Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
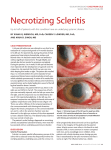
Episcleritis and Scleritis Recommend Urgent ophthalmologist referral within 24 hours [1] Background The episclera and sclera is thickened and discoloured 1. May present with: A red sore eye Episcleritis and scleritis differ from conjunctivitis in that they usually present as localised tender areas of inflammation Scleritis is more florid and much more painful than episcleritis The episcleral and scleral blood vessels are larger than the conjunctival vessels There may be a watery discharge 2. Immediate management: not applicable 3. Clinical assessment: Obtain a comprehensive patient history with particular note: medical history – any rheumatoid arthritis or any autoimmune disease, vascular or connective tissue disease family history current medications – is the patient taking any medications involving systemic steroids, NSAIDs, antimetabolites Perform standard clinical observations Examine both eyes starting with visual acuities – vision may be impaired in scleritis [1] sclera is thickened and discoloured the globe is tender to palpation (with eyelid closed) 4. Management: Consult MO and discuss further management including whether can be treated as per Conjunctivitis (episcleritis) evacuation/hospitalisation is needed for Ophthalmologist review (scleritis) within 24 hours 5. Follow up: If not evacuated/hospitalised, review daily Consult MO if: not improving on each review visual acuity deteriorates at any time See next MO visit 6. Referral / Consultation: Consult MO and see next MO clinic as above