Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
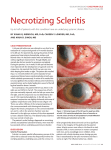
Painless Necrotizing Scleritis with Inflammation in Wegener’s Granulomatosis Divya Mutyala, M.D. Robert S. Feder, M.D. Feinberg School of Medicine Northwestern University Chicago, Illinois The authors have no financial interest in the material presented • Purpose: To report two cases of painless necrotizing anterior scleritis with inflammation • Methods: Retrospective chart review • Results: – Necrotizing anterior scleritis with inflammation was confirmed on external and slit lamp examinations in both patients – Both patients repeatedly denied pain and demonstrated no tenderness on examination despite severe inflammation – The patients were diagnosed with Wegener’s granulomatosis after being referred for treatment – Both patients were successfully treated with oral steroids and systemic immunosuppressive therapy Case 1 • 81-year-old woman with a one-month history of redness and a mass lesion on the bulbar surface of the right eye (OD) was referred for evaluation. She had mild photophobia, but denied discomfort or change in vision. Past history of chronic sinus congestion and recurrent nosebleeds. • Examination: – Best-corrected visual acuity (BCVA) 20/25- OD – External examination: an elevated, injected nodule on the temporal bulbar surface with an avascular necrotic center measuring 4.2 x 3.0 mm OD; no abnormal pigmentation – Slit-lamp examination (SLE): scleral thickening surrounding the necrotic patch; scleral thinning in the avascular area; no corneal involvement or involvement OS – Tension, fundus examination normal Case 1 Necrotizing Scleritis with Inflammation • The patient was treated with prednisone 60 mg daily. Five days later, the area of injection was diminished and the area of ulceration was shrinking. • A laboratory work-up revealed a positive classic antineutrophilic cytoplasmic autoantibody (c-ANCA) at 1:640, positive anti-nuclear antibody (ANA) at 1:40 speckled, elevated erythrocyte sedimentation rate (ESR) at 119, and a positive Proteinase-3 ANCA at 234. • Computed tomography (CT) of the sinuses revealed trace mucosal thickening in the anterior and posterior ethmoidal air cells without evidence of bony destruction, bony thickening, or sclerosis osteoitis. • A diagnosis of painless necrotizing nodular scleritis OD secondary to WG was made. Scleritis was successfully treated with prednisone. The patient began long-term immunosuppresive therapy. Case 2 • A 60-year-old woman in previously good health was referred with slowly progressive painless redness OD. The onset of the ocular symptoms was concurrent with a chronic sinus inflammation that had begun one month previously. Prior treatment included oral amoxicillin, methylprednisolone, triamcinolone nasal spray and 0.5% loteprednol etabonate eye drops. • Sinus CT was significant for bilateral mucosal thickening of the ethmoidal and maxillary sinuses • On examination: – BCVA was 20/25- OD – The external examination showed a hyperemic right upper lid with 2+ diffuse conjunctival injection – SLE revealed a band of peripheral keratitis superiorly OD – There were also several non-tender areas of scleral necrosis with inflammation at the superior limbus Case 2 Peripheral keratitis OD Case 2 Scleral necrosis with thinning at least 50% • The work-up revealed a positive c-ANCA level of 1:320 and a positive proteinase-3 ANCA at 102 units and a presumed diagnosis of WG was made • Treatment was initiated with oral prednisone 80 mg daily • Over a 3-year period, the patient was managed with tapering doses of oral prednisone and oral methotrexate with a maximum dose of 30 mg per week. Topical prednisolone acetate 1% was used intermittently when small peripheral corneal infiltrates would emerge OU • The c-ANCA ultimately normalized • Significant scleral loss with visible choroidal pigment was noted superiorly for several clock hours and following uncomplicated cataract surgery visual acuity of 20/30 OD sc was retained. Discussion • Of the different presentations of scleritis, necrotizing anterior scleritis with inflammation is the most severe and has the greatest potential for visual loss. Additionally, if these patients are not appropriately treated, the areas of inflammation may widen and cause complications of visual loss, peripheral ulcerative keratitis, uveitis, glaucoma, and rarely corneal perforation. The involved sclera can heal remarkably well when inflammation ceases. • Our two patients presented with dilatation of the deep episcleral vascular plexus with scleral necrosis and edema. Typically, pain and scleral tenderness would herald this presentation, yet our two patients had no discomfort. If necrosis had damaged the anterior ciliary nerves reducing pain perception, one might expect discomfort earlier in the course of the disease. • The most common systemic diseases associated with necrotizing scleritis are rheumatoid arthritis, Wegener’s granulomatosis, relapsing polychondritis, and systemic lupus erythematosus. • WG is a life-threatening disorder characterized by necrotizing granulomatous inflammation of the upper and lower respiratory tracts, vasculitis, and glomerulonephritis. Neither of our patients suffered any pulmonary or renal complications. • In pursuing a workup, a positive c-ANCA level and sinus CT findings of bony destruction, bony thickening, or mucosal thickening are helpful in providing a diagnosis of WG without a biopsy. Additionally, the antiproteinase-3 subset of ANCA is 85% sensitive and is a relatively specific marker for WG. • The radiologic, laboratory and clinical evidence in our patients helped formulate a presumptive diagnosis of WG. Conclusion • Early recognition of necrotizing anterior scleritis with inflammation is essential in reducing ocular morbidity and systemic complications. Clinicians are cautioned to avoid making the presence of pain and tenderness determinate factors for the diagnosis of necrotizing anterior scleritis, as this can potentially delay the appropriate systemic evaluation, and potentially eye saving and life saving therapeutic intervention.