Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Thalamus and connections
An anatomical journey
Sam Terman
January 30, 2017
• I have no disclosures.
• “You are a masochist and a true American.”
Objectives
• Describe the development, structure, and function of the thalamus
and its connections
• Recognize disease processes affecting the thalamus
Outline
• Significance
• Development
• Gross anatomy
• Nuclei organization
• Vascular supply
• Disease states
Significance
• “Inner chamber” or “bedroom”
• Multimodal processing station (i.e….it does more than you think)
• Sensory
• Motor
• Cerebellum
• Basal ganglia
•
•
•
•
Limbic and motivation
Arousal, alertness, and sleep-wake cycles
Cognition
Language
• Thalamus <-----------> Cortex
Development
Development
Development
• The prosencephalon divides into the diencephalon and the
telencephalon. The diencephalon gives rise to, among other
structures, the thalamus, globus pallidus, and hypothalamus. The
telencephalon gives rise to the striatum and cerebral cortex.
Gross Anatomy
Gross anatomy
Gross anatomy
• Connected by the massa intermedia
Nuclei organization
• Relay (most of the thalamus)
•
•
•
•
Lateral
Medial
Midline
Anterior
• Intralaminar
• Reticular
What goes in…
…must come out
• Fill in the blank: Most thalamocortical fibers project to layer __ of
neocortex.
“Layer IV contains a dense horizontal band of fibers--the
external band of Baillarger. This band contains the terminal
ramifications of the thalamocortical projections from specific
thalamic relay nuclei. It is particularly prominent in the
striated or primary visual cortex and known as the line of
Gennari.”
Most thalmocortical fibers project to layer IV
Nuclei organization - Lateral
•
•
•
•
•
•
•
•
•
•
•
VPL (somatosensory spinal = body)
VPM (somatosensory cranial nerve = face, taste)
LGN (vision, “lateral light”)
MGN (hearing, “medial music”)
VL (from basal ganglia/cerebellum, RITE prefers cerebellum)
VA (from basal ganglia)
Pulvinar (behavioral orientation towards stimuli (i.e. visual), to diffuse
association cortex)
Lateral dorsal (like an anterior nucleus, multimodal)
Lateral posterior (like pulvinar)
Ventral medial (alertness)
VIM (DBS target for ET)
Nuclei organization - Lateral
VPM
VPL
Nuclei organization - Lateral
• Facial pain, thermal sensibility, fine touch and position sense all converge
for the first time in the ventroposterior medial nucleus of the contralateral
thalamus. The chief sensory nucleus of cranial nerve V serves fine touch,
the spinal nucleus of cranial nerve V serves pain and thermal sensibility
and the mesencephalic nucleus of cranial nerve V serves position sense.
These sensory modalities converge in the contralateral thalamus in the
ventroposterior medial nucleus of the thalamus while sensory information
from the contralateral trunk and extremities converges on the
ventroposterior lateral nucleus of the thalamus.
• The ventral posterolateral nucleus projects to areas three, one, and two-the primary somesthetic area of the parietal lobe. The
ventroposteromedial nucleus, that conveys facial sensation, also projects
to the postcentral gyrus.
What structure?
LGN
• LGN: convex shape
(Napoleon's hat)
• L = “Light” (vision)
• Tract -> LGN -> Radiations > cortex
LGN
• Extra credit: How is the LGN organized?
LGN
• Each thalamus contains information from the contralateral hemifield
• Layers alternate visual information
• Layers 1 and 2 = magnocellular (rods, movement)
• Layers 3 to 6 = parvocellular (cones, color)
• In between = koniocellular (color, movement, integration, ?)
• Layers alternate eyes
• Layers 2, 3, 5 = ipsilateral thalamus
• Layers 1, 4, 6 = contralateral thalamus
LGN
LGN
Extrageniculate visual pathways
• Pretectal area -> parasympathetics (pupillary light reflex)
• SCN (circadian rhythms)
• Superior colliculus (orient eyes and head to stimuli, saccades) ->
pulvinar and lateral posterior nucleus -> association cortex (FEF, parietal) for
visual attention and orientation
• Superior colliculus -> tectospinal tract (reflex postural movements in response
to visual stimuli) -> C1-C4
MGN
• Medial = “music”
MGN
• What is the input to MGN?
MGN
• What is the input to MGN?
• Inferior colliculus
MGN
Don’t get confused
• Olives
• Superior olive = hearing
• Inferior olive = cerebellum
• Colliculi
• Inferior colliculus = hearing
• Superior colliculus = vision
• Lemniscus
• Lateral lemniscus = hearing
• Medial lemniscus = somatosensation
Pulvinar
• The pulvinar is an association nucleus in the thalamus involved in
visual processing. The pulvinar receives fibers from the superior
colliculus (extrageniculate) and projects to areas 17, 18 and 19. Both
the inferior and lateral pulvinar have reciprocal connections with the
occipital cortex.
• Very close to LGN
Insula
• Insular cortex receives inputs from the ventromedial nucleus of the
thalamus, relaying taste and visceral sensation. In addition, it receives
nociceptive and thermal inputs from the posterior ventromedial
nucleus, which is the site of termination of spinothalamic pathways
arising from lamina I of the dorsal horn.
Exception
• What sensory modality doesn’t project to thalamus en route to
primary cortex (hint: what haven’t we talked about?)
•
•
•
•
•
A) Somatosensation
B) Taste
C) Sight
D) Sound
E ) Smell
Exception
• Olfactory neurons project directly
to (allo)cortex without synapsing in
thalamus
• That said, thalamus still processes
olfaction (i.e. olfactory cortex ->
MD)
VA/VL
• Inputs are
basal ganglia
and
cerebellum
VA/VL
• Output to frontal/motor cortex
Basal ganglia output to thalamus
• Basal ganglia has 4 parallel channels
•
•
•
•
Motor
-> VA/VLo
Oculomotor -> VA/MD
Prefrontal -> VA/MD
Limbic
-> VA/MD
• Also output to intralaminar (centromedian, parafascicular) nuclei ->
back to striatum
Basal ganglia outputs to thalamus
• SNr/GPi -> thalamic fasciculus (AL + LF) -> thalamus (VA/VL) -> frontal
lobe
• Nomenclature 1: AL+LF = TF
• Ansa lenticularis (loop around IC)
• Lenticular fasciculus (plow through IC)
• Nomenclature 2:
• H fields of Forel (white dead guy, H=‘hood’)
• H1 field of Forel = thalamic fasciculus
Unrelated, but testable and in the neighborhood
• What is the
only
excitatory
connection in
the basal
ganglia classic
model?
Cerebellum output to thalamus
• Cerebellum ->
VLc ->
premotor
cortex
Nuclei organization - Medial
Nuclei organization - Medial
Nuclei organization - Medial
• MD
• Limbic, executive function, behavior, motivation
• Amygdala/olfactory cortex/limbic/prefrontal cortex/basal ganglia -> MD ->
frontal cortex
• The medial dorsal nucleus of the thalamus has rich connections with the
amygdala, orbitofrontal region, and the temporal lobe. Lesions involving this
nucleus typically involve disinhibition, utilization behavior, mania, and
memory loss.
• Motivation pathway: cingulate gyrus -> limbic striatum (ventral caudate,
nucleus accumbens, olfactory tubercle) -> MD -> cortex
Nuclei organization - Anterior
Nuclei organization - Anterior
Nuclei organization - Anterior
• Anterior nucleus
• Limbic
• Mammillary body/hippocampal formation (mammillothalamic tract, Papez
circuit) -> anterior n. -> cingulate gyrus
• Lesions -> amnesia, confabulation, anomia.
• The lateral dorsal nucleus has connections similar to those of the anterior
nucleus to which it is adjacent though it may also have posterior parietal
connections as well.
Nuclei organization - Midline
• Midline thalamic nuclei
• Limbic, diffuse
• Hyopthalamus/basal forebrain/amygdala/hippocampus -> midline nuclei
amygdala/hipoccampus/limbic cortex
Nuclei organization - Intralaminar
• Intralaminar nuclei
• Alertness/consciousness, motor relay for basal ganglia and cerebellum
• Deep cerebellar nuclei, globus pallidus, ARAS, sensory pathways ->
intralaminar nuclei -> cortex and striatum
• I.e. inputs and outputs are to/from basal ganglia
• Caudal: (including large centromedian nucleus): basal ganglia circuitry
• Rostal: Basal ganglia circuitry, but also relay inputs from ARAS to cortex to
maintain alertness
• The intralaminar nuclei are cell groups within the internal medullary lamina,
which separates the medial and lateral subdivisions of the thalamus. Its
afferents are from nuclei in the brainstem reticular formation and
somatosensory input, and has diffuse cortical projections
Nuclei organization - Reticular
Nuclei organization - Reticular
• Reticular nucleus
• Thin sheet just lateral to the rest of the thalamus, separated by the external
medullary lamina
• NOT synonymous with the brainstem reticular formation, but connected to
ARAS so involved in alertness
• Regulates state of other thalamic nuclei by inhibitory neurons and alertness
• Only nucleus which doesn’t project to cortex
• Cortex, ARAS, intralaminar nucleus -> reticular nuclei -> intralaminar nuclei,
ARAS
Nuclei organization - Reticular
• Generates sleep
spindles
Nuclei Review
• VPM v VPL (face versus body?)
• MGN (input?) v LGN (Waterloo?)
• VA v VL
• MD v anterior (which one relays info hippocampus/Papez ->
cingulate?)
• What modality doesn’t pass through thalamus en route to cortex?
• What’s interesting about reticular (2 things)?
• What sensory modality comes up most with the pulvinar?
Vascular supply
4
1
4
3
2
Vascular supply
• Mostly posterior circulation
• Four major arteries
• Tuberothalamic (polar)
• From Pcomm
• Anterior thalamus, especially VA
• Thalamoperforating (paramedian)
• From P1
• Medial thalamus, especially DM
• Thalamogeniculate
• From P2
• Lateral thalamus, including VL
• Posterior choroidal
• From P2
• Posterior thalamus such as pulvinar
• Tiny anterior circulation supply (not pictured)
• Anterior choroidal artery
• From ICA
• Posterior limb of internal capsule and lateral thalamus
Vascular supply
• The thalamoperforating branches of the posterior cerebral arteries
perfuse the medial and anterior regions of the thalamus. The
thalamogeniculate branches of the posterior cerebral arteries perfuse
the pulvinar and lateral nuclei. The inferior thalamic arteries arise
from the posterior communicating arteries and perfuse the inferior
portions of the thalamus. The medial posterior choroidal artery
supplies the superior and medial portions of the thalamus.
Disease states
• Vascular
• Drug mechanism
• Prion
• Metabolic
• Movement
Vascular: Lacunar syndrome
• Pure sensory lacunar syndrome
• Dejerine Roussy syndrome
Vascular: Artery of percheron
• Unilateral proximal PCA feeds bilateral paramedian thalami and
rostral midbrain ….. zzzzzzzzz
Vascular: Aphasia
• “Paramedian infarcts of the thalamus can result in language disorders
that resemble transcortical motor however there are more paraphasic
errors and patients are slightly more fluent than a typical transcortical
motor aphasia. Other common symptoms include behavioral changes
and amnesia.”
An 83-year-old right-handed woman presented with sudden right-sided hemiparesis, somnolence, and loss of normal speech. Speech was nonfluent with semantic paraphasias and wordfinding difficulties. Word repetition and comprehension were normal. MRI brain showed an area of restricted diffusion in the left thalamus consistent with acute infarction (figure 1). Speech
fluency returned to normal after 2 days with occasional dysnomia and paraphasias. Left thalamic infarcts can result in aphasia that is characterized by lexical-semantic deficits and intact word
repetition; fluency and comprehension are variably affected.1 Thalamic aphasia has been hypothesized to result from disconnection between cortical language centers and thalamic nuclei
(figure 2).1,2. –Teaching NeuroImages Thalamic aphasia syndrome. Afzal U and Farooq MU, Neurology 2013;81;e177. http://www.neurology.org/content/81/23/e177.full.pdf
Vascular: Anterior choroidal
• Branch of ICA
• Posterior limb of IC and lateral
thalamus
• Hemiparesis and quadruple
sectoranopia
Vascular: infarct-related dementia
• Apparently a lesion of 0.5 cm in the MD is capable of producing a
dementia since it is capable of disrupting the encoding circuit
(producing an amnesia) and also the frontal-subcortical circuits
(producing profound executive and behavioral dysfunction).
Vascular: Susac
• Susac syndrome is a clinical triad of retinal
branch occlusion, hearing impairment, and
MRI changes that resembles multiple
sclerosis. In multiple sclerosis the lesions tend
to be in the forceps and more peripheral
margins of the corpus callosum. Susac
syndrome tends to involve the midline of the
corpus callosum. Other MR abnormalities
seen in Susac syndrome include hyperintense
scattered subcortical T2 lesions,
leptomeningeal enhancement, and focal
lesions in the basal ganglia and the thalamus.
Vascular: Venous infarct
• Sagittal T1 and axial proton density images show abnormal
hyperintensity filling the vein of Galen and straight sinus, instead of
the normal flow void expected. This is secondary to thrombus in
these structures and has resulted in hemorrhagic venous infarction
in the thalami. Mass effect from the infarctions has compressed the
third ventricle, resulting in obstructive hydrocephalus of the lateral
ventricles. The axial image shows prominent basal veins of Rosenthal
(seen on either side of the vein of Galen as flow void), likely providing
collateral venous drainage. The pineal gland is normal in appearance,
but inferiorly displaced by the thrombus and mass effect.
AVM
Vascular: AVM
• There is a large draining vein and nidus of smaller vascular structures
within the right thalamus, with adjacent hemorrhage and mass effect
on the third ventricle. The appearance is that of an arterial venous
malformation. The vein of Galen malformation would extend in the
posterior midline. A venous malformation would have a linear, radial
or caput medusa pattern. A hemangioblastoma may be a cystic or
solid highly vascular tumor however a large vein and vascular nidus as
shown are not associated features.
Vascular: hypoxia
Drug mechanism
• _____ blocks calcium channels in the thalamus.
Drug mechanism
• Ethosuxamide blocks calcium channels in the thalamus.
• “Corticothalamic rhythms are believed to be involved in the generation of
spike-and-wave discharges that are the characteristic
electroencephalographic signs of absence seizures. The spontaneous
pacemaker oscillatory activity of thalamocortical circuitry involves low
threshold T-type Ca2+ currents in the thalamus, and ethosuximide is
presumed to reduce these low threshold T-type Ca2+ currents in thalamic
neurons.” – Ethosuxamide: from bench to bedside, Goren MZ and Onat F, CNS
Drug Rev, 2007 Summer; 13(2):224-39.
What is this?
• Variant CJD
• Rare prion disease typically seen in
younger patients who present with
rapidly progressive cognitive decline (but
less rapid than sporadic CJD), cerebellar
dysfunction, visual disturbance and may
have increased signal intensity lesions on
FLAIR views in the bilateral posterior
thalami ("pulvinar sign").
• Florid amyloid plaque surrounded by rim
of spongiform changes. Tonsillar biopsy
particularly diagnostic.
CJD
• DWI: cortical gyri, caudate, and thalamus.
Diagnosis?
• A 50 year old begins experiencing insomnia followed by several
months of panic attacks and hallucinations. This is followed by
complete inability to sleep, rapid weight loss, unresponsiveness, and
death six months later. His father perished similarly.
Fatal familial insomnia
• Autosomal dominant prion disease
• Involves some atrophy of the thalamus
Wernicke’s encephalopathy
• The location of the T2 hyperintensity in the dorsal midbrain and the
symmetrical abnormal enhancement in the mammillary bodies,
periaqueductal tissue and dorsal midbrain and the FLAIR
hyperintensity in the medial thalami are highly indicative of
________________________ in this clinical setting.
• Question had a negative MRV and MRA (not vascular)
Wilson’s
• There is symmetric high signal intensity involvement of the putamen
and thalami bilaterally. The globus pallidus is also involved but not
exclusively as it is in many patients with carbon monoxide poisoning.
The heads of the caudate and nuclei appear normal, and there is no
significant overall atrophy of the brain. These are findings that tend to
exclude Huntington disease while the high signal intensity within the
globus pallidus and putamen is atypical for Parkinson disease.
Gliomatosis cerebri, an infiltrating astrocytoma of the white matter, is
excluded by the fact that the disease process spares the white matter
where the tumor occurs. The correct response is Wilson disease.
Movement
• Essential tremor
• Lesion part or all of the
thalamus to suppress
contralateral tremor
• DBS of VIM
• Thalamotomy
• Side effect of bilateral
thalamotomy? Speech
Movement
• Ballism
• Associated with discrete lesions in the subthalamic nucleus. The dyskinesia
occurs contralateral to the lesion and is associated with hypotonia. As the
hemiballismus improves, the movements are more like chorea. The
subthalamic nucleus modulates (suppresses) ispilateral basal ganglionic
activity, which in turn modulates cortical motor outflow to the contralateral
effector muscles.
Movement
• STN excites
SNr/GPi,
which
inhibits
thalamus
Movement
• Ballism
Movement
• Ballism
• Associated with discrete lesions in the subthalamic nucleus. The dyskinesia
occurs contralateral to the lesion and is associated with hypotonia. As the
hemiballismus improves, the movements are more like chorea. The
subthalamic nucleus modulates (suppresses) ispilateral basal ganglionic
activity, which in turn modulates cortical motor outflow to the contralateral
effector muscles.
Movement
• Dopamine excites
direct pathway,
and direct
pathway excites
thalamus/cortex
(excite 2
negatives)
• Dopamine inhibits
indirect pathway,
and indirect
pathway inhibits
thalamus/cortex
(inhibits 3
negatives)
Movement
• Q: What’s the
lesion in PD?
• A: SNc
Movement
• DBS:
depolarization
block of STN
(or GPi) for PD
Movement
• Q: What’s the
lesion in HD?
• A: Caudate and
putamen, initially
indirect pathway
more affected
• Later, both
pathways
degenerate, and
rigid/hypokinetic
parkinsonism can
develop (and
parkinsonism
predominates in
the young)
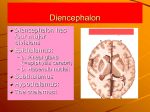
Hypothalamus
• A few recurrent themes
• Sarcoid and NMO enjoy the diencephalon
• Hamartoma = gelastic seizures
• Begin with laughter, precocious puberty may occur, disorganized hypocellular collection
of mature neurons and glia, not cystic (unlike craniopharyngiomas)
• Dopamine = prolactin inhibitory factor
Thalamus and connections
An anatomical journey
Sam Terman
January 30, 2017