Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
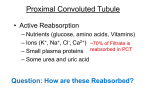
TUBULAR REABSORPTION LEARNING OBJECTIVES: At the end of the lecture, the student should be able to describe : • Tubular reabsorption: An overview • General structure of tubular system • Mechanism of transport • Tubular reabsorption at different renal segments • Effect of tubular reabsorption on concentration of urine • Role of ADH and urea TUBULAR REABSORPTION: OVERVIEW • Tubular reabsorption: occurs as filtrate flows through the lumens of proximal tubule, loop of Henle, distal tubule, and collecting ducts. • Processes used in reabsorption include: – Diffusion – Facilitated diffusion – Active transport – Co transport – Osmosis • Reabsorbed substances are transported to interstitial fluid and reabsorbed into peritubular capillaries. TUBULAR REABSORPTION AND SECRETION: MECHANISMS OF REABSORPTION IN THE PROXIMAL CONVOLUTED TUBULE PERITUBULAR CAPILLARIES: • Blood has unusually high COP here, and BHP is only 8 mm Hg – This favors reabsorption • Water absorbed by osmosis and carries other solutes with it (solvent drag) REABSORPTION OF SALT & H20: • The PCT returns most molecules & H20 from filtrate back to peritubular capillaries – About 180 L/day of ultrafiltrate produced; only 1–2 L of urine excreted/24 hours • Urine volume varies according to needs of body • Minimum of 400 ml/day urine necessary to excrete metabolic wastes (obligatory water loss). PCT: • Filtrate in PCT is isosmotic to blood (300 mOsm/L) • Thus reabsorption of H20 by osmosis cannot occur without active transport (AT) – Is achieved by AT of Na+ out of filtrate • Loss of + charges causes Cl- to passively follow Na+ • Water follows salt by osmosis. GLUCOSE & AMINO ACID REABSORPTION: • Filtered glucose & amino acids are normally 100% reabsorbed from filtrate – Occurs in PCT by carrier-mediated cotransport with Na+ • Transporter displays saturation if ligand concentration in filtrate is too high – Level needed to saturate carriers & achieve maximum transport rate is transport maximum (Tm) – Glucose & amino acid transporters don't saturate under normal conditions. • TUBULAR MAXIMUM TM: Defined as • Maximum rate at which a substance can be actively absorbed – Each substance has its own tubular maximum – Normally, glucose concentration in the plasma (and thus filtrate) is lower than the tubular maximum and all of it is reabsorbed. – In diabetes mellitus, tubular load exceeds tubular maximum and glucose appears in urine. – Urine volume increases because glucose in filtrate increases osmolality of filtrate reducing the effectiveness of water reabsorption . SIGNIFICANCE OF PCT REABSORPTION: • ≈65% Na+, Cl-, & H20 is reabsorbed in PCT & returned to bloodstream • An additional 20% is reabsorbed in descending limb of the loop of Henle • Thus 85% of filtered H20 & salt are reabsorbed early in tubule – This is constant & independent of hydration levels – Energy cost is 6% of calories consumed at rest – The remaining 15% is reabsorbed variably, depending on level of hydration MEDULLARY CONCENTRATION GRADIENT: • In order to concentrate urine (and prevent a large volume of water from being lost), the kidney must maintain a high concentration of solutes in the medulla • Interstitial fluid concentration (mOsm/kg) is 300 in the cortical region and gradually increases to 1400 at the tip of the pyramids in the medulla • Maintenance of this gradient depends upon – Functions of loops of Henle – Vasa recta flowing countercurrent to filtrate in loops of Henle – Distribution and recycling of urea DESCENDING LIMB: • Is permeable to H20 • Is impermeable to salt • Because deep regions of medulla are 1400 mOsm, H20 diffuses out of filtrate until it equilibrates with interstitial fluid – This H20 is reabsorbed by capillaries . Ascending Limb LH: • Has a thin segment in depths of medulla & thick part toward cortex • Impermeable to H20 • Permeable to salt • Thick part ATs salt out of filtrate – AT of salt causes filtrate to become dilute (100 mOsm) by end of LH. AT IN ASCENDING LIMB: • NaCl is actively extruded from thick ascending limb into interstitial fluid • Na+ diffuses into tubular cell with secondary active transport of K+ and Cl- . • Na+ is AT across basolateral mem-brane by Na+/ K+ pump • Cl- passively follows Na+ down electrical gradient • K+ passively diffuses back into filtrate COUNTERCURRENT MULTIPLIER SYSTEM: • Countercurrent flow & proximity allow descending & ascending limbs of LH to interact in way that causes osmolarity to build in medulla • Salt pumping in thick ascending part raises osmolarity around descending limb, causing more H20 to diffuse out of filtrate – This raises osmolarity of filtrate in descending limb which causes more concentrated filtrate to be delivered to ascending limb – As this concentrated filtrate is subjected to AT of salts, it causes even higher osmolarity around descending limb (positive feedback) – Process repeats until equilibrium is reached when osmolarity of medulla is 1400. VASA RECTA : • Is important component of countercurrent multiplier • Permeable to salt, H20 (via aquaporins), & urea • Recirculates salt, trapping some in medulla interstitial fluid • Reabsorbs H20 coming out of descending limb • Descending section has urea transporters • Ascending section has fenestrated capillaries. EFFECTS OF UREA: • Urea contributes to high osmolality in medulla – Deep region of collecting duct is permeable to urea & transports it. OSMOTIC GRADIENT IN THE RENAL MEDULLA: URINE CONCENTRATING MECHANISMS: COLLECTING DUCT (CD): • Plays important role in water conservation • Is impermeable to salt in medulla • Permeability to H20 depends on levels of ADH. ADH: • Is secreted by posterior pituitary in response to dehydration • Stimulates insertion of aquaporins (water channels) into plasma membrane of CD • When ADH is high, H20 is drawn out of CD by high osmolality of interstitial fluid – & reabsorbed by vasa recta. FORMATION OF CONCENTRATED URINE: • ADH-dependent water reabsorption is called facultative water reabsorption • ADH is the signal to produce concentrated urine • ADH stimulates formation of aquaporins in membrane of tubule cells. Increases water reabsorption from filtrate • The kidneys’ ability to respond depends upon the high medullary osmotic gradient. THANKS