Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
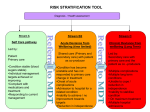
Sickle Cell Disease Introduction • Vaso-occlusive phenomena and hemolysis are the clinical hallmarks of Sickle Cell Disease (SCD) • Inherited disorder due to homozygosity for the abnormal hemoglobin, hemoglobin S (HbS) • HbS results from substitution of valine for glutamic acid as sixth amino acid of the beta globin chain, which produces a hemoglobin tetramer that is poorly soluble when deoxygenated. • Polymer assumes elongated rope-like fiber form in the classic sickle shape • Sickle cell shape results in decrease cell deformability. • Changes also occur in red cell membrane structure and function, disordered cell volume control and increase adherence to vascular endothelium. Overview • Disorder most severe in patients with SCD (homozygosity for HbS), of intermediate severity in hemoglobin SC disease (HbSC, combined heterozygosity for hemoglobin S & C), and generally benign in those with sickle cell trait (heterozygosity for Hbs). • Patients with homozygous SCD are typically anemic and often lead a life of painful episodes. • Clinical signs and symptoms begin at an early age. Prevalence of symptoms at age • • • • • Six month of age - 6% Twelve months of age - 32% Two years of age - 61% Six years of age - 92% eight years of age - 96% Predictors of adverse outcome • • • • Dactylitis before age one Hemoglobin concentration < 7 g/dl Leukocytosis in absence of infection An adverse outcome, defined as stroke, frequent episodes of pain, recurrent acute chest syndrome or death occurred in 18% with these predictors,(392 infants/10yrs). Laboratory findings • • • • Moderate anemia Reticulocytosis 3-15% High MCV Unconjugated hyperbilirubinemia • Elevetaed LDH • Low haptoglobin • Folate & iron deficit • Peripheral smear shows sickle cells • Polychromasia • Howell-jolly bodies • Elevated WBC • Elevated Platelets • Low than after 18 yrs high creatinine Acute Severe Anemia • Acute fall in haptoglobin. • Patients present with pallor, weakness and lethargy. • Fatalities not uncomon. • Due to the Splenic sequestration crisis, aplastic crisis or hyperhemolytic crisis. Splenic sequestration crisis • Vaso-occlusion in the spleen and pooling of blood in the spleen produce fall in hemoglobin, reticulocytosis and rapidly enlarging spleen. • Risk of hypovolemic shock and 10-15% mortality. • Recurrent in 50% of survivors. Aplastic crisis • Arrest of erythopoiesis with falling hemoglobin levels and absence of reticulocytes. • Associated with infection namely ParvoB19, EBV, Streptococcus and salmonella. • Reticulocytes usually reappear in 2-14 days. Hyperhemolytic crisis • Sudden exacerbation of anemia with reticulocytosis. • Cause unknown. • Rare Major Clinical Manifestations • • • • Acute painful episodes Multiorgan failure Psychosocial issues Growth & development • Infection • Bacteremia • Meningitis • • • • • • • • Bacterial pneumonia Osteomyelitis CVA Bone complcations Infarct and necrosis Marrow infarct Orbital compression Arthritis Major Clinical Manifestations • Cardiac complications • Myocardial infarct • Dermatologic complications • Leg ulcers • Hepatobiliary complications • Cholelithiasis • Chronic liver disease • Acute hepatic episodes • Pregnancy complications • Fetal complications • priapism • Pulmonary complications Major Clinical Manifestations • Renal complications • Retinopathy • Take a deep breath! Acute painful crisis • Precipitated by cold, infection, dehydration, infection, stress, menses, hypoxemia, alcohol or no identifiable cause. • Can affect any area, but back, chest, extremities and abdomen most frequent. • Usually last 2-7 days. • Frequency- 1/3 rarely, 1/3 2-6yr, 1/3>6yr Acute chest syndrome • Due to pneumonia, infarct due to in situ thrombosis and embolic phenomena due to fat embolism and bone marrow infarct. • Manifestations are chest pain, infiltrate on CXR and fever. • Treat with O2, antibiotics, and exchange transfusion to lower HbS to below 30%. Management • Treatment and prevention of the acute manifestations of SCD. • Therapies designed to interfere with the polymerization process at different levels General principals • Regular Physician follow up. • Establish base line labs and Physical findings. • Education regarding nature of disease, genetic counseling and psychosocial assessment. • Immunize for Strep, influenza and Hep B • • • • • • Prophylactic penicillin until five years. Folic acid 1md/day TCD Retinal evaluation BCP Hydroxyurea Hdroxyurea • Increases production of hemoglobin F. • Reduces median crisis rate by 50%, decreased acute chest syndrome and transfusion. • 40% reduction in mortality. • Mild increase in acute myeloid leukemia Pain management • • • • • Narcotics - Morphine or dilaudid Toradol Inhaled nitric oxide anticoagulation low dose INR 1.5 Poloxamer 188 Management of infection • Prophylactic fever - Ceftriaxone • Acute chest syndrome - Cefuroxime & Erythromycin. • Osteomyelitis - Cover salmonella and staph until cultures available. Transfusion therapy • • • • • • • Aplastic crisis Acute chest syndrome or sepsis CVA Priapism Perioperative Simple vs exchange Do not raise Hgb > 10 Prophylactic preoperative transfusion • Increase hemoglobin to 10g/dl • Reduces serious complications • Orthopedic surgery still has 67% serious complications and 17% sickle-related Complications ( acute chest syndrome and vaso-occlusive crises ) Transfusion complications • Alloimmunization • Iron overload • Infection Prognosis • Median age of death for SCD in males is 42 for men and 48 for women • Median age of death for Hb SC is 60 for men and 68 for females Causes of death • • • • • • • Infection - 48% Stroke - 10% Complications of therapy - 7 % Splenic sequestration - 7 % Thromboembolism - 5% Renal failure - 4 % Pulmonary hypertension - 3 % The future • • • • Gene therapy Increase expression of Hb F RNA repair Hematopoietic cell transplantation