Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
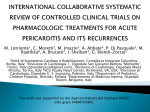
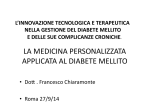
Journal Club Dutra Medeiros M, Mesquita E, Gardete-Correia L, Moita J, Genro V, Papoila AL, AmaralTurkman A, Raposo JF. First Incidence and Progression Study for Diabetic Retinopathy in Portugal, the RETINODIAB Study: Evaluation of the Screening Program for Lisbon Region. Ophthalmology. 2015 Sep 14. pii: S0161-6420(15)00781-2. doi: 10.1016/j.ophtha.2015.08.004. Bakris GL, Agarwal R, Chan JC, Cooper ME, Gansevoort RT, Haller H, Remuzzi G, Rossing P, Schmieder RE, Nowack C, Kolkhof P, Joseph A, Pieper A, Kimmeskamp-Kirschbaum N, Ruilope LM; Mineralocorticoid Receptor Antagonist Tolerability Study–Diabetic Nephropathy (ARTS-DN) Study Group. Effect of Finerenone on Albuminuria in Patients With Diabetic Nephropathy: A Randomized Clinical Trial. JAMA. 2015 Sep 1;314(9):884-94. doi: 10.1001/jama.2015.10081. 2015年10月8日 8:30-8:55 8階 医局 埼玉医科大学 総合医療センター 内分泌・糖尿病内科 Department of Endocrinology and Diabetes, Saitama Medical Center, Saitama Medical University 松田 昌文 Matsuda, Masafumi Microvascular Endpoints 15 Hazard ratio 10 p<0.0001 1 0.5 37% decrease per 1% decrement in HbA1c 0 5 6 7 8 9 10 11 Updated mean HbA1c UKPDS 35. BMJ 2000; 321: 405-12 ukpds 1 Portuguese Diabetes Association, Lisbon, Portugal 2 Department of Ophthalmology, Central Lisbon Hospital Center, Lisbon, Portugal 3 NOVA Medical School, Universidade NOVA de Lisboa, Lisbon, Portugal 4 University of Minho, Braga, Portugal 5 Statistics and Informatics Department, NOVA Medical School, Universidade NOVA de Lisboa, Lisbon, Portugal 6 Epidemiology and Statistics Unit, Research Centre, Central Lisbon Hospital Center, Lisbon, Portugal 7 CEAUL (Center of Statistics and Applications); University of Lisbon, Lisbon, Portugal 8 Department of Statistics and Operational Research, Faculty of Sciences, University of Lisbon, Lisbon, Portugal 9 Department of Public Health/CEDOC (Chronic Diseases Research Center), NOVA Medical School, Universidade NOVA de Lisboa, Lisbon, Portugal Ophthalmology. 2015 Sep 14. pii: S0161-6420(15)00781-2. doi: 10.1016/j.ophtha.2015.08.004. Purpose To estimate the 5-year incidence and progression of diabetic retinopathy (DR) among persons with type 2 diabetes mellitus (DM). Design Population-based, prospective, cohort study. Participants The RETINODIAB (Study Group for Diabetic Retinopathy Screening) program was implemented in the Lisbon and Tagus Valley area between July 2009 and December 2014. A total of 109 543 readable screening examinations were performed and corresponded to 56 903 patients who attended the screening program at entry. A total of 30 641 patients (53.85%) had at least 1 further screening event within the study period and were included in the analysis. Methods Participants underwent two 45°nonstereoscopic retinal digital photographs per eye according to RETINODIAB protocol. All images were graded according to the International Clinical Diabetic Retinopathy Scale. Referable diabetic retinopathy (RDR) was defined for all patients graded as moderate nonproliferative DR (NPDR), severe NPDR, or proliferative DR (PDR), with or without maculopathy or mild NPDR with maculopathy. Nonparametric estimates of the annual and cumulative incidences were obtained by Turnbull's estimator. Associations between the potential risk factors and the time to onset/progression of retinopathy were assessed through a parametric survival analysis for interval-censored data. Main Outcome Measures The authors estimated the onset and progression incidence rates of DR. 科学的根拠に基づく糖尿病診療ガイドライン2013 http://www.med.teikyo-u.ac.jp/~ortho/med/dis/dis2/dmr.htm Results Yearly incidence of any DR in patients without retinopathy at baseline was 4.60% (95% confidence interval [CI], 3.96– 4.76) in the first year, decreasing to 3.87% (95% CI, 2.57– 5.78) in the fifth year. In participants with mild NPDR at baseline, the progression rate to RDR in year 1 was 1.18% (95% CI, 0.96–1.33). Incidence of any DR and RDR and DR progression rate were associated with known duration of diabetes, age at diagnosis, and use of insulin treatment. Conclusions This longitudinal epidemiologic study provides the first Portuguese incidence DR data in a largescale population-based cohort of type 2 diabetes after a 5-year follow-up. Duration of diabetes, age at diagnosis, and insulin treatment were associated with increasing risk of incidence and progression of DR. A personalized schedule distribution of screening intervals according to the individual patient's profile should be implemented, with resulting benefits in terms of health costs. Message ポルトガルで2型糖尿病(DM)患者3万641人を対 象に、5年間の糖尿病性網膜症(DR)発症率と進 行率を集団ベースの前向きコホート研究で調査 (RETINODIAB試験)。ベースラインで非網膜症 だった患者のDR年間発症率は1年目4.60%(95% CI, 3.96 - 4.76)、5年目3.87%(同2.57 5.78)だった。糖尿病罹病期間、診断時年齢、 インスリン治療がDR発症および進行リスク増加 と関連した。 http://www.m3.com/clinical/journal/15856 Spironolactone Eplerenone George L. Bakris, MD1; Rajiv Agarwal, MD2; Juliana C. Chan, MD3; Mark E. Cooper, MD, PhD4; Ron T. Gansevoort, MD, PhD5; Hermann Haller, MD, PhD6; Giuseppe Remuzzi, MD7,8; Peter Rossing, MD9,10,11; Roland E. Schmieder, MD12; Christina Nowack, MD13; Peter Kolkhof, PhD14; Amer Joseph, MBBS15; Alexander Pieper, DiplStat16; Nina Kimmeskamp-Kirschbaum, PhD17; Luis M. Ruilope, MD, PhD18 ; for the Mineralocorticoid Receptor Antagonist Tolerability Study–Diabetic Nephropathy (ARTS-DN) Study Group 1University of Chicago Medicine, Chicago, Illinois L. Roudebush VA Medical Center and Indiana University, Indianapolis 3Department of Medicine and Therapeutics, Chinese University of Hong Kong, Hong Kong, China 4Baker IDI Heart and Diabetes Institute, Melbourne, Australia 5Department of Nephrology, University Medical Center Groeningen, Groeningen, the Netherlands 6Departments of Nephrology and Hypertension, Hannover Medical School, Hannover, Germany 7Istituto di Ricerche Farmacologiche Mario Negri, Clinical Research Center for Rare Diseases “Aldo e Cele Daccò,” Ranica (Bergamo), Italy 8Unit of Nephrology and Dialysis, Azienda Ospedaliera Papa Giovanni XXIII, Bergamo, Italy 9Steno Diabetes Center, Gentofte, Denmark 10University of Copenhagen, Copenhagen, Denmark 11Aarhus University, Aarhus, Denmark 12Department of Nephrology and Hypertension, University Hospital Erlangen, Erlangen, Germany 13Global Clinical Development, Bayer HealthCare AG, Wuppertal, Germany 14Heart Diseases Research, Global Drug Discovery, Bayer HealthCare AG, Wuppertal, Germany 15Global Clinical Development, Bayer PLC, Newbury, England 16MARCO GmbH & Co KG, Düsseldorf, Germany 17Global Research and Development Statistics, Bayer HealthCare AG, Leverkusen, Germany 18Institute of Investigation and Hypertension Unit, Hospital 12 de Octubre, Madrid, Spain 2Richard JAMA. 2015 Sep 1;314(9):884-94. doi: 10.1001/jama.2015.10081. Importance Steroidal mineralocorticoid receptor antagonists, when added to a renin-angiotensin system blocker, further reduce proteinuria in patients with chronic kidney disease but may be underused because of a high risk of adverse events. Objective To evaluate the safety and efficacy of different oral doses of the nonsteroidal mineralocorticoid receptor antagonist finerenone, given for 90 days to patients with diabetes and high or very high albuminuria who are receiving an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker. Design, Setting, and Participants Randomized, doubleblind, placebo-controlled, parallel-group study conducted at 148 sites in 23 countries. Patients were recruited from June 2013 to February 2014 and the study was completed in August 2014. Of 1501 screened patients, 823 were randomized and 821 received study drug. Interventions Participants were randomly assigned to receive oral, once-daily finerenone (1.25 mg/d, n = 96; 2.5 mg/d, n = 92; 5 mg/d, n = 100; 7.5 mg/d, n = 97; 10 mg/d, n = 98; 15 mg/d, n = 125; and 25 mg/d, n = 119) or matching placebo (n = 94) for 90 days. Main Outcomes and Measures The primary outcome was the ratio of the urinary albumin-creatinine ratio (UACR) at day 90 vs at baseline. Safety end points were changes from baseline in serum potassium and estimated glomerular filtration rate. Figure 1. Flowof Participants in the Mineralocorticoid Receptor Antagonist Tolerability Study–Diabetic Nephropathy Results The mean age of the participants was 64.2 years; 78% were male. At baseline, 36.7% of patients treated had very high albuminuria (UACR ≥300 mg/g) and 40.0% had an estimated glomerular filtration rate of 60 mL/min/1.73 m2 or lower. Finerenone demonstrated a dose-dependent reduction in UACR. The primary outcome, the placebo-corrected mean ratio of the UACR at day 90 relative to baseline, was reduced in the finerenone 7.5-, 10-, 15-, and 20-mg/d groups (for 7.5 mg/d, 0.79 [90% CI, 0.68-0.91; P = .004]; for 10 mg/d, 0.76 [90% CI, 0.65-0.88; P = .001]; for 15 mg/d, 0.67 [90% CI, 0.58-0.77; P<.001]; for 20 mg/d, 0.62 [90% CI, 0.54-0.72; P < .001]). The prespecified secondary outcome of hyperkalemia leading to discontinuation was not observed in the placebo and finerenone 10-mg/d groups; incidences in the finerenone 7.5-, 15-, and 20-mg/d groups were 2.1%, 3.2%, and 1.7%, respectively. There were no differences in the incidence of the prespecified secondary outcome of an estimated glomerular filtration rate decrease of 30% or more or in incidences of adverse events and serious adverse events between the placebo and finerenone groups. Conclusions and Relevance Among patients with diabetic nephropathy, most receiving an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker, the addition of finerenone compared with placebo resulted in improvement in the urinary albumin-creatinine ratio. Further trials are needed to compare finerenone with other active medications. Trial Registration clinicaltrials.gov Identifier: NCT1874431 Message 糖尿病性腎症でACE阻害薬またはARB治療中の821 人を対象に、非ステロイド性鉱質コルチコイド 受容体拮抗薬finerenoneの併用効果を無作為化 試験で検証。90日後、7.5、10、15、20mg/日群 で尿中アルブミン/クレアチニン比(AER)が低 下した(プラセボ補正後のベースラインに対す る比0.79[90% CI, 0.68 - 0.91;P=0.004]、 0.76[90% CI, 0.65 - 0.88;P=0.001]、 0.67[90% CI, 0.58 - 0.77;P<0.001]、 0.62[90% CI, 0.54 - 0.72;P<0.001])。 https://www.m3.com/clinical/journal/15821