Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
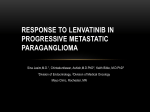
Metastatic Tumor of the Iris Mark R Parsons, OD, FAAO Reed Eye Associates Rochester, NY Grand Rounds 2015 American Academy of Optometry- New Orleans Abstract: A 55 year-old white male presents with a vascular fleshy-white mass of the iris, later to find stage 4 metastatic disease with lung as primary site. Unfortunately, the patient passes away shortly after initial visit. I. Case History a. 55 year-old, white male b. Chief Complaint: eye pain and irritation. Thinks he scratched his eye c. Ocular Hx: Myopia d. Medical Hx: 40 pack-years of smoking, hospitalized x 9/26/14 for “Possible pneumonia” per patient, concussion and neuropathic pain from severe car accident x 5/6/14 e. Medications: Lyrica II. Pertinent Findings a. Clinical: i. VA: 20/25 OD, 20/20 OS ii. Externals WNL iii. Posterior Segment exam unremarkable b. Physical: i. Vascularized, fleshy-white mass of iris root OD superotemporally ii. Microcystic edema localized to site of lesion from corneal touch iii. 3+ endothelial precipitates (combo of KPs and shed tumor cells) iv. 4+ AC Rxn (combo of WBCs and tumor seeding) c. Laboratory Studies: i. Basic Metabolic Panel (BMP): (Na+, K+, Cl-, CO2, ANION GAP, BUN, Cr, FBS, Ca2+)WNL ii. CBC w/ diff 1. WBC: high 2. RBC: Low 3. HCT: Low 4. HGB: Low 5. Lymphocytes: Low 6. Monocytes: Low 7. Neutrophils: High 8. Platelets: high iii. Troponin I: normal iv. Comprehensive Metabolic Panel (CMP) 1. Albumin: low 2. AST, ALT, ALK Phos: very high *** v. Blood Culture: negative for septicemia d. Radiology Studies: i. CT Chest w/ IV Contrast x 9/10/14 (ordered for pleural effusion seen on screening mammogram) 1. “Findings concerning for stage IV bronchogenic carcinoma w/ left hilar adenopathy/mass associated w/ postobstructive atelectasis of the left lower lobe, mediastinal adenopathy, bilateral pulmonary nodules likely to represent metastatic disease, hepatic metastases, and bilateral adrenal masses…low attenuation foci within both kidneys.” 2. “Heterogenous density characteristics of the right thyroid lobe which may warrant further work-up with thyroid ultrasound” 3. Biopsy of liver findings recommended due to accessibility ii. Chest X-Ray x 9/25/14 (indication was for shortness of breath) 1. Increased opacity at left base c/w known malignancy 2. Left Hilar Adenopathy iii. Ultrasound Guided Liver Biopsy x 10/1/14 iv. MRI of Brain w/ and w/o Contrast (9 lesions) x 10/8/14 1. Enhancing mass of left parietoocciptial lobe 3cm x 2.3cm x 2.9cm 2. Mass of choroid plexus 2.4cm x 1.4cm on right side 3. Enhancing mass of pineal gland 6.6mm 4. 3 Small enhancements of right frontoparietal watershed area 6.6mm x 6.6mm, 5.5mm, 4.8mm 5. Subtle enhancing lesion of left parietal lobe vertex 8mm x 6mm 6. Enhancing mass of left cerebellar hemisphere 3.4mm 7. Punctate enhancement of left cerebropontine angle III. Differential Diagnosis a. Primary: Metastatic tumor to iris b. Other: solid iris lesion related to car accident in May 2014; primary ocular tumor IV. Diagnosis and Discussion a. Metastatic tumor to iris from stage IV metastatic disease with lung as primary site b. The patient presented to our office with an incomplete medical history, one that he was hesitant to relay to the optometrist. He scheduled an appointment approx. 3 days before for a “possible corneal abrasion”. When medical hx was reviewed, he only reported the car accident and his recent admission to the hospital for “possible pneumonia”. The patient was further questioned, as it seemed very unusual and unlikely for a hospital to discharge a patient with a “possible” diagnosis. The patient admitted that the hospital thought it may be secondary pneumonia from a new mass that was found in his lung approximately 3 week ago. At this point, no cancer diagnosis has been made. He was scheduled for a US guided liver biopsy today. c. The features of the iris mass was classic for what is described in the literature, most notably by J. Shields and C. Shields. Metastases to the iris is rare, only accounting for ~7% of uveal metastases. Breast and lung cancer are the most common primary sources for uveal metastases (Men: Lung and GI, Women: Breast and Lung). Mean survival time of patients with uveal metastases is ~7 months per J/C Shields. d. A brief review of solid and cystic tumors of the iris will be discussed in the grand rounds V. Treatment and Management a. Specific to this case, communication with the patient’s internist was the primary treatment. b. Decision to biopsy the ocular mass with fine-needle biopsy aspiration was not performed as a liver biopsy was already scheduled. Biopsy of an ocular mass is only needed if primary site cannot be determined and/or the ocular site is the easiest site to biopsy c. XRT can be used in cases of recalcitrant iris tumors. Many times, systemic therapy of cancer will treat the ocular tumor as well. Decision for localized treatment is case-by- case. Our patient has yet to begin systemic treatment and the iris mass has not affected visual function. d. To relieve patient’s symptoms, the uveitis was treated with standard protocol: 5% homatropine BID and Pred Forte 1% q1h. e. Referral to our ophthalmologist was made 1 week later for evaluation. We decided to decrease the Pred Forte to QID, stop the homatropine, and taper quicker than usual. The goal was to relieve symptoms and allow the patient to resume CL wear in order to maximize quality of life for remaining survival time. The full presentation of the uveitis was not all inflammatory anyhow. Much of the cells observed was tumor seeding from the ocular mass. f. Bibliography: i. Chen CL, et al. Unilateral Iris Metastasis from Lung Cancer. J Med Sci. 25(6):319-322. 2005 ii. Cohen VML. Ocular Metastasis. Eye, 27:137-141. 2012 iii. Piperdi B, et al. Targeting Angiogenesis in Squamous Non-Small Cell Lung Cancer. Drugs. 74:403-413. 2014 iv. Shields CL, et al. Review of cystic and solid tumors of the iris. Oman Journal of Ophthalmology, 6(3). 2013. v. Shields CL, et al. Uveal Metastasis from Breast Cancer in 264 Patients. American Journal of Ophthalmology. 136(2). 2003 vi. Shields JA, et al. Metastatic Tumors to the Iris in 40 Patients. American Journal of Ophthalmology. 119:422-430. 1994 vii. Snee M. Bevacizumab in Non-small Cell Lung Cancer: An Overview of Practice in the Era of Molecular Testing. Clinical Oncology 26:468-472. 2014. viii. Soysal HG. Metastatic tumors of the uvea in 38 eyes. Can J Ophthalmol. 42(6). 2007 ix. Trichopoulos N, Augsburger J. Neuroendocrine tumours metastatic to the uvea: diagnosis by fine needle aspiration biopsy. Graefe’s Arch Clin Exp Ophthalmol. 244:524-528. 2006 x. Williams C, et al. Technology is Key to Iris Lesion Diagnosis. Review of Optometry. 4/15/2009. VI. Conclusion: a. The presence of a uveal metastatic tumor creates a poor prognosis for the patient as this suggests tumor cell spread via intracranial vascular supply. Since ~7% of uveal metastases are to the iris, it is imperative to rule out choroidal involvement in the posterior segment. Communication with the internist is imperative to initiate laboratory and radiographic testing to detect a primary site of cancer. Recommendation for neuroimaging is the rule with ocular involvement. Unfortunately, our patient passed away 3 weeks after the initial exam. Complications included failure to thrive secondary to dysphagia, respiratory failure, and postobstructive pneumonia. ***This case report includes images of brain MRI, US-guided liver biopsy, Chest X-Ray, and iris tumor.