Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
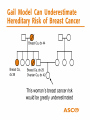
Breast Cancer Risk and Risk Assessment Models Jessica Ray, MS, CGC Cancer Genetic Counselor Ambry Genetic Laboratories [email protected] ¡Vida! Educational Series - Promoting Good Health Learning Objectives • Identify Personal and Family Characteristics that may indicate an inherited increased risk for cancer • Understand the role of genetic counseling in assessing patients with possible hereditary cancer syndromes • Understand characteristics, advantages, limitations, and differences of the Gail and BRCAPRO risk-assessment tools used by clinicians to help establish cancer risk Who Is at “High Risk”? • Atypia • 5-year Gail risk >1.7% • 2 or more 2nd-degree premenopausal affected relatives • Combined estrogen-progesterone hormone therapy for more than 10 years • Mammographically dense breasts • Obesity Who Is at “Very High Risk”? • • • • • Personal history of BC <50 BRCA1 or BRCA2 mutation carrier 2 or more 1st-degree relatives with BC Lobular carcinoma in situ (LCIS) Atypia and a 1st-degree relative with BC What is Genetic Counseling? Genetic Counseling is a communication process that deals with both the medical and psychological issues associated with the occurrence of a genetic disorder in a family • Cancer genetic counseling focuses on hereditary cancer syndromes • This process involves one or more trained professionals to help the individual or family Reasons for Seeking Genetics Consultation • To learn about • • • • Personal risk for cancer Children’s risk for cancer Family’s risk for cancer Risks for developing cancer if you have a “cancer gene” • Recommendations for screening, surveillance, and/or treatment • Educational information • To obtain genetic DNA testing J Med Genet 2000; 37:866-874 Key Flags that Warrant Genetic Counseling • Significant family medical history-breast, ovarian, prostate, colon, uterine, melanoma, pancreatic, or other cancers • Cancer occurs in every generation • Early age of onset (< 50 years) • Male breast cancer • Bilateral cancer, or multiple primary cancers in one individual • Known family genetic mutation • Ethnicity – Ashkenazi Jewish ancestry Sporadic, Familial or Hereditary? • 5-10% cancers have a hereditary component • Over 200 hereditary cancer syndromes described • Hereditary cancer tends to occur at younger ages than sporadic cancer, often bilateral, multifocal • Lifetime risks of cancer exceed cancer risks due to noninherited factors (early menarche, nulliparity, late age of menopause, HRT, etc) • Majority show an autosomal dominant inheritance pattern (few are recessive) Average Age of Diagnosis Hereditary • Breast 41 • Ovarian 40-50 • Prostate 63 Sporadic • Breast • Ovarian • Prostate 62 60 71 Gail Model National Cancer Institute http://www.cancer.gov/bcrisktool/Default.aspx Gail Model: Advantages • Identifies women who could benefit from preventive interventions; may assist in making clinical decisions (Determination of eligibility for tamoxifen for breast cancer risk reduction…Gail score>1.7) • Incorporates risk factors other than family history (eg, reproductive variables, atypical hyperplasia, history of breast biopsies) • Calculation of breast cancer risk in absence of family history in women • Shows that BC risk increases with age and, therefore, may prompt discussion about the importance of BC screening • Used to counsel and educate women, especially those who overestimate their BC risk Gail Model: Limitations • Not validated for black, Hispanic, and other ethnic groups • Only solicits family history involving first-degree relatives • May underestimate risk when family history is on father’s side • Does not take into account age at which relatives developed BC • Effect of number of breast biopsies (without atypical hyperplasia) may cause inflated risk estimates • May underestimate risk for women with demonstrated mutations of the BRCA1 or BRCA2 genes BRCAPRO - Advantages • Incorporates both affected and unaffected family members in estimation of carrier probability • incorporates maternal and paternal breast and ovarian cancer history • age at cancer diagnosis, current ages, ages relatives became deceased considered • Ashkenazi Jewish ethnicity taken into consideration • Oophorectomy status and breast cancer receptor status considered BRCAPRO - Limitations • Dependent on published estimates of prevalence and penetrance of BRCA1 and BRCA2 • Does not consider more distant family history past 1st and 2nd degree relatives • Does not consider other potential susceptibility genes with features similar to BRCA1 and BRCA2 When Do You Offer Testing? • American Society of Clinical Oncology recommends genetic testing : • The individual has a personal or family history of features suggestive of a genetic cancer susceptibility condition • The test can be adequately interpreted • The results will aid in diagnosis or influence the medical or surgical management of the patient or family members at hereditary risk of cancer ASCO recommendations: • Genetic testing only be done in the setting of pre-and post-test counseling, • Should discuss possible risks and benefits of cancer early detection and prevention modalities Implications/Important Points • What do we offer individuals at high risk for hereditary cancers who test negative for a genetic mutation? • Negative genetic test result does not mean No Increased Risk!! • AZCC High Risk Clinic for individuals at greater risk of developing cancer • Must continue studies to find other genes responsible for hereditary cancers • Must develop more advanced, individualized risk assessment tools