Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
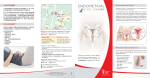
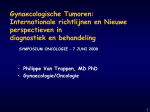
Malignant disease of the body of the uterus The most common malignant diseas affecting the uterus is endometrial carcinoma, which arises from the lining of the uterus. sarcomas also arise from the stroma of the endometriu'm or from the myometrium. introduction Incidence The incidence about age 45 years to about 55 years and remains at the same high rate thereafter. Etiology The cause of endometrial carcinoma is unknown Many of the factors are related to an increase in oestrogen levels. excess oestrogen as the prime factor in the development of endometrial cancer. The interaction between oestrogen, insulin and insulin-like growth factor-may be more important. In the postmenopausal period, the majority of circulating oestrogen is derived from aromatization of peripheral androgens. This conversion takes place principally in adipose tissue. In addition, postmenopausal women with diabetes have increased oestrogen levels.women with polycystic disease increase oestrogen level. Increasing evidence suggests that it is simplistic to view excess oestrogen as the prime factor in the development of endometrial cancer. The interaction between oestrogen, insulin and insulin-like growth factor-1 may be more important. risk factor number of factors that increase the risk of endometrial cancer are : Obesity. Impaired carbohydrate tolerance. Nulliparity Late menopause. Unopposed oestrogen therapy. Functioning ovarian tumours. Previous pelvic irradiation. Family history of carcinoma of breast, ovary. women who use oral contraception or progestogens have up to a 50 per cent reduction in the incidence of endometrial cancer and the protection lasts for many years after stopping these drugs. Cigarette smoking has also been associated with the reduced risk of endometrial cancer. Pathology The commonest subtype of endometrial carcinoma is called endometrioid because it resembles the normal proliferative endometrium. Squamous metaplasia can occur within adenocarcinomas and this can result in an adenoacanthoma or an adenosquamous carcinoma. Papillary serous and clear cell carcinomas . primary squamous cell carcinoma of the endometrium is extremely rare. uterus with adenocarcinoma of the endometrium. Clinical presentation 1-Most women with endometrial carcinoma will present with postmenopausal bleeding. 2- a postmenopausal discharge, particularly a bloodstained discharge. 3-premenopausal period, many women with endometrial carcinoma will present with intermenstrual bleeding. 4-one-third will present with heavy periods only. Diagnosis Traditionally, postmenopausal bleeding was investigated by a dilatation and curettage. More recently, however, diagnosis has shifted to the outpatient setting, with the ultrasound determination of endometrial thickness and outpatient sampling of the endometrium using instruments such as a Pipelle sampler in cases where the ultrasound suggests that the endometrium is more than 5 mm thick. If the sampler has been fully introduced into the uterus and no malignant tissue is identified, the test can be regarded as negative. Outpatient hysteroscopy may be Undertaken. Diagnosis Ultrasound also allows the ovaries to be imaged, as a number of patients with postmenopausal bleeding will have ovarian pathology. It is important to advise women to return if the bleeding recurs. Staging The FIGO classification and staging are │ The carcinoma is confined to the corpus II The carcinoma has involved the corpus and the cervix but has not extended outside the uterus III The carcinoma has extended outside the uterus but not outside the true pelvis IV The carcinoma has extended outside the true pelvis or has obviously involved the mucosa of the bladder or rectum Bullous oedema as such does not permit a case to be allotted to Stage IV Staging is usually by histopathology postoperative. Treatment Surgery The treatment of choice in patients with endometrial carcinoma is total abdominal hysterectomy and bilateral salpingo-oophorectomy. Most women with Stage IIdisease are not diagnosed until after the hysterectomyhas been performed. In such women, the prognosis is much the same as for Stage 1. Radical hysterectomy and bilateral pelvic lymphadenectomy with paraaortic node sampling is only performed if the cervical spread is clearly recognized before surgery. Even then,it is often wiser to treat the patient with radiotherapy like a cervical cancer Lymphadenectomy has not achieved an establishedplace in the treatment of endometrial cancer only samplingThe age, the obesity and the high rate of co-morbidity in these women detract further from the widespread adoption of lymph adenectomy in women with endometrial cancer Radiotherapy indication 1- postoperative radiotherapy deep myometrial invasion was regarded as an indication for this adjuvant treatment. 2-recurrent disease. In this group of women, salvage radiotherapy offers a 50 per cent cure rate. 3-the patient with more advanced disease, but surgery is not usually the first line of treatment. Pelvic radiotherapy is performed and then occasionally residual disease may be removed surgically. 4- radiation to para-aortic nodal disease if there is lymphatic spread. Hormonal therapy Progestogens 1-The only value of progestogens is in the palliation of recurrent disease. Good results are obtained rarely and only with well-differentiated tumors containing oestrogen receptors. 2-Women unfit for surgery. Five-year survival for women with endometrial cancer 5-year survival (%) Stage I Stage II Stage III Stage IV 83 71 39 27 Leiomyosarcoma Leiomyosarcoma arise in the uterine muscle. aris by transformation ofa previously benign fibromyoma(0.2per cent of fibro ids). Sarcoma also occasionally arises in the stroma of the endometrium -endometrial stromal sarcoma. pathology Tumours of this group grow more rapidly and are softer than fibromyomata. They may increase in size after the menopause.by naked-eye inspection, the tumour may be seen to have invaded the uterine wall or the capsule of the fibromyoma, and the cut surface often shows small haemorrhages and areas of degenerative softening. Microscopically, they consist of spindle-shaped or rounded cells, many of them pleomorphic, with little stroma and primitive blood vessels. Histological diagnosis of malignancy depends on the number of mitoses per high-power field (HPF). Metastasis Distant metastasis via the bloodstream and direct spread to adjacent structures often occur. DIAGNOSIS&TREATMENT These tumours occur in adults, who usually complain of uterine bleeding. Rapid growth of the tumour,with increasing pain, may give rise to suspicion of itsnature, but in many cases the diagnosis is made only after the tumour has been removed. In rare cases, asarcoma may be slow growing, and its nature discovered only when it recurs after operation. Sarcoma and mixed mesodermal tumours of the uterus Mixed mesodermal tumours This includes tumours that contain heterologous mesenchymal elements. In adults they often present as a large fleshy mass protruding from the uterine wall into the uterine cavity. Histological examination shows that it contains some elements resembling sarcoma and others resembling carcinoma, together with bizarre components such as cartilage and striped muscle. CLINICAL PRESENTATION . The patient complains of bleeding from the uterus, and sometimes of pain. Tumours of this type occasionally follow uterine irradiation. Metastasis via the bloodstream is common,as is local recurrence after removal The prognosis is poor. Sarcoma botryoides (embryonal rhabdomyosarcoma)is a variety of the same type of tumour that is seen in infants and young children. Clinical presentation There is a bloodstained,watery discharge and the vagina is found to contain grape-like masses of soft growth, usually arisingfrom the cervix. Local recurrence often follows removal, and distant metastases occur. Treatment total hysterectomy and bilateral salpingo-oophorectomy is performed, followed by external radiotherapy. radiotherapy must then be taken, depending on the extent and nature of the disease. The prognosis is poor,except for leiomyosarcoma arising in a fibromyoma. Treatment ofSarcoma botryoides (embryonal rhabdomyosarcoma) In children, as with many other forms of malignant disease, the prognosis with conventional treatment has been very poor. The modern use of a combination of external irradiation and chemotherapy hasaltered the outlook T H A N K Y O u