Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
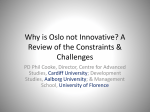
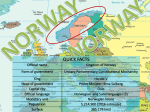
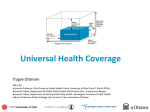
Poster I-5 Osteoprotegerin levels are associated with myocardial injury and function, but also heparin use in ST-elevation myocardial infarction. Christian Shetelig1,2,5, Shanmuganathan Limalanathan1,2,3, Jan Eritsland1,2,4, Pavel Hoffmann1, Ingebjørg Seljeflot1,2,4,5, Jon Michael Gran5,6, Pål Aukrust5,7,8,9, Thor Ueland5,7,9, Geir Ø. Andersen1,2,4. 1Department of Cardiology, Oslo University Hospital Ullevål, Oslo, Norway, 2Center for Clinical Heart Research, Oslo University Hospital Ullevål, Oslo, Norway, 3Feiring Heart Clinic, Feiring, Norway, 4Center for Heart Failure Research, Oslo, Norway, 5Faculty of Medicine, University of Oslo, Oslo, Norway, 6Oslo Center for Biostatistics and Epidemiology, Oslo University Hospital, Oslo, Norway, 7Research Institute of Internal Medicine, Oslo University Hospital Rikshospitalet, Oslo, Norway, 8Section of Clinical Immunology and Infectious Diseases, Oslo University Hospital Rikshospitalet, Oslo, Norway, 9K.G. Jebsen Inflammatory Research Center, University of Oslo, Oslo, Norway. Poster I-5 Background and purpose • Recent studies have shown that OPG levels are associated with infarct size in STEMI patients, however, the results have been inconsistent. • Aims of the study – To evaluate: 1. The temporal profile of OPG during ST-elevation myocardial infarction (STEMI). 2. Possible associations between OPG and infarct size, adverse left ventricular (LV) remodeling, microvascular obstruction (MVO) and myocardial salvage. 3. The possible effect of heparin administration on OPG levels. Poster I-5 Methods • Population: 272 patients with first-time STEMI treated with primary percutaneous coronary intervention (PCI). • Blood sampling immediately before and at the end of the PCI procedure, Day 1 (median 14.7 hours after PCI), and at 4-month follow-up. • Cardiac magnetic resonance imaging (CMR) performed in the acute phase and after 4 months. Poster I-5 Results Figure 1. Temporal profile of OPG during the course of STEMI. Data are presented as median (boxes) with 25th and 75th percentile (whiskers). Figure 2. Osteoprotegerin (OPG) levels in patients with suspected stable coronary artery disease before and after heparin administration. Blood samples were drawn from patients (n=20) during elective coronary angiography. A venous sample was taken before angiography (A). Arterial samples were taken immediately after cannulation (B, 1 min before heparin), and at the end of the angiography procedure (C, 20 min after heparin). Poster I-5 Results Table 1. Baseline characteristics of the study population related to osteoprotegerin (OPG) levels measured at day 1 (above or below median value). Table 2. Myocardial injury and function measured by CMR according to osteoprotegerin (OPG) values measured at day 1. Data are presented as median (25th, 75th percentiles) or numbers (%). OPG was measured median 14.7 hours after PCI. • Data are presented as median (25th, 75th percentile) or numbers (%). OPG was measured median 14.7 hours after PCI. Multivariable analyses: OPG remained significantly associated with infarct size and LVEF after adjustment for relevant clinical covariates, but not after adjustment for peak troponin T and peak CRP. Poster I-5 Conclusions • High levels of OPG are associated with myocardial injury, but not adverse remodeling or myocardial salvage. • The role of OPG as a potential biomarker in STEMI patients seems to be limited by a strong association with age, confounding effect of heparin administration, and little additive value to well-established biomarkers such as Troponin T and CRP.