Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
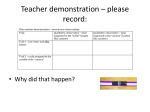
Anatomy & Physiology Lab Week 4: Respiratory System Station 1 : Using the respiratory lab materials a) Using a clean and disinfected mouthpiece, Measure your tidal volume (Vt) and fill out your Tv on the chart provided. Look at the variety of Vt’s in the class. Clean the mouthpieces with alcohol once you are done! Let dry b) c) What is your FEV? Over what time period is it measured in? Measure resting breath rate and active breath rate. Put it on the chart provided d) Now, since you know your Tv, and RR (at rest) what is your minute ventilation? How does this change during exercise. d) What is meant by “ breath control”. When would it be useful? Try the breath control exercise – please clean well with alcohol after use Station 2: Ventilation/Perfusion Ratio VENTILATION AND PERFUSION Ventilation is defined as the flow of air into and out of the alveoli. Perfusion is defined as blood flow to the alveoli. The lungs are composed of about 300 million alveoli that are capable of gas exchange. Gas is exchanged between the blood and the air. Thus, it depends on both ventilation and perfusion. To be the most efficient, the right proportion of alveolar air flow (ie.ventilation) and capillary blood flow (perfusion) should be available to each alveolus. Any mismatch is called ventilation-perfusion inequality. In an ideal lung, the V/Q ratio=1, ie. they are equal (V= ventilation and Q = perfusion). To understand the concept of V/Q inequalities it is best to visualize the simplest situations first. Thus, the two extremes of this phenomenon: 1) A ventilated alveoli with no blood supply (see alveolar dead space). 2) Blood supply to an alveoli that is not ventilated (this is a shunt). The major effect of any ventilation-perfusion inequality situation is that it lowers the PO2 of systemic arterial blood. In other words, the O2 in the alveoli will remain much higher than the O2 in the arterial blood. Go to this web site to look at the exercise in VQ Mismatch http://sprojects.mmi.mcgill.ca/resp/ventilation_perfusion.htm Station 3: Compliance/Resistance A. Resistance Resistance to air flow is caused by two forms of resistances: Airway resistance and Tissue resistance AIRWAY Resistance to flow: The first component of lung resistance is called airway resistance. Airway resistance is composed of: 1- Frictional resistance to flow (discussed below); 2- Acceleration or deceleration of gas flow due to changes in cross sectional area (see Bernoulli Effect). (http://sprojects.mmi.mcgill.ca/resp/bernoulli_effect.htm Frictional resistance: In a branched system, like that of our airways, frictional resistance depends on the individual resistances of each pipe and greatly depends on the manner in which they are connected. A small diameter causes a higher resistance, but the large number of parallel airways in that generation reduces the overall resistance. Remember that if you had 5 identical resistances in parallel, the total resistance would be 1/5 of any single resistance. Now imagine you have 20, 30 or 100 parallel resistance. The total resistance would then be 1/100 of any single resistance. At this distal point in the airways, the resistances become almost insignificant. Most of the overall airway resistance comes from generations 0 through 8. During normal tidal breathing, both components of airway resistance contribute majorly to air flow resistance. Look at http://sprojects.mmi.mcgill.ca/resp/resistance.htm B. Compliance Compliance = V / P Compliance is defined as the change in the volume of a closed system over the change in the pressure distending it. To explain the concept of compliance, we will use the example of a balloon. Compliance is the ease with which a balloon (or lung) can expand (ie. increase in volume). Thus the lower the pressure required to inflate the balloon, the greater the compliance. When a balloon is completely deflated (a collapsed lung), a high pressure is required to begin inflating it. As it is being inflated or if there is some residual air (like at RV), some of the elastic fibers in the balloon break, making it easier (ie. requiring less pressure) to continue inflating the balloon. As the balloon approaches its maximal distension (like at TLC), the elastic fibers of the balloon have less potential stretch, and therefore it becomes more difficult (requiring a higher pressure) to inflate the balloon further. If a high enough pressure is maintained the balloon will explode. Look at http://sprojects.mmi.mcgill.ca/resp/compliance.htm Exercise in lab: attach the BVM to the compliance resistance machine. A. Set to zero, set compliance and resistance also to zero (no springs, and dial to zero) Have partner not look at machine and just bag gently. What are the volumes they get with each “bag”? Measure 10 of them 1 6 2` 7 3 8 4 9 5 10 What is the average Tv your partner delivers with one hand? Switch and have your partner measure you B. Set Resistance to ‘100’ what do you notice about both the effort and the volume? Switch and have your partner try it! This mimics a moderate asthma patient C. Set resistance to ‘200’. Now what do you notice about effort and volume. ?? How hard is it to keep Tv at a set amount? Bag for 2 full minutes. What happens to your hand? The volume delivered breath to breath? Imagine doing that from the house to the hospital! This mimics a very severe asthmatic! D. Attach the springs to the machine (both). This is the closest mimic to compliance. How does this change your ventilation? Ensure your partner tries this as well Station 4 Fill in the partial pressure diagram attached to the lab. Label the percentages of gases that dissolve or are carried by HGB in the blood, as well as the relative partial pressures of both gases at both the alveoli and at the tissues Exercise 5: Workbook Exercises- Look at list attached. These are the unique characteristics of infants vs adults respiratory systems. KNOW THESE Match the condition with its description Condition Pneumonia Tuberculosis An emerging infectious disease, spread globally after first showing up in China in 2002 Pulmonary edema Slow shallow breathing asphyxia Cheyne-Stokes breathing Letter Description a. abnormal accumulation of fluid in the aveoli,due to left ventricular failure b. Irregular breathing pattern c. Hypoventilation d. oxygenation starvation e. Causes by a species of Mycobacterium; lung tissue is destroyed : incidence higher in patients who are immunocompromised f. acute infection or inflammation of the alveoli, which fill with fluid. g. Severe acute respiratory syndrome Exercise 5 :Arterial Blood Gases Medical Tests: The Respiratory System ARTERIAL BLOOD GAS (ABG) To measure the partial pressures of oxygen and carbon dioxide in a sample of arterial blood To measure the pH of arterial blood as a way of monitoring acid-base status To measure the bicarbonate ion level in arterial blood To evaluate cardiac and pulmonary function and the effectiveness of therapy for various cardiac and pulmonary diseases. Diagnostic Value A blood sample is taken from either the radial, brachial, or femoral artery. Procedure Normal Values 1. The sample is placed into an automated blood gas analyzer that measures pH, PO2, PCO2, bicarbonate ion concentration, and oxygen saturation pH: Oxygen (PO2): Carbon dioxide (PCO2): Bicarbonate ion (HCO3-): Oxygen saturation (SaO2): What would you say about a patient with the following gases? pH 7.31 paO2 42 paCO2 50 HCO3 22 2. Which patients (list 10 pathologies ) that would possible get ABG’s taken at the hospital?