Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Pharmaceutical industry wikipedia , lookup
National Institute for Health and Care Excellence wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription costs wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Adherence (medicine) wikipedia , lookup
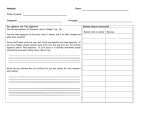
Bone Morphogenetic Protein Prescription Chart for use in Orthopaedics and Neurosurgery Allergies and Adverse Drug Reactions – List the medicines or substances & the nature of the reaction (write NKDA if none) It is mandatory to complete this section Medicine / Substance First Name: Surname: Hospital No: Reaction DOB: NHS No: Sample only - not for clinical use Sign (NAME) Date Sign (NAME) Allergy status unconfirmed. Authority to administer medicines ceases after 24 hours. Consultant: Theatre Hospital: Time & Date USE ORIGINAL CHARTS ONLY - DO NOT PHOTOCOPY Has patient previously been given bone morphogenetic protein? Y / N PRESCRIPTION Date required Drug (Please delete one not required) Eptotermin alfa BMP7 Osigraft® Eptotermin alfa BMP7 Opgenra® Dibotermin alfa BMP2 Inductos® Signature ADMINISTRATION Prescriber (Consultant only) Pharm Batch number/ sticker Administered by: Signature Signature PRINT name & contact details PRINT name & contact details Witness PRINT name & contact details Signature Signature PRINT name & contact details PRINT name & contact details Witness PRINT name & contact details Signature Signature PRINT name & contact details PRINT name & contact details Witness PRINT name & contact details Licensed indications Eptotermin alfa Osigraft - Treatment of non-union of tibia of at least 9 months duration, secondary to trauma, in skeletally mature patients, in cases where previous treatment with autograft has failed or use of autograft is unfeasible. Opgenra - Posterior lateral infusion Dibotermin alfa 1. As a substitute for autogenous bone graft in adults requiring single level (L4-S1) anterior lumbar spine fusion for degenerative disc disease, who had have at least 6 months non-operative treatment (licensed Indicator). 2. Treatment of acute tibia fractures in adults, as an adjunct to standard care using open reduction and intramedullary nail fixation. Instructions 1. This prescription should be sent to Advanced Clinical Pharmacist (ACP) for Orthopaedics/Neurosurgery at least 2 full working days before it is required. 2. Vials must only be used for the named patient, any unused vials MUST be returned to Pharmacy immediately the operation is concluded. 3. Please document the batch numbers of the vials used on this chart and ensure the chart is filed in the patients’ notes. Pharmacy Staff Please send this chart with the order to the relevant theatre. If the Advanced Clinical Pharmacist (ACP) for Orthopaedics/Neurosurgery is unavailable, please supply the requested item and leave a copy of the prescription request for the attention of the ACP. Registered by Medicines Risk Management Group Reviewed & re-registered Next review Pharm Ref No. June 2011 March 2014 March 2016 11/006 v3 For further supplies please contact your Ward Pharmacist.