Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
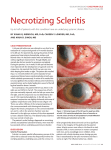
I. Introduction: A. Steroids: mechanism, type, & strength 1. topical 2. oral B. NSAIDs: mechanism C. Immunomodulation Agents: cyclosporin II. 75 yoAMF with severe deep eye pain, blurry vision, and “brittle type II diabetes A. Scleritis: 1. severe, rapidly progressive, destructive disease 2. fourth to sixth Decades of life, females > males 3. Clinical Charateristics: a. gradual pain (severe/boring) b. sectoral(60%) or diffuse(40%) injection all vessels c. limbal changes and peripheral keratitis d. sclerokeratitis/uveitis: 30% 4. Types: a. diffuse anterior scleritis: 30% systemic disease b. nodular anterior scleritis: 30% systemic disease c. necrotizing anterior scleritis with inflammation: 66% systemic disease d. necrotizing anterior scleritis w/o inflammation: 66% systemic disease e. posterior scleritis 5. Etiology and Differential Diagnosis: 6. Basic inflammatory work-up: 50% have known systemic disease CBC with differential ESR or CRP RF, ANA, ACE, ANCA RPR, FTA-ABS Serum uric acid PPD with anergy panel Lyme titer Chest x-ray, B-scan, CT/MRI urinalysis Cultures 7. Management: a. internist &/or rheumatology consult b. topical: prednisolone acetate q 1 hr vs q 10min qid c. oral: 1) NSAIDs: indocin 25-75 mg tid or ibuprofen 600-800mg tid 2) steroids: prednisone 60 to 80 mg 3) H2 blocker: rantidine 150 mg bid 4) Immunosuppressive therapy: cyclosporine, cyclophosphomide d. I.V. Methyprednisolone e. surgical grafting B. Cystoid Macular Edema 1. CME vs CSME 2. CME Management: a. NSAID vs prednisolone acetate vs NSAID & prednisolone acetate b. Steroid injections in scleritis: controversial III. 32 yoWF with sudden vision loss and eye pain A. differential diagnosis of optic neuritis B. Multiple Sclerosis 1. clinical features: 2. Devic’s Syndrome 3. management a. ONTT: Optic Neuritis Treatment Trial b. CHAMPS: Controlled High Risk Subjects Avonex MS Prevention Study: c. CHAMPIONS: Controlled High Risk Subjects Avonex MS Prevention Study In Ongoing Neurological Surveillence IV. 57 yoWF with burning, tearing eyes and reduced near A. Dry Eye 1. aqueous deficiency dry eye a. primary disease: Sjogren’s syndrome 1) inflammatory mediated dry eye: cascade 2) International Classification for Sjogren’s Syndrome: 4 of 6 needed Ocular symptoms: 1 of 3 symptoms: daily persistent dry eye > 3 months recurrent sandy scratchy eyes use of tear substitutes > 3 times per day Oral symptoms: 1 of 3 symptoms: daily feeling of dry mouth > 3 months recurrent or persistent swollen salivary glands as an adult drink liquids to swallow dry foods Ocular signs: 1 of 2 signs: Schirmer-1 test < 5mm in 5 minutes rose bengal score > 4 by van Bijsterveld scoring system Salivary gland involvement: 1 of 3 tests salivary scintigraphy parotid sialography unstimulated salivary flow < 1.5 mL in 15 minutes Histoplathologic findings: focus score > 1 on minor salivary gland biopsy Autoantibodies: antibodies to Ro(SSA) or La(SSB) or ANA or RF b. secondary Sjogren’s syndrome: RA, SLE, polymyositis, etc. 2. lipid deficiency dry eye 3. mucin deficiency dry eye 4. dry eye management: a. lipid layer: 1) warm compresses & lid scrubs bid 2) tetracycline 250mg po bid x 6 weeks 3) doxycycline 100 mg qd po x 6 weeks b. aqueous deficiency: 1) tear drop/gel/ointment supplements: preservative free 2) Restasis: .05% cyclosporin bid x 1 year 3) topical steroids: Lotemax vs FML vs Pred mild bid-qid x 4-6 weeks 4) fish oils: omega 3 fatty acids vs omega 6 fatty acids c. mucin deficiency IV. Episcleritis A. Signs/ Sx: 1. acute onset of redness 2. injection of superficial episcleral plexus may be nodular 3. episcleral edema 4. tearing, photophobia, foreign body sensation B. Epidemiology/ Etiology: 1. usually in young females 20-40yrs 5. 15-25% from allergy 2. often recurrent, transient, self 6. collagen vascular disease: 5-10% limiting (3weeks) 7. Relatively benign condition 3. Nodular form (20% of all cases) is 8. F>M somewhat more painful and runs a 9. 1/3 bilateral longer course 10. bilateral more commonly seen in – 2-3 mm diameter simple episcleritis – often involves pinguecula 11. mild anterior uveitis in 11% 4. 75% idiopathic 12. associated systemic disease: 32% C. Associated systemic diseases: 1. 13%connective tissue/ vasculitic 4. RA diseases (RA, inflammatory bowel 5. HZO Dz, SLE, Reiter’s) 6. EBV 2. 2% infectious disease: 7. polyarteritis nodosa (H zoster, H simplex) 8. syphilis 3. 17% miscellaneous Dz 9. TB D. Differential Diagnosis: 1. Scleritis 2. Iritis 3. Conjunctivitis E. Treatment 1. Mild disease a. Artificial tears b. Topical vasoconstrictors / antihistamine qid 2. Moderate disease: a. Fluorometholone qid, or Medrysone qid, or Pred mild qid or Flarex, NSAID’s V. VI. 3. Severe disease: a. Pred mild to Pred Forte qid b. Oral NSAIDS (e.g. Ibuprofen 200-600 mg po q 3-4 x /day c. EC ASA 325-1000 mg po q 3-4 x /day with food Iridocyclitis A. Fuch’s heterochromic iridocyclitis: 1. Etiology/ Epidemiology a. 2-5% of all uveitis ( often missed) b. 0-40 yrs of age c. etiology uncertain d. No HLA association 2. Signs: a. chronic, insidious i. Cataract (50%) b. predominantly unilateral g. Glaucoma in 25-50% (bilateral in up to 15%) h. Pars plana exudates, c. mostly quiet, white eye neovascularization d. Fine stellate KP’s i. Vitreous cells, vitreous e. Mild A/C cells hemorrhage f. Possible heterochromia j. Macular edema possible 3. Treatment a. Steroid resistant b. NSAIDS orally c. Periocular steroids for vitritis or macular edema d. Glaucoma management e. Cataract extraction w IOL 4. Differential Dx: infectious causes:Herpetic keratouveitis, herpetic iridocyclitis, noninfectious causes: connective tissue / inflammatory diseases: ankylosis spondylitis, Juvenile rheumatoid arthritis, Chronic cyclitis (young women) Vasculitic diseases. Others Idiopathic orbital inflammatory syndrome (IOIS) A. Symptoms: Swelling of the tissue around the eye with bulging of the eye, often painful, usually uniocular. B. Etiology: unknown. No risk factors are known. C. Differential Diagnosis: 1. Orbital pseudotumor, lymphoma, Grave's disease, less likely metastatic disease. (myositis, --scleritis, posterior scleritis, dacryoadenitis). 2. orbital cellulitis 3. thyroid eye disease 4. -Other conditions: dural sinus fistula, sarcoidosis, Wegener's granulomatosis, or an orbital tumor D. Clinical manifestations: vary widely, commonly include pain and proptosis. 1. symptoms develop within hours to days 2. Chemosis over the extraocular muscle insertions, eyelid edema, and ptosis 3. periorbital edema, erythema, and palpable mass 4. If orbital apex involved: marked restriction of EOM’s, pain, and min. proptosis, poor Va. 5. Tolosa-Hunt syndrome: superior orbital fissure and cavernous sinus -acute in onset. E. Signs and tests::Ultrasound, X-ray, Biopsy F. Treatment: 1. Mild cases may regress without treatment. 2. More severe cases will usually respond to corticosteroid. 3. Very severe cases may develop damaging pressure on the eye and requires surgical decompression. G. Prognosis: 1. Most cases are mild and do well 2. Severe cases may be resistant to treatment and visual loss may occur. H. Complications: Lid retraction, exposure keratitis, diplopia . I . Discussion: 1. idiopathic nongranulomatous inflammatory disorder 2. third most common orbital disease (5%-8%) 3. accounts for about 16% of all cases of unilateral proptosis in adults 4. most commonly presents between the third and fifth decades of life 5. M=F, no racial preference children 15% of all cases but more often bilateral Acute vs Chronic: a. acute more common- onset with pain, swelling, erythema, ptosis, painful/restricted eye movement, usually responds to steroids b. uncommonly chronic with diplopia, proptosis less commonly responds to steroids- XRT or chemo may help 8. involves lacrimal gland, EOMs, fat 9. orbital apex, cavernous sinus= Tolosa Hunt- painful ophthalmoplegia 10. other systemic diseases associated: Wegener's PAN RA RP fibrosis PSC SLE Reidel's dermatomyositis 11. imaging: -tendons involved and unilateral (to dist from Graves), marked enhancement, retrobulbar fat stranding, may present as focal or infiltrating mass, rare bone destruction, T2 hypo to distinguish from mets. J. Management: 1. High-dose short term steroids at a dose of 80 to 100 mg /day 2. the steroids are slowly tapered over several weeks. 3. Recurrences: may treat with high-dose steroids over a longer course and slower taper. 4. An anti-ulcer medication should be given concurrently for gastrointestinal prophylaxis 5. other immunosuppressive agents such as cyclophosphamide or radiotherapy 6. 7.