5αreductase inhibitor should be offered to men with moderate to severe LUTS, enlarged prostates, and reduced Qmax (men likely to develop disease progression). Combination treatment is not recommended for shortterm therapy (< 1 year) Combination treatment with α-blocker and muscarinic receptor antagonist might be considered in patients with moderate to severe LUTS if symptom relief has been insufficient with the monotherapy of either drug EAU guidelines 2013 on conservative treatment of non neurogenic male LUTS, available at www.uroweb.org Alpha-blockers α1A α1B α1D Primary subtype expressed in the prostate. Regulates contraction of the smooth muscle in the prostate, bladder base and neck, urethra, seminal vesicles, and vas deferens. Primary subtype expressed in the blood vessels. Regulates contraction of arterial blood vessels in response to postural redistribution of blood volume. Primary subtype expressed in the bladder, spinal cord, and nasal passages. Thought to play a role in bladder symptoms and nasal secretions. Silodosin is an -adrenoceptor antagonist with high selectivity for the 1A receptors relative to 1B receptors α1-Blocker α1-Receptor Selectivity Doxazosin1 Terazosin1 Alfuzosin1 Tamsulosin1,2 Silodosin3 α1A = α1D = α1B α1A = α1D = α1B α1A = α1D = α1B α1A = α1D >α1B α1A >α1D >α1B 1. Schwinn DA, et al. Mayo Clin Proc. 2004;79:1423-1434. 2. Kenny BA, et al. Br J Pharmacol. 1996;118:871-878. 3. Akiyama K, et al. J Pharm Exp Ther. 1999;291:81-91. Results based on in vitro data α1-Blocker Receptor Selectivity α1A:α1B Silodosin Tamsulosin Alfuzosin Ratio expressed as the relative concentration. Tatemichi S, et al. Yakugaku Zasshi. 2006;12:209-216. Data on file, Watson Laboratories, Inc. KMD-0005 Study Report. 162:1 10:1 1:1 Results based on in vitro studies IN VITRO DIFFERENCES IN ALPHA-BLOCKER SELECTIVITY MAY NOT CORRELATE TO DIFFERENCES IN ACTUAL CLINICAL OUTCOMES. α1A Adrenoreceptor Expression Increases in BPH vs Non-BPH Prostate Tissue Non-BPH Tissue BPH Tissue α1A 63% 85% α1D 31% 14% α1B 6% 1% Nasu K, et al. Br J Pharmacol. 1996;119:797-803 SILODOSIN • Efficacy • Safety data • Who may benefit the most? Silodosin is efficacious within 2 - 6 hours… …..with sustained efficacy during 12-weeks treatment (8mg o.d) versus placebo (p<0.0001 – p<0.005) in two phase III trials in the USA Marks et al J Urol 181, 2634, 2009 More than 2,500 pts included in 5 RCTs Silodosin: 68% of responders (delta IPSS ≥25%) Capitanio et al. Int J Clin Pract, June 2013, 67, 6, 544–551 Pharmacokinetics and Safety data SILODOSIN does not inhibit cytochrome P450 enzyme systems at normal (8 mg) and supra-therapeutic (24 mg) doses had no meaningful effects on heart rate, PR, and QRS interval duration does not affect cardiac repolarization Marks et al J Urol 181, 2634, 2009 Silodosin has no effect on ECG parameters QTc interval Heart Rate Time-averaged change (beats / min) 10 5 placebo 0 Silodosin 8 mg od Silodosin 24 mg od -5 -10 In 139 healthy male subjects, placebo, silodosin 8 or 24 mg once daily for 5 days did not affect heart rate, QTc interval, PR-interval or QRScomplex and did not cause any deviations of the ECG morphology Morganroth et al Clin Pharm Ther 87, 609, 2010 Virtually no effect on blood pressure Chapple et al. Eur Urol 2011 SILODOSIN: SAFETY & TOLERABILITY Most common adverse reactions (all studies) Placebo controlled studies Preferred Term All studies Silodosin 8 mg (n = 931) Placebo (n = 733) Silodosin (n = 1,581) Total No. of patients with drug related AE 268 (28.8%) 66 (9.0%) 502 (31.8%) Retrograde ejaculation 200 (21.5%) 6 (0.8%) 373 (23.6%) Dizziness 17 (1.8%) 6 (0.8%) 33 (2.1%) Orthostatic hypotension 11 (1.2%) 7 (1.0%) 20 (1.3%) 9 (1.0%) 1 (0.1%) 20 (1.3%) Headache 10 (1.1%) 9 (1.2%) 20 (1.3%) Diarrhoea 6 (0.6%) 2 (0.3%) 16 (1.0%) Nasal congestion Silodosin Integrated Summary of Safety (September 2008) SILODOSIN: SAFETY & TOLERABILITY Discontinuations due to adverse reactions • In controlled studies 40/931 (4.3%) patients discontinued with silodosin, as compared to 14/733 (1.9%) patients on placebo • Overall (controlled + long term extensions), only 148/1,581 (9.4%) subjects discontinued the study due to TEAE • The most frequent cause was retrograde ejaculation (3.9%) SILODOSIN: EFFICACY Placebo Sil-EjD Sil+EjD Ejaculation disorder was associated with a significantly improved change in total IPSS at all time points from weeks 1-12 vs no ejaculation disorder or placebo Homma Y et al., Urology 2011 DIMINUZIONE DEL VOLUME DELL’EIACULATO Forte correlazione tra una importante riduzione nel volume dell’eiaculato e la gravità dei LUTS n = 11,063 (uomini con erezioni) Netta riduzione dell’eiaculato Aneiaculazione % 100 88 90 80 70 70 64 63 60 10 0 27 18 16 2 73 58 62 43 31 2 7 50 – 59 anni 2 67 57 44 36 25 2 69 45 38 40 20 50 45 50 30 81 78 6 5 60 - 69 anni 5 9 13 14 19 70 - 79 anni Rosen et al. Eur.Urol. 44(2003) 637-649 Terapia medica dell’IPB: focus su Silodosina A novel alpha blocker: Silodosin Who are the best candidates? Silodosin: who are the best candidates 1- Patients suffering from moderate-severe nocturia Post-hoc analyses: statistically significant superiority vs placebo, while tamsulosin not, in a subgroup of patients with at least 2 episodes of nocturia at baseline Michel et al. EAU Annual Meeting Vienna 2011 Montorsi et al. Eur Urol Suppl 2010; 9: 491-5 Silodosin: who are the best candidates 1- Patients suffering from moderate-severe nocturia 1. Nocturia 2. Frequency 3. Incomplete emptying Statistically significant superiority vs tamsulosin and placebo on the simultaneous improvement of nocturia, frequency and incomplete emptying Michel et al. EAU Annual Meeting Vienna 2011 Montorsi et al. Eur Urol Suppl 2010; 9: 491-5 Silodosin: who are the best candidates 2 – Patients with low blood pressure levels and patients concomitantly treated with antihypertensive medications • One third of the patients included in clinical trials received concomitant antihypertensive agents • Dizziness was cause of discontinuation in 8/1,581 pts (0.5%) and orthostatic hypotension in only 3/1,581 pts (0.2%) • Virtually no risk of orthostatic hypotension Agency EM. CHMP ASSESSMENT REPORT FOR Silodyx. Doc.Ref.: EMA/72316/2010. Procedure No. EMEA/H/C/001209. 2010. http://www.ema. europa.eu/docs/en_GB/document_library/EPAR_Public_assessment_report/human/001209/WC500074188. Silodosin: who are the best candidates 3 – Patients concomitantly treated with PDE5-I Heart-rate Systolic BP Diastolic BP MacDiarmid et24a Urology 75;l, 520, 2010 Silodosin: who are the best candidates 4 – Patients with ureteral stone EAU Guidelines 2014 Silodosin: who are the best candidates 4 – Patients with ureteral stone The density of α1 receptors (especially α1A and α1D) in the ureteral smooth muscle has been shown to be greater than other adrenoceptors Park et al. Urol Res 2007 55 male Sprague-Dawley rats (250-300gr) Saline infusion in the ureter through a PE-10 catheter at a speed 0.4ml/hour The psoas muscle was sutured around the distal part of the ureter to cause a partial distal obstruction. Carotid artery and femoral vein were cannulated in order to register mean arterial pressure and to administer drugs, respectively. α – BLOCKERS EFFECT IN VIVO α – BLOCKERS EFFECT IN VITRO - Silodosin reduces ureteral pressure with less systemic side effects than tamsulosin and prazosin - Silodosin exhibits better inhibitory efficacy on EFS-induced contraction of human and rat isolated ureters than tamsulosin and prazosin Villa et al. BJP 2013 Silodosin: who are the best candidates 5 – Chronic prostatitis/chronic pelvic syndrome-related symptoms Nickel JC et al. J Urol 2011. 186: 125-31 6 – Patients not satisfied (for efficacy or tolerability) with previous treatment with other alpha-blokers Miyakita et al. IJU 2010; 17: 869-75 7 – Brachytherapy-related symptoms Tsumura H et al. IJROBP 2011; 81: e385-92 8 – After Acute Urinary Retention for TWOC success Kumar et al. Urology 2013 CONCLUSIONI - 1 I LUTS sono molto frequenti nella popolazione generale I farmaci antagonisti dei recettori α1A-adrenergici rappresentano la terapia di prima linea nel trattamento dei LUTS La Silodosina ha dimostrato una selettività mai riscontrata per i recettori adrenergici α1A rispetto a α1B e α1D in studi di legame e funzionali. CONCLUSIONI - 2 La Silodosina ha un’efficacia pari a quella della tamsulosina, addirittura superiore in alcuni scenari clinici (e.g. nocturia) Grazie alla sua elevata uroselettività gli effetti collaterali a livello dell‘apparato cardiovascolare sono risultati minimi. Silodosina puo’ essere somministrata in concomitanza di PDE5-I Dati preliminari suggeriscono un ruolo determinante di silodosina nell’espulsione di calcoli ureterali, nei sintomi secondari a brachiterapia e nella CP/CPPS