Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
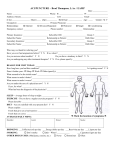
INTAKE FORM NAME:____________________________________________________ DATE: ___________ Reason for your Visit: _______________________________________Medication Allergies___________________________________ Has your child had any major illnesses since your last office visit? □ No □ Yes _______________________ Has your child had any surgeries since your last office visit? □ No □ Yes _______________________ Has your child had any hospitalizations since your last office visit? □ No □ Yes _______________________ Please describe any other changes to your family history or social history here: □ None ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ Medications your child is currently or recently on including over the counter and prescription: __________________________________ ____________________________________________________________________________________________________________ Did they finish the full prescription? □ Yes □ No If No, when did they stop it?_____________________________________________ Briefly, describe your child’s current symptoms: ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ REVIEW OF SYSTEMS: If your child is experiencing or has recently experienced any of the following, please mark below: General Ears Urinary Nervous System □ Fever: ___________°F □ Ear Pain □ Pain □ Fainting □ Weight loss □ Poor hearing □ Blood in urine □ Blackouts □ Weigh gain □ Ringing in ears □ Urgency □ Seizures □ Fatigue □ Dizziness □ Incontinence □ Paralysis Skin □ Infection □ Bed wetting □ Local weakness □ Rash □ Discharge □ Infections □ Numbness □ Swelling □ Excess ear wax □ Frequency □ Tingling □ Dryness Noses/Sinuses □ Urinating less □ Tremors □ Itching □ Runny Nose Endocrine □ Memory □ Eczema □ Nasal stuffiness □ Heat intolerance Mind □ Color change □ Allergies □ Cold intolerance □ Nervousness □ Infection □ Nosebleeds □ Excessive sweating □ Lack of concentration □ Change in hair □ Sinus trouble □ Excessive thirst □ Memory issues □ Change in nails □ Color_____________ □ Excessive hunger Emotions Blood Mouth/Throat □ Excessive urination □ Mood swings □ Abnormal blood test □ Cavities Circulation □ Depression □ Bleed easily □ Cold sores □ Leg cramps □ Excess anger □ Bruise easily □ Hoarseness □ Cold extremities □ Sadness □ Anemia □ Sore throat Digestion □ Frustration Head □ Blisters □ Excess □ Belching □ Mania □ Headache Lungs □ Bloating □ difficulty feeling or expressing emotions □ Head Injury □ Cough □ Passing Gas Neck □ Wheezing □ Trouble swallowing Please list other: □ Swollen nodes □ Shortness of breath □ Heartburn _____________________________________ □ Stiffness □ Difficulty breathing □ Nausea □ Pain Heart Appetite □ increased _____________________________________ Eyes □ Heart murmur □ Decreased □ Poor vision □ Palpitations □ Vomiting _____________________________________ □ Blurry vision Musculoskeletal □ with blood □ Sensitive to light □ Joint pains □ Abdominal pain _____________________________________ □ Pain □ Stiffness □ Constipation □ Redness □ Backache □ Diarrhea □ Discharge □ Muscle pain or □ Blood in stool □ Excess tearing cramps □ Change in bowel habits □ Double vision Stools □ pale □ black □ Infections Office Use Only: B/P __________ P _________ R _________ Pulse Ox __________ Temp __________ HT _________ WT _________