Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
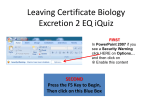
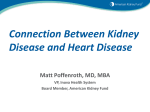
CHRONIC KIDNEY DISEASE Definition Chronic kidney disease (CKD) refers to the myriad problems that follow loss of kidney function. It results from a large number of diseases that either are systemic and damage the kidney or are intrinsic to the kidney ( Table 131-1 ). CKD has two characteristics. First, there is chronicity because the kidney damage of CKD is rarely repaired and loss of function persists, unlike the course of acute kidney failure. Second, loss of kidney function generates even more kidney damage so that CKD progressively worsens even if the disorder that caused it becomes inactive. CKD is the preferred term because another widely used one, chronic renal failure or insufficiency, is not as easily identifiable by patients as a disorder that affects the kidney. In addition, chronic renal failure suggests that the kidneys have lost all of their function, whereas CKD covers the spectrum of clinical problems beginning with abnormalities detectable only by laboratory testing to a late stage, labeled uremia. Uremia literally means “urine in the blood” and represents the toxic state principally resulting from accumulation of unexcreted waste products derived from metabolism of protein. When the kidney fails to perform most of its function, the clinical state is labeled end-stage renal disease (ESRD), and dialysis or transplantation is required to sustain life. The progressive and chronic nature of CKD is emphasized because treatment can slow or even halt the loss of kidney function, and many symptoms of uremia can be ameliorated or eliminated. TABLE 131-1 -- CAUSES OF CHRONIC RENAL FAILURE Diabetic glomerulosclerosis[*] Hypertensive nephrosclerosis Glomerular disease Glomerulonephritis Amyloidosis, light chain disease[*] [*] Systemic lupus erythematosus, Wegener's granulomatosis Tubulointerstitial disease Reflux nephropathy (chronic pyelonephritis) Analgesic nephropathy Obstructive nephropathy (stones, benign prostatic hypertrophy) Myeloma kidney[*] Vascular disease Scleroderma[*] Vasculitis[*] Renovascular renal failure (ischemic nephropathy) Atheroembolic renal disease[*] Cystic diseases Autosomal dominant polycystic kidney disease Medullary cystic kidney disease * Systemic disease involving the kidney. Epidemiology The increase in the number of patients with ESRD in the United States and other industrialized countries has features of an epidemic. For example, the number of patients with ESRD in the United States increased by an average of 5% between 1980 and 1990, and the incidence of ESRD was 219 per million population in 1991 but grew to 334 per million by 2000. A recent assessment suggests that the rate of increase of patients with ESRD is falling to an annual increase of 1% or less, possibly because of the emphasis on earlier detection of CKD and aggressive treatment of hypertension and especially more widespread treatment with blockers of the renin-angiotensin-aldosterone system (see later). Population-based studies such as the National Health and Nutrition Survey, a cross-sectional survey of U.S. adults, have uncovered the magnitude of the CKD problem ( Table 131-2 ). Approximately 8 million persons are afflicted with stage 3 or stage 4 CKD and hence are at high risk of progressive kidney failure. Two disorders account for almost 70% of all new ESRD patients; in 2003, 44.8% had diabetes mellitus and 27.1% had hypertension-induced kidney damage. The populations experiencing the highest incidence were the elderly (i.e., >65 years) and African Americans plus Native and Asian Americans. The reasons for the racial susceptibility to CKD are unknown. Besides a racial susceptibility, groups that have been identified as being at high risk for progressing from CKD to ESRD are those with hypertension, diabetes mellitus, or cardiovascular disease and those with family members who have ESRD. Other epidemiologic factors that have been identified as increasing the risk of progressive CKD include smoking, albuminuria, obesity, and hyperlipidemia. The presence of any of these factors should be sought and attempts made to correct them in treating a patient with CKD. TABLE 131-2 -- STAGES OF CHRONIC KIDNEY DISEASE (CKD) WITH PROJECTED NUMBERS OF INDIVIDUALS AND THE FREQUENCY OF COMPLICATIONS GFR[*] Stage Description 1 Chronic kidney damage with (mL/min/1.73 m2) >90 Projected Number (×1000) Symptoms or Signs 5900 normal or increased GFR Anemia 4% Hypertension 40% 5-year mortality 19% 2 Mild GFR loss 60–89 5300 Anemia 4% GFR[*] Stage Description Projected 2 (mL/min/1.73 m ) Number (×1000) Symptoms or Signs Hypertension 40% 5-year mortality 19% 3 Moderate GFR loss 30–59 7600 Anemia 7% Hypertension 55% 5-year mortality 24% 4 Severe GFR loss 15–29 400 Hyperphosphatemia 20% Anemia 29% Hypertension 77% 5-year mortality 46% 5 Kidney failure <15 or dialysis 300 Hyperphosphatemia 50% Anemia 69% Hypertension >75% 3-year mortality 14% Scr = serum creatinine. * The formula for estimating the glomerular filtration rate (GFR) of adults with CKD is derived from data obtained during the National Institutes of Health Mod-ification of Diet in Renal Disease trial. GFR 186 × [SCr]-1.154 × [age]-0.203 × [0.742 if patient is female] × [1.212 if patient is black]. Pathophysiology Physiologic and metabolic functions of the kidney include the regulation of ion concentrations in the extracellular and intracellular fluids, the regulation of blood pressure, the regulation of several endocrine functions, and the excretion of waste products ( Table 131-3 ). The breadth of these functions yields several predictable and some unpredictable consequences of CKD. For example, it is predictable that limitation of the ability to excrete acid would cause hyperventilation and a decrease in Pco2, but acidosis also causes less easily predictable losses of muscle mass and bone disease. Although changes in bone metabolism could be predicted from impaired excretion of calcium and phosphates, the discovery that the rate of parathyroid hormone (PTH) secretion varies with activation of calcium-sensitive receptors on parathyroid cells as well as the actions of vitamin D was not predictable. To understand the complex pathophysiologic process of CKD, certain principles must be integrated. TABLE 131-3 -- FUNCTIONS OF THE KIDNEY AND PROBLEMS DUE TO IMPAIRMENT OF KIDNEY FUNCTIONS IN PATIENTS WITH CHRONIC KIDNEY DISEASE Kidney Functions Consequences of Dysfunction Maintain concentrations and Hyponatremia, hyperkalemia, low total potassium content, body contents of electrolytes hypocalcemia, hyperphosphatemia, decreased tolerance to electrolyte and fluid volumes or mineral loading Regulate blood pressure Hypertension, cardiovascular disease Endocrine mediators Anemia (low erythropoietin), hypertension (renin system activation), bone disease (secondary hyperparathyroidism), low vitamin D activation, prolonged half-lives of peptide hormones (e.g., insulin) Waste product excretion Anorexia, nausea, soft tissue deposition of oxalates and phosphates, neurologic dysfunction, loss of muscle protein Balance and Steady-State Considerations The first principle, balance, is the condition in which the intake or production of a substance equals its elimination. For example, a loss of nephrons impairs the ability to excrete sodium, but there is an adjustment by the remaining nephrons to excrete a greater fraction of the sodium that is filtered by each glomerulus. Similar phenomena occur with other ions and substances, allowing the patient with CKD to avoid accumulation of sodium or potassium, for example. The ability to achieve balance has a limit, however, and when this limit is reached, ions and other molecules destined for excretion by the kidney will instead accumulate unless the intake or production of the retained ion or compound is reduced. A related concept is that of the steady state. A patient is in the steady state when the intake or processes of production and elimination are not changing. Although a patient in balance is also in the steady state, the converse is not necessarily true. A patient can be in the steady state but not be in balance because he or she is gaining or losing an ion or compound at a constant rate. For example, if nitrogen intake is less than the excretion of nitrogen, a patient will be losing protein stores. Such a patient would be in the steady state but in negative nitrogen balance. The Tradeoff Hypothesis The second important principle, the tradeoff hypothesis, is that a patient with CKD will achieve balance by activating pathophysiologic responses, but the responses lead to a tradeoff that has the potential of causing adverse consequences. A classic example is the responses activated in CKD to achieve sodium balance. CKD initially reduces salt excretion, leading to sodium retention and expansion of extracellular fluid. The result is high blood pressure. Although a higher blood pressure is beneficial because it increases the filtration and excretion of sodium, the tradeoff for maintaining sodium balance is persistent hypertension. There is experimental evidence that another adjustment that can prevent salt accumulation is an increase in circulating inhibitors of Na+,K+-ATPase in patients with CKD. These inhibitors increase the sodium concentration in tubular cells, thereby reducing the ability of the cell to reabsorb filtered sodium. The tradeoff for the ability to increase sodium excretion is that some patients with CKD will not tolerate an abrupt decrease in sodium intake, and persistent sodium excretion will lead to a fall in extracellular volume, impaired perfusion of the kidney, and a decrease in glomerular filtration rate (GFR). Another CKD tradeoff occurs in response to a decreased ability to excrete potassium. The rise in serum potassium stimulates adrenal aldosterone production, which stimulates potassium excretion by both the damaged kidney and the colon. The tradeoff for this adaptation is an increase in blood pressure caused by aldosterone-mediated sodium retention. The most intensely studied tradeoff is the adaptation to phosphate retention. When CKD limits the kidney's ability to excrete phosphates, they accumulate in extracellular and intracellular fluids. For example, CKD patients given a challenge dose of phosphates develop supranormal blood phosphorus levels. Accumulated phosphates form calcium-phosphate complexes and decrease the circulating concentration of ionized calcium. This in turn stimulates the production and release of PTH, a beneficial response because it suppresses the reabsorption of phosphates by the proximal tubule. The subsequent increase in phosphate excretion leads to a rise in ionized calcium, but the tradeoff is that the new steady state is maintained only as long as circulating PTH concentration is high ( Fig. 131-1 ). The tradeoff is stimulation of osteoclastic activity in bone that accelerates release of minerals, leading to uremic bone disease ( Chapter 132 ). It follows that restriction of phosphates in the diet plus the use of phosphate binders to increase gastrointestinal excretion of phosphates will eliminate the increase in circulating PTH concentration. This has been demonstrated experimentally and in CKD patients. FIGURE 131-1 A decrease in glomerular filtration rate (GFR) is followed by an increase in serum phosphorus and a decrease in serum calcium. An increase in serum parathyroid hormone (PTH) returns phosphorus and calcium to normal levels. Hypertension Hypertension, like anemia, is almost universal in CKD patients and often is the first sign of CKD. The coincidence of CKD and high blood pressure is particularly important because hypertension contributes to the development of cardiovascular disease, the leading cause of morbidity and mortality in CKD patients. Hypertension in CKD patients is mainly the result of an expanded extracellular volume from a salt-rich diet and a decreased capacity for excretion of sodium. As discussed earlier, the normal response to an increase in the extracellular volume is a rise in blood pressure that stimulates sodium excretion to achieve a balance between sodium intake and the excretion of salt. In the steady state, however, salt balance can be maintained only as long as blood pressure is high unless dietary salt is restricted and diuretics are used to increase sodium excretion. Two practical implications arise from these relationships. First, they reveal why treatment of hypertensive patients with vasodilating drugs alone is frequently unsuccessful. When vasodilator drugs reduce blood pressure, the fall in sodium excretion leads to sodium retention and expansion of extracellular volume that raises blood pressure. Second, they explain why control of the amount of salt in the diet is required even when diuretics are used to treat hypertension in CKD patients. A salt-rich diet can cancel the benefits of using diuretics, ultimately leading to expansion of extracellular volume and reappearance of hypertension. Another mechanism for hypertension in CKD patients is activation of the renin-angiotensin-aldosterone (RAA) system and the sympathetic nervous system. Evidence for activation of the RAA system in CKD patients includes circulating levels of renin and aldosterone that are too high for individuals who are hypertensive, suggesting that the vasoconstrictive action of angiotensin II and the salt retention induced by aldosterone contribute to hypertension ( Table 131-4 ). Other evidence includes the beneficial effects of inhibitors of the RAA system in reducing kidney damage and slowing the loss of kidney function. Evidence for activation of the sympathetic nervous system includes higher circulating levels of norepinephrine and the detection of increased sympathetic nerve activity in certain dialysis patients. The sympathetic nervous system not only causes vasoconstriction but also can suppress nitric oxide production in CKD patients. Finally, patients with hypertension frequently have serum uric acid values in the upper range of normal or at supranormal levels. Experimentally, a high uric acid level can cause vascular damage, suggesting that uric acid could play a role in the genesis of hypertension in CKD. The close association between CKD and hypertension (see Table 131-2 ) and the damaging effects of hypertension are the reasons that subjects with persistent hypertension (especially those with hypertension and diabetes or other systemic diseases) should be examined yearly for evidence of kidney damage. TABLE 131-4 [*] -- ANGIOTENSIN II RESPONSES IN CHRONIC KIDNEY DISEASE Hemodynamic responses Systemic hypertension Vasoconstriction Salt retention (aldosterone) Intraglomerular hypertension Efferent arteriolar vasoconstriction Nonhemodynamic responses in the kidney Macrophage infiltration and inflammation Interstitial matrix accumulation Increased transforming growth factor-β Increased plasminogen activator inhibitor type 1 Increased aldosterone * The proposed actions of angiotensin II that can contribute to the development of cardiovascular disease and progressive loss of kidney function. Endocrine Disorders The mechanisms causing bone disease in CKD patients include abnormalities in endocrine responses other than stimulation of PTH secretion. Vitamin D is activated by repeated hydroxylations of the parent molecule, cholecalciferol or vitamin D3. The initial hydroxylation occurs in the liver, forming 25-hydroxyvitamin D3. Although 25-hydroxyvitamin D3 can influence the function of muscle and other organs by poorly defined mechanisms ( Chapter 132 ), it mainly serves as a substrate for a second hydroxylation at the 1α position to form 1,25-dihydroxyvitamin D3, the most active form of vitamin D. This critical step is catalyzed by 1α-hydroxylase activity in the proximal tubule of the kidney, so loss of kidney function results in decreased function of 1,25-dihydroxyvitamin D3, including lower absorption of calcium and phosphorus by the gastrointestinal tract and reduced suppression of PTH secretion. The decrease in phosphate absorption plus the persistent stimulation of renal phosphate excretion by the action of PTH accounts for the low values of serum phosphorus that are measured in blood samples obtained after an overnight fast. These considerations indicate why vitamin D should not be given to CKD patients with high serum phosphorus levels. Stimulation of gastrointestinal calcium and phosphate absorption can cause hypercalcemia and, by stimulating the accumulation of phosphates, will initiate the mechanisms that raise circulating PTH concentration (see earlier). Decades ago, it was shown that CKD causes insulin resistance by reducing the ability of insulin to stimulate glucose uptake by muscle and other organs ( Chapter 248 ). This leads to an increase in circulating insulin concentration, even in CKD patients without type 2 diabetes. In insulin-resistant CKD patients, insulin has been shown to interact normally with its receptor, so the failure to stimulate glucose metabolism is due to a post-receptor defect in cell signaling. The abnormality in insulin-stimulated cell signaling mechanisms is controversial; one possibility is decreased ability to activate phosphatidylinositol 3-kinase and its downstream kinase, Akt. Reduced function of these enzymes in muscle cells impairs the metabolism of both glucose and protein. Clinically, the insulin resistance of nondiabetic CKD patients is rarely associated with blood glucose levels above 200 mg/dL. In fact, blood glucose concentration is usually normal or only slightly high because insulin secretion rises to overcome defects in cell signaling. One possible initiator of insulin resistance is metabolic acidosis, a frequent complication of CKD. Metabolic acidosis will impair insulin-stimulated glucose uptake in normal adults, and it causes loss of muscle protein, an insulin-sensitive metabolic function. Metabolic acidosis can contribute to other CKD-induced endocrine abnormalities; it impairs the ability of growth hormone to stimulate insulin-like growth factor 1. When this is combined with impaired metabolism of bone minerals, it contributes to the impaired growth of children with CKD. Metabolic acidosis also impairs thyroid function by increasing thyroid-stimulating hormone and depressing circulating levels of thyroxine (T4) and triiodothyronine (T3); similar changes are present in the sick euthyroid syndrome ( Chapter 244 ). Metabolic acidosis should be eliminated because its correction largely eliminates these abnormalities in CKD patients. Another impaired kidney function that affects a patient's endocrine status is the ability to degrade small proteins, including several hormones. For example, diabetic patients treated with their usual dose of insulin can develop hypoglycemia with progressive loss of kidney function because the damaged kidney does not remove enough of the injected insulin. This same function also affects interpretation of circulating PTH concentrations because the damaged kidney leads to accumulation of different fragments of PTH; it is important to know whether the PTH level being measured is the active or one of the inactive fractions of PTH. In patients with advanced CKD, normochromic, normocytic anemia is almost universal, principally due to another endocrine abnormality, impaired production of erythropoietin by the kidney. Anemia can often be detected in patients with stage 2 CKD who have lost 50% or more of their GFR and have serum creatinine values that are just outside of the normal range. Erythropoietin is produced by interstitial cells in the kidney, and loss of kidney function reduces its production, causing decreased erythropoiesis. Other factors contributing to anemia are a shortened half-life of erythrocytes and vitamin deficiencies. Fortunately, administration of the recombinant hormone erythropoietin eliminates the anemia of CKD. This is therapeutically important because correction of anemia can suppress the development of left ventricular hypertrophy and other factors that contribute to the cardiovascular disease that is so prevalent in CKD patients. The major reasons for an impaired response to erythropoietin are iron deficiency and inflammation, and these should be corrected to achieve optimal responses to erythropoietin therapy ( Chapter 160 ). Accumulation of Uremic Toxins The protein in protein-rich foods is metabolized to amino acids that can be used to build body protein stores ( Fig. 131-2 ). The other fate of amino acids is the formation of urea and other potentially toxic products that must be excreted. Besides amino acids, protein-rich foods contain phosphates, sodium, potassium, acid, and other ions that must be eliminated. The principal nitrogen-containing waste product derived from protein metabolism is urea. When a patient is in protein balance, the net production of urea is directly proportional to the amount of protein in the diet; but if a patient is in negative nitrogen balance, urea and other waste products and ions arise from the breakdown of the body stores of protein. It follows that treatment should be directed at maintaining neutral protein balance at the lowest rate of urea production. More than 135 years ago, it was noted that symptoms of uremia in patients with advanced CKD are ameliorated by reducing the amount of protein in the diet. FIGURE 131-2 Breakdown of dietary protein enlarges the pool of essential and nonessential amino acids that can be used to synthesize body protein. The amino acids are also used to produce urea, which must be excreted. Besides nitrogenous waste products, dietary protein catabolism yields inorganic ions that must be excreted. The consequences of accumulating ions and uremic toxins include the development of symptoms and problems that involve several organs, including the nervous system, the gastrointestinal system, and the skin ( Table 131-5 ). For example, phosphate accumulation leads to secondary hyperparathyroidism and bone disease (see earlier discussion). Acid accumulation contributes to the bone disease of CKD but also stimulates the breakdown of muscle protein and contributes to hypoalbuminemia. Accumulation of peptides, also known as middle molecules, is associated with disorders that range from anorexia to neurologic abnormalities. Accumulation of indoxyl sulfate, a product of tryptophan metabolism, has been linked to progressive kidney damage; guanidine-containing compounds are associated with neurologic damage. Ideally, the levels of these uremic toxins should be monitored, but measuring the levels of individual products is complicated and impractical. The production of urea, however, is directly proportional to the production of other waste products because urea is the principal end product of protein metabolism (see Fig. 131-2 ). For this reason, the production of all waste products is approximated by the 24-hour excretion of urea nitrogen as long as the patient is in the steady state (i.e., the serum urea nitrogen [SUN] concentration and body water are stable). The corollary is that the production of urea should be kept to a minimum that is consistent with maintaining body protein stores (see later). TABLE 131-5 -- UREMIA RESULTS FROM THE DYSFUNCTION OF MANY ORGANS SUGGESTING GENERALIZED TOXICITY Affected System Cause or Mechanism Clinical Syndrome Systemic Anemia, inflammation Fatigue, lassitude Hyperparathyroidism, Rash, pruritus, metastatic calcification symptoms Skin calcium-phosphate deposition Cardiovascular Hypertension, anemia, disease homocysteinemia, vascular Atherosclerosis, heart failure, stroke calcification Serositis Unknown Pericardial or pleural pain and fluid, peritoneal fluid Gastrointestinal Unknown Anorexia, nausea, vomiting, diarrhea, gastrointestinal tract bleeding Immune system Leukocyte dysfunction, Infections depressed cellular immunity Endocrine Neurologic Hypothalamic-pituitary axis Amenorrhea, menorrhagia, impotence, dysfunction oligospermia, hyperprolactinemia Unknown Neuromuscular excitability, cognitive dysfunction progressing to coma, peripheral neuropathy (restless leg syndrome or sensory deficits) Progression of Chronic Kidney Disease Persistence of diseases affecting the kidney (e.g., diabetes or inflammatory conditions such as systemic lupus erythematosus) is one factor in the progression of CKD, but other mechanisms progressively damage the kidney in most CKD patients even when the disease that initially damaged the kidney is no longer active. Mechanisms that have been associated with progression of CKD include kidney damage from systemic hypertension, hemodynamic injury to the kidney, proteinuria, and nephrotoxic injury. Hypertension is suspected to cause progressive loss of kidney function (i.e., progression of CKD) for several reasons. First, hypertension alone can damage the kidney; malignant hypertension damages the endothelial cells of the afferent arteriole and the glomerulus and can even cause thrombosis in these vessels. Second, chronic hypertension is frequently associated with diffuse ischemic injury to the glomerulus and can include collapse of glomerular vessels. The presumed mechanism of progressive kidney damage is direct transmission of the increased blood pressure to the afferent arteriole and the glomerulus, leading to glomerulosclerosis. The degree of hypertension has been directly correlated with the rate of loss of kidney function, and in a multicenter trial, effective treatment of hypertension was associated with slowing of CKD progression. The important question is whether hypertension is a factor contributing to progression or the principal mechanism causing kidney damage. The answer to this question is unsettled. For example, when African American patients with hypertension and kidney disease were studied, progression of CKD continued despite a lowering of blood pressure. Regardless, the close association between the presence of hypertension and the development of cardiovascular diseases mandates control of blood pressure. In multicenter, randomized trials of CKD patients with type 1 or type 2 diabetes or with nondiabetic nephropathy, the major class of drugs with proven effectiveness was the inhibitors of the RAA system, including angiotensin-converting enzyme inhibitors (ACEi) and angiotensin receptor blockers (ARB). The benefits of ACEi or ARB on progression of CKD are additive to their blood pressure–lowering effects. The association between hypertension and progression extends to another proposed mechanism of progressive glomerular damage (see Table 131-4 ). The mechanism is based on preferential constriction of the glomerular efferent arteriole to a greater extent than in the afferent arteriole. This imbalance in arteriolar vasoconstriction increases intracapillary pressure to raise filtration (the hyperfiltration mechanism), but the tradeoff for the increase in GFR is damage to glomerular capillaries. Angiotensin II is the mediator of preferential efferent arteriolar constriction, and experimentally, ACEi or ARB administration can prevent both hyperfiltration and damage to the kidney. The benefits of ACEi or ARB involve more than correction of hyperfiltration. For example, angiotensin II has growth factor properties, and it activates transforming growth factor-β, plasminogen activator inhibitor type 1, and other cytokines, aggravating interstitial damage to the kidney (see Table 131-4 ). It is also suspected that another product stimulated by angiotensin II, aldosterone, contributes to the development of interstitial damage and collagen deposition. Because ACEi and ARB have been demonstrated to slow the loss of kidney function in patients with diabetes and other types of CKD, they should be considered a major strategy to treat progressive CKD. It has been repeatedly demonstrated that ACEi or ARB will reduce albuminuria, presumably by decreasing albumin filtration. This is relevant because experimental evidence suggests that albumin or some component of albumin (e.g., lipids or molecules attached to albumin) is toxic to kidney cells. In these experiments with cultured kidney cells, application of albumin increased the expression of cytokines and damage to the cells. In addition, patients with the greatest amounts of albumin in the urine also have the most rapid loss of kidney function, and when the degree of albuminuria is reduced, the loss of kidney function generally slows. These observations raise the possibility that albumin is a major cause of progressive kidney damage. The shortcoming of focusing on albuminuria as the principal cause of progressive kidney damage is that many kidney diseases initiate albuminuria, and as the kidney damage increases, the degree of albuminuria rises. It is possible, therefore, that reducing albuminuria may simply reflect correction or suppression of the mechanism damaging the kidney rather than blocking the ability of albumin to induce kidney damage. Other proposed mechanisms for progression of CKD can be grouped under a general heading of nephrotoxic damage. It has been known for more than 60 years that animals fed a high-protein diet have more evidence of hypertension and more severe kidney damage, but why this occurs is controversial. Ions or molecules suspected of exerting toxic effects include phosphates and oxalates that lead to deposition of calcium-phosphate or calcium-oxalate salts and toxic responses in the interstitium of the kidney. Other candidates include indoxyl sulfate, generated during the metabolism of the amino acid tryptophan. The mechanisms proposed to explain the toxicity of these ions and compounds include direct damage to kidney cells and stimulation of cytokines (e.g., transforming growth factor-β) and inflammatory pathways that result in damage and fibrosis in the kidney. It has been difficult to assign all of the abnormalities in progressive kidney disease to a single factor. (From: http://www.mdconsult.com/das/book/body/113611082-4/0/1492/501.html?tocnode=54617373&fromURL =501.html#4-u1.0-B978-1-4160-2805-5..50136-1_5573)