Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
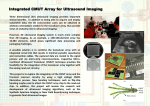
The future of vascular ultrasound RAD Magazine, 39, 456, 22 Professor N D Pugh Consultant medical physicist Dr R J Morris Principal medical physicist University Hospital of Wales, Cardiff email: [email protected] The advent of Duplex scanners in the late 1970s and early 1980s enabled, for the first time, the measurement of blood flow velocity from specific areas within blood vessels. This in turn allowed more accurate assessment of the degree of stenosis/occlusion. The further development of colour flow scanners in the late 1980s and early 1990s moved vascular ultrasound on to become the front-line investigative technique for vascular assessment. Since that time there have been significant advances in medical ultrasound hardware and software that have improved quality and resolution of B-mode and colour flow to greatly enhance their clinical usefulness. As computer speed and power increase rapidly, it is probable that some of the current emerging technologies will develop to have as big a clinical impact as colour flow and Duplex. This article gives a brief summary of newer imaging techniques, and their potential for development in vascular ultrasound. Contrast enhanced ultrasound (CEUS) is one of the oldest of the ‘new’ technologies. It has not yet become a widespread or routine technique, but has undergone resurgence in recent years. Microbubble contrast agents are used to depict low volume flow and perfusion, on the principle of increased backscatter and resonance from tiny encapsulated bubbles of gas that are injected into the body. It is a safe and easy technique, providing one has the appropriate equipment, as most common techniques require contrastspecific software. It also has benefits over other perfusion imaging methods, as it does not involve ionising radiation, and has no nephrotoxicity. Several different imaging protocols are available, employing pulse inversion and harmonic techniques. Contrast is currently used in echocardiography (myocardial contrast echocardiography) and in general radiology for imaging the liver, prostate and breast. Limited use of contrast agents in general vascular ultrasound imaging has been reported,1,2 with further potential in areas such as EVAR (endovascular aneurysm repair) surveillance3 (figure 1) and the identification of adventitial and intra-plaque angiogenesis (vasa-vasorum).4,5 Another ultrasound development that has been available for some time, but has not yet found an essential clinical application, is 3D/4D scanning. First described in the mid 1980s, it became commercially available in the mid 1990s, and mostly found use in obstetrics. Three-dimensional data blocks are produced simply by sweeping a 2D beam through a volume of tissue. The most significant recent development has been the replacement of mechanical sweeping by electronic sweeping with 2D array transducers. These matrix transducers, by imaging the three imaging planes simultaneously, also have the capability of displaying these orthogonal views together in real time. This should speed workflow and reduce transducer manipulation to minimise repetitive Figure 1 Patient with an expanding aneurysm sac following EVAR. CEUS showing a small type III endoleak (hole in graft material) that was not detected on CT. Figure 2 3D ultrasound showing multi-slice views of an aortic aneurysm. strain injuries. The applications to vascular ultrasound are not yet established, but acquisitions of volume data can produce series of cross sectional B-mode images, similar to CT and MR, which has been used in AAA screening6 (figure 2). Three-dimensional and 4D imaging could have a role in carotid scanning, particularly in measuring lumen diameters, and in allowing complete archiving and remote reporting of scans. A weakness in using 3D in vascular ultrasound to develop ‘ultrasound angiography’ is that colour flow cannot be reproduced usefully within the greyscale data set. At the moment there is a problem in the way the data is collected due to the cardiac cycle. Each part of the 3D volume is acquired during different parts of the cardiac cycle so that there will be incomplete colour filling in arteries. Solutions would involve some form of cardiac gating, or selecting data at peak systole. A general problem with colour flow is that conventionally it has poorer resolution than B-mode due to longer pulse lengths. Broadband Doppler (such as Advanced Dynamic Flow – Toshiba Medical Systems)7, and direct visualisation of moving blood cells in B-mode (B-flow – GE Medical Systems) overcome spatial resolution artefacts.8 These methods have great advantages in the assessment of stenoses (figure 3) as they improve the display of surface character- istics and flow channels, which allows more reliable measurement of the stenosis extent. In vascular imaging, the counterpart to improvements in the visualisation of flow are improvements to the imaging of surrounding tissue. The quality and resolution of B-mode has developed with upgrades in transducer and scanner technologies. Nevertheless, it is still generally true in ultrasound that, however good the quality of the image, the ability to distinguish different tissue types will rely on the experience and training of the operator. Several attempts have been made over many years to produce automated systems that can distinguish between cyst, haematoma, calcification, lipid, etc, and code those differences on an image. Ideally, this would allow assessments to be made of the likely presence of disease within tissue during a scan, or to determine the composition of a specific lesion. Elastography is an established tissue characterisation technique based on the measurement of local tissue deformation in response to some sort of applied mechanical stress. Although requiring some assumptions about the physical properties of the tissue, it gives a more quantitative measure of stiffness than manual palpation, together with a strain map. Current clinical applications are in the assessment of the breast, liver and prostate. From a vascular perspective, intravascular elastography can be used in plaque characterisation, using changes in intra-luminal pressure to produce the stress.5 The strain image shows areas of high strain in soft areas and low strain in calcified regions. A future development in vascular imaging may be to perform venous elastography to assess the age of venous thrombus. Acoustic Structure Quantification is a tissue characterisation package developed by Toshiba Medical Systems for use in liver assessment. Changes in the probability density function of the echo signal between normal and fibrotic tissue are used to produce quantitative data and to colour-code B-mode images. This approach may again be applicable in vascular ultrasound to investigate plaque morphology and thrombus age. Characterisation of tissue would automate the assessment of disease currently confined to the subjective assessments of experienced users. A further approach is to make vascular imaging more accessible to interpretation by nonspecialists. Perspective volume rendering (Fly Thru – Toshiba Medical Systems) displays a 3D volume data set in a way that allows interrogation of the interior surface of cavities, ducts and blood vessels. Cross-sectional ultrasound data is added to the plane surface data to enable the user to ‘fly through’ a cavity or vessel, viewing the interior surface of the cavity. This has the potential, with refinement, to aid in the visualisation of the surface characteristics of plaque and the friability of thrombus (figure 4). The future of vascular ultrasound indicated by these emerging techniques is both to enhance the quality of information available to the operator, and to provide new diagnostic information for clinicians. None of these will move from limited or experimental use to become normal and routine parts of a scan until they can be shown to improve the quantification of vascular disease, or to reduce current subjective limitations. However, as these methods clearly show potential in this direction, they will only be adopted more widely if we make the effort to put them into practice and report on their usefulness. References Figure 3 Conventional colour flow (left) and Toshiba Advanced Dynamic Flow images (right) of a significant carotid stenosis. The improved spatial resolution of the Advanced Dynamic Flow overcomes the ‘bleeding artefact’ associated with conventional colour flow imaging and allows for better measurement of degree of stenosis and assessment of plaque morphology. Figure 4 1, Duerschmied D, Maletzki P, Freund G, Olschewski M, Bode C, Hehrlein C. Success of arterial revascularization determined by contrast ultrasound muscle perfusion imaging. J Vasc Surg 2010;52:1531-36. 2, Clevert D A, Sommer W H, Zengel P, Helck A, Reiser M. Imaging of carotid arterial diseases with contrast-enhanced ultrasound (CEUS). Eur J Radiol 2011;80:68-76. 3, Dill-Macky M J, Wilson S R, Sternbach Y, Kachura J, Lindsay T. Detecting endoleaks in aortic endografts using contrast-enhanced sonography. Am J Roentgenol 2007;188:W262-68. 4, Feinstein S B. Contrast ultrasound imaging of the carotid artery vasa vasorum and atherosclerotic plaque neovascularization. J Am Coll Cardiol 2006;48:236-43. 5, de Korte C L, Hansen H H, van der Steen A F. Vascular ultrasound for atherosclerosis imaging. Interface Focus 2011;1:565-75. 6, Nyhsen C M, Elliott S T. Rapid assessment of abdominal aortic aneurysms by 3-dimensional ultrasonography. J Ultrasound Med 2007;26:223-26. 7, Heling K S, Chaoui R, Bollmann R. Advanced dynamic flow – a new method of vascular imaging in prenatal medicine. A pilot study of its applicability. Ultraschall Med 2004;25:280-84. 8, Clevert D A, Rupp N, Reiser M, Jung E M. Improved diagnosis of vascular dissection by ultrasound B-flow: a comparison with color-coded Doppler and power Doppler sonography. Eur Radiol 2005;15:342-47. Toshiba Fly Thru images of a normal carotid artery (right) and a carotid artery with significant intraluminal plaque (left). Fly Thru allows surface rendering of the plaque and the potential for assessing plaque morphology.