Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
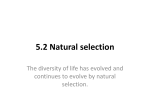
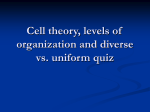
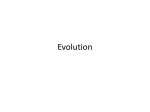
Heart and Circulation Research Article Gestational High-Salt Intake Causes Cardiovascular Dysfunction in Adulthood Satomi Kagota1*, Kana Maruyama1, Bruce N Van Vliet2 and Kazumasa Shinozuka1 Department of Pharmacology, School of Pharmacy and Pharmaceutical Sciences, Mukogawa Women’s University, Japan 2 BioMedical Sciences Division, Faculty of Medicine, Memorial University, Canada 1 *Corresponding author: Satomi Kagota, Email: [email protected] Received: 20 December 2016; Accepted: 24 January 2017; Published: 07 February 2017 Abstract Objective: We have demonstrated that a maternal high-salt intake administered throughout gestation and lactation causes cardiac and vascular dysfunction in offspring of spontaneously hypertensive rats (SHR). The objective of this study was to investigate the influence on arterial and cardiac function of a maternal high-salt diet administered during gestation alone versus during both gestation and lactation. Materials & Methods: SHR were treated with either a maternal 6% NaCl diet or a control (0.3% NaCl) diet during the gestation and suckling periods. A third group was exposed to a high-salt maternal diet during gestation alone. After weaning, the offspring were fed control diet or the high-salt diet for 8 weeks, and then their heart function and vasodilation in aortas and mesenteric arteries were determined at 12 weeks of age by a Langendorff heart perfusion system and myograph methods. Results: Left ventricular systolic and diastolic functions were significantly impaired in 12-week-old offspring of dams fed the highsalt diet during gestation and suckling, irrespective of post-weaning salt intake. Left ventricular function was not altered when high-salt was administered during gestation alone, i.e., restriction of salt intake during suckling was associated with reduced impairment of ventricular function. Offspring of dams fed the high-salt diet during gestation alone had a decreased vasodilatory response to nitric oxide relative to those of control diet-fed dams. The level of impairment was similar to that triggered by a maternal high-salt diet during gestation and lactation, and to that of post-weaning high-salt intake in offspring of the normal diet-fed dams. Conclusions: These results indicate that a maternal high-salt intake during gestation alone is sufficient to trigger vascular dysfunction in offspring, whereas restriction of salt intake during lactation can attenuate the detrimental effects of a maternal high salt intake during gestation on cardiac function. Keywords: Cardiac function; Dietary salt; Fetal programming; Prenatal nutrition physiology; Vascular function Introduction High-salt intake is widely accepted to be associated with significantly increased risk of stroke and cardiovascular diseases [1,2]. A recent systematic review has further added to the evidence of associations of high sodium intake with blood pressure or adverse health outcome including cardiovascular mortality, and supports the current global recommendations for a reduction in dietary salt intake [3]. A variety of mechanisms have been proposed to explain salt-induced alterations of cardiovascular functions. Impairment of vasodilation in Open Access response to nitric oxide (NO) represents one of the potential underlying mechanisms. Dysfunction of vasodilation via the NO pathway has been shown in patients with salt-sensitive hypertension [4,5]. Oral salt loading has been reported to suppress flow-mediated vasodilation (presumably endothelial NO dependent) in healthy subjects [6], and to reduce vascular NO bioactivity in young healthy normotensives [7]. Using experimental animals, high-salt intake (8%NaCl) was found to impair vasodilation in response to NO in spontaneously hypertensive rats (SHR) [8,9], and decreased production of or response to NO in Dahl salt-sensitive hypertensive rats [10,11]. Increasing dietary salt loading (4, 6 and 8% NaCl) in SHR promotes an increase in vascular resistance independent of arterial pressure, leading to renal injury [12]. In contrast, effects of high-salt intake on heart function has also been reported: oral salt loading reduced left ventricular (LV) myocardial relaxation in young healthy normotensives [7] and in young hypertensive patients [13], and salt excess (8%NaCl) led to increased left ventricular mass, myocardial fibrosis, and impairment of LV diastolic function in SHR [14]. On the other hand, cardiovascular structure and function and the risk of developing cardiovascular disease are also influenced by the maternal environment during development, including the maternal diet [15,16]. Fetal exposure to both inadequate maternal diet and maternal over-nutrition have been clearly shown to influence cardiovascular health in later life, and a growing literature points to a similar influence of a maternal high-salt intake [16]. It has been known that increased preference for salt develops during pregnancy in women [17,18]. Our previous study demonstrated that offspring of SHR fed a high-salt diet during gestation and lactation have impaired LV systolic and diastolic dysfunctions and vasodilation in response to NO independent of postweaning salt intake, compared with offspring of SHR fed a control diet. A high-salt intake during pregnancy and lactation has also been demonstrated to increase fibrosis of the arterial wall and decrease expression of soluble guanylyl cyclase (sGC), leading to impairment of vasodilation in response to NO, in aortas of offspring in SpragueDawley rats [19]. In contrast, maternal salt during gestation alone has been found to affect to development of heart structures, probably mediated by the renin-angiotensin system [20,21], but there is very limited information about the effects of maternal high-salt intake on heart function [22]. Furthermore, very few studies have investigated the role of the timing of the exposure to a maternal high-salt diet during gestation and/or lactation. For instance, a high-salt diet neither during conception to lactation nor lactation alone affect heart rates in the borderline hypertensive rat offspring [22], and a high-salt diet during pregnancy alone increased vascular contractility in Sprague-Dawley rat offspring [23]. Therefore, in this study, we compared the degree of the cardiac and arterial dysfunction induced in SHR offspring by a maternal highsalt intake administered during gestation alone with that administered during both gestation and lactation. The findings of the current study may provide insight regarding the most salt sensitive periods of development, and the periods in which salt restriction may provide the greatest protection against development of the cardiac and vascular dysfunction in offspring. Materials & Methods Animals and experimental designs As shown in Figure 1, SHR dams were fed a control (NN, 0.3% NaCl) or high-salt (HH, 6% NaCl) diet ad libitum from 1 week before mating Copyright © 2017 The Authors. Published by Scientific Open Access Journals LLC. Volume 1, Issue 1 Kagota et al. Determination of cardiovascular functions (12 weeks of age) Weaning (4 weeks of age) 1 week before mating Gestation Lactation After weaning Male offspring N Heart Circ 2017; 1:007 N N 14 n h n h NN_n group NN_h group (n = 7) HN_n group HN_h group (n = 7) (n = 7) (n = 7) H H n h HH_n group (n = HH_h group (n = 7) 7) N and n; a standard diet containing 0.3% NaCl H and h; a high salt diet containing 6% NaCl Figure 1: Experimental protocol for salt loading. SHR dams and offspring were given a standard diet containing 0.3% NaCl (N and n) or a high-salt diet containing 6% NaCl (H and h). until weaning at 4 weeks of age. A second experimental group of dams (HN) was fed a high-salt from 1 week before mating until birth, and was then switched to the normal salt diet until weaning. Weaned male offspring were received from Japan SLC, Inc. (Hamamatsu, Japan) at 4 weeks of age, and they were divided into two groups of the same body weight. Offspring were given a standard diet containing 0.3% NaCl (n) or a high-salt diet containing 6% NaCl (h) for 8 weeks, leading to a total of 6 experimental groups: NN_n, NN_h, HN_n, HN_h, HH_n, HH_h group (n = 7 each). Diets were based on a standard rodent chow (MF diet, Oriental Yeast Co., Tokyo, Japan; 7.9% moisture, 23.1% crude protein, 5.1% crude fat, 5.8% crude ash, 2.8% crude fiber, 55.3% nitrogen free extract, supplemented with vitamins and minerals including Ca 1.07 % and K 0.9 %). At 11 weeks of age, offspring systolic blood pressure and heart rate were measured using a photoplethysmographic tail-cuff system (Model MK-2000; Muromachi Kikai Co. Ltd., Tokyo, Japan) without heating, as described previously [24]. At 12 weeks of age, body weight was measured under anesthesia (sodium pentobarbital, 60 mg/kg, i.p.), and then hearts and arteries were removed from each rat. All procedures were performed in accordance with the guidelines for the Care and Use of Laboratory Animals at Mukogawa Women’s University. Measurement of heart function using isolated heart by Langendorff methods Using an isolated Perfused Heart, Working Heart & Langendorff system (IPH-L2A, Primetech Co., Tokyo, Japan), heart function was determined as described previously [24]. Briefly, hearts removed from each rat were immediately perfused with Krebs-Henseleit solution (in mM: NaCl 118.4, KCl 4.7, MgSO4 1.2, CaCl2 2.5, NaHCO3 25, KH2PO4 1.2, and glucose 11.1) saturated with 95% O2 and 5% CO2. A collapsed latex balloon was inserted into the LV cavity and connected to a pressure monitoring kit (SAFTI, Kawasumi Lab., Inc., Tokyo, Japan) coupled to a recorder (8K21, NEC San-Ei, Tokyo, Japan). Hearts were allowed to beat spontaneously at sinus rhythm, and LV developed pressure (LVDP) and the maximum rate of LV pressure decline (-dP/dt) were determined as indices of systolic and diastolic function, respectively. Coronary flow was determined from the Langendorff perfusion system with hearts provided with a constant perfusion pressure of 80 mmHg. Measurement of vasodilation in isolated aortas and mesenteric arteries by myograph methods Vasodilatory function was assessed as described previously [24]. Briefly, aortas and mesenteric arteries removed from each rat were immediately placed in oxygenated Krebs–Henseleit buffer, described above. Ring preparations were contracted by addition of 0.1–1 µM phenylephrine to generate approximately 80% of the maximal contraction. After a stable contraction was obtained, relaxation was elicited using nitroprusside (0.1 nM–1 µM). Individual concentrationresponse curves were analyzed by nonlinear curve fitting of relaxationdrug concentration relationships to determine the negative log EC50 using Graph Pad Prism software (ver. 5.0 for Mac, San Diego, CA, USA). Data analysis Data are expressed as the mean ± SEM. Statistical analysis was carried out with a one-way ANOVA followed by Bonferroni’s post-hoc test (GraphPad Prism software). The results were considered significant when P-values were < 0.05. Results Offspring blood pressure, heart rate, body weight, and heart weight The detailed protocol for salt loading is shown in Figure 1. As shown in Table 1, at 11 weeks of age, one week before determination of vascular and heart functions, systolic blood pressure in offspring of dams fed high-salt diet during gestation and lactation (HH_n) was lower than that in offspring of the control diet-fed dams (NN_n), but did not differ in offspring of dams fed high-salt diet during gestation alone (HN_n). A post-weaning high-salt intake was associated with increased blood pressure in the offspring of dams fed a control diet (NN_h vs. NN_n), but not in the offspring of dams fed high-salt diets (HN_h vs. HN_n or HH_h vs. HH_n). There were no significant differences in heart rate of conscious offspring among the 6 groups. On the day of the determination of cardiac and vascular functions (at 12 weeks of age, 8 weeks after weaning), there were no significant differences in body weight among the 6 groups (Table 1). There were no significant differences in heart weight-to-body weight ratio in offspring fed the control diet (NN_n vs. HH_n and HN_n). In contrast, postweaning high-salt intake increased offspring heart weight (h vs. n). However, this effect was significantly smaller in offspring of dams fed a maternal high salt diet throughout gestation and lactation (HH_h vs. NN_h, Table 1). Citation: Kagota S, Maruyama K, Vliet BNV, et al. Gestational High-Salt Intake Causes Cardiovascular Dysfunction in Adulthood. Heart Circ 2017; 1:007. Volume 1, Issue 1 Kagota et al. Heart Circ 2017; 1:007 Table 1: Changes in offspring blood pressure and heart rate measured using a tail-cuff system at 11 weeks of age and body and heart weights at 12 weeks of age on the day of determination cardiovascular functions in the offspring of dams fed a standard diet containing 0.3% NaCl (N and n) or a high-salt diet containing 6% NaCl (H and h). Systolic blood pressure (mmHg) Heart rate (beats/min) Body weight (g) Heart weight (mg/g body weight) Ventricular heart weight (mg/g body weight) NN_n HN_n HH_n NN_h HN_h HH_h 175 ± 5 176 ± 4 157 ± 5* 192 ± 5 183 ± 6 172 ± 8 395 ± 15 370 ± 11 331 ± 22 387 ± 16 338 ± 10 361 ± 14 298 ± 3 296 ± 6 305 ± 9 318 ± 5 291 ± 5 290 ± 5 4.03 ± 0.08 4.19 ± 0.07 4.09 ± 0.06 4.78 ± 0.11# 4.56 ± 0.07# 4.44 ± 0.07#* 3.74 ± 0.06 3.85 ± 0.06 3.76 ± 0.05 4.44 ± 0.09# 4.22 ± 0.06# 4.07 ± 0.07#* # Results are expressed as the mean ± SEM. n = 7 each group. *P<0.05, NN vs. HN and HH in offspring fed a standard or high-salt diet (effects of mother salt); #P<0.05, n vs. h in each mother (effects of offspring salt). See Figure 1 for detailed protocol for salt loading. B 155 * 55 _n NN _n HN _n HH _h NN _h HN 500 _n NN D 10 5 _n NN _n NH _n HH _h NN _h NH _h HH * 1000 _h 15 * 1500 HH 20 * 2000 _n HN _n HH _h NN _h HN _h HH 300 Heart beat (beats/min) Coronary flow (mL/min) 2500 105 5 C * * -dP/dt (mmHg/sec) LVDP (mmHg) A 200 100 0 _n NN _n NH _n HH _h NN _h NH _h HH Figure 2: Changes in left ventricular cardiac function (A, left ventricular systolic function and B, maximum rate of left ventricular pressure decline), coronary flow (C), and heart beat (D) in Langendorff perfused heart of the offspring of dams fed a high or normal salt diet at 12 weeks of age. Results are expressed as the mean ± SEM. n = 7 each group. *P<0.05. See Fig. 1 for detailed protocol for salt loading. Offspring cardiac function determined by a Langendorff heart perfusion system LV contractile function (Figure 2A) and diastolic function (Figure 2B) were unchanged in the offspring of dams fed a high-salt diet during gestation alone (HN_n), but were significantly decreased in the offspring of dams fed a high-salt diet during both gestation and lactation (HH_n). Post-weaning high-salt intake did not itself significantly affect cardiac functions in the offspring of either control diet-fed dams or the high-salt diet-fed dams (n vs. h, Figure 2A and 2B). There were no significant differences in coronary flow or in spontaneous heart rate of the isolated hearts among the 6 groups (Figure 2C and 2D). Offspring vasodilatory myograph methods function determined by Figure 3A and Table 2 shows endothelium-independent nitroprusside-induced relaxations for the thoracic aortas of offspring. The sensitivity to nitroprusside was decreased by maternal dietary salt during gestation only (NN_n vs. HN_n), and the degree of the decrease was the same in offspring of the high-salt diet-fed dams during both gestation and lactation (HH_n). A decrease was also observed in response to a post-weaning high-salt intake in offspring of the normal diet-fed dams (NN_n vs. NN_h). In contrast, post-weaning high-salt intake was not altered in offspring of dams fed the high-salt diet during gestation alone (HN_n vs. HN_h) or during gestation and lactation (HH_n vs. HH_h). As shown in Figure 3B and Table 2, impairment of vasodilatory responses in response to a maternal dietary high-salt diet was also observed in mesenteric arteries of offspring of the high-salt diet-fed dams during either gestation only or during gestation and lactation. Discussion & Conclusion We have previously demonstrated that a maternal high-salt (4% NaCl) diet throughout gestation and lactation causes dysfunction of post-weaning cardiac and vascular functions in SHR [24]. The present study compared these functions in offspring exposed to a maternal high-salt (6% NaCl) diet during gestation alone versus throughout both gestation and lactation. The data of this study confirmed the ability of a maternal high-salt diet during gestation and lactation to impair cardiac and vascular dilator function. In addition, however, the data also demonstrate that exposure to the maternal high-salt diet during gestation alone was sufficient to impair vascular NO-dependent dilation. Furthermore, the effects of maternal exposure to a high-salt Citation: Kagota S, Maruyama K, Vliet BNV, et al. Gestational High-Salt Intake Causes Cardiovascular Dysfunction in Adulthood. Heart Circ 2017; 1:007. Volume 1, Issue 1 Kagota et al. A B 100 80 NN_n HN_n HH_n 60 40 NN_h HN_h HH_h 20 0 -10 * -log EC50 -9 -8 -7 Nitroprusside (logM) -6 Relaxation (%) 100 Relaxation (%) Heart Circ 2017; 1:007 80 NN_n HN_n HH_n 60 40 NN_h HN_h HH_h 20 0 -10 -9 -8 -7 Nitroprusside (logM) * -log EC50 -6 Figure 3: Changes in the vasodilatory response to nitroprusside in isolated aorta (A) and mesenteric artery (B) in the offspring of dams fed a high or normal salt diet at 12 weeks of age. Results are expressed as the mean ± SEM. n = 7 each group. *P<0.05. See Fig. 1 for detailed protocol for salt loading. Table 2: Changes in the vasodilatory response to nitroprusside in thoracic aorta and mesenteric artery measured by myograph methods in the offspring of dams fed a standard diet containing 0.3% NaCl (N and n) or a high-salt diet containing 6% NaCl (H and h) at 12 weeks of age. Thoracic aorta Mesenteric artery -Log EC50 Emax -Log EC50 Emax NN_n 8.38 ± 0.07 87.9 ± 1.2 7.78 ± 0.03 92.3 ± 1.3 HN_n 8.10 ± 0.08* 85.1 ± 1.5 7.49 ± 0.06* 89.2 ± 1.7 HH_n 8.09 ± 0.02* 89.2 ± 1.0 7.51 ± 0.06* 88.6 ± 4.3 NN_h 8.02 ± 0.08# 88.3 ± 1.3 7.33 ± 0.06# 88.1 ± 1.6 HN_h 7.90 ± 0.07 91.9 ± 1.4 7.38 ± 0.05 85.2 ± 2.9 HH_h 8.09 ± 0.03 93.2 ± 1.0 7.50 ± 0.04 90.8 ± 2.1 Results are expressed as the mean ± SEM. n = 7 each group. *P<0.05, NN vs. HN and HH in offspring fed a standard or high-salt diet (effects of mother salt); #P<0.05, n vs. h in each mother (effects of offspring salt). See Figure 1 for detailed protocol for salt loading. diet throughout gestation and lactation on cardiac function appeared to be greater than those caused by exposure during gestation alone (e.g. comparing LV functions for HN_n with HH_n in Figure 2). This suggests that the harmful effects of a maternal high-salt diet during gestation on cardiac function can be reduced by salt restriction during the subsequent period of lactation. The present study focused on the effects of maternal and offspring salt intake on functional changes assessed in vitro in isolated hearts and vascular segments. Our results point to important functional effects on both the heart and vasculature in vitro. Nevertheless, it is important to consider that these effects may be manifested differently under the loading and neurohumoral conditions that prevail in the intact animal. A recent study demonstrated that increased salt in the maternal diet has lasting effects on offspring cardiovascular function that were not only highly sex-dependent, but were also related to the offspring’s stress-response [25]. Careful consideration will be required to fully understand and explain the net effects of maternal salt intake on cardiovascular function of the intact animal. In salt-sensitive individuals or species, a high-salt intake leads to an increase in blood pressure in the manner that we observed here in the offspring of dams fed a standard diet (NN_n vs. NN_h group). In contrast, a post-weaning high-salt intake did not affect blood pressure in the offspring of dams fed a high-salt diet (e.g. HH_n vs. HH_h group). It is not clear why a high maternal salt intake would reduce the salt-sensitivity of offspring blood pressure, though it may reflect the impairment of cardiovascular functions that we have observed to be produced by maternal salt intake. In addition, the impairment could be associated with decrease in blood pressure in the offspring of dams fed a high-salt diet (HH_n vs. NN_n group). There have been few studies investigating the effect of the period of maternal exposure to a high-salt diet on blood pressure and heart functions of offspring. For example, a maternal 8% NaCl diet from conception to weaning accelerated the increase in post-weaning blood pressure of offspring, but maternal high-salt intake during lactation period only was not altered in the borderline hypertensive rat strain at 8 weeks of age [22]. In another report, a maternal 3%NaCl diet during gestation and lactation was found to not alter blood pressure of SHR offspring [26]. In contrast, a maternal high-salt diet during gestation alone was reported to have less of an effect on offspring blood pressure than exposure during both gestation and lactation in female Brattleboro rats [27]. Furthermore, in heart functions, neither a maternal 8% NaCl diet during gestation nor during lactation alone was found to affect offspring heart rates in the borderline hypertensive rats at 17 weeks of age [22]. The present study indicates that decreases in blood pressure, unchanged heart rate, and decrease in LV contractile and diastolic functions were observed in SHR offspring of the 6% NaCl diet-fed dams during gestation and lactation independent with a post-weaning high-salt diet (HH_n groups). The extent of the dysfunction was approximately similar to the degree induced by a maternal 4% NaCl diet during gestation and lactation in our previous study [24]. Cardiac abnormalities, normal LV contractile and impaired LV diastolic functions, were also described in SHR exposed to a post-weaning 8% NaCl intake (a higher concentration of NaCl compared to that we used) from 8 to 16 weeks of age [14]. This suggests that a maternal high-salt intake has long-term consequences for cardiac functions of offspring in later life, including effects that may be similar to some of those of a post-weaning high-salt intake. Concerning the mechanisms associated with cardiac dysfunction, we previously demonstrated that a maternal high-salt diet reduces alphasmooth muscle-actin expression and phosphorylated phospholambanto-phospholamban ratio in SHR offspring myocardium, which would be expected to lead to a reduced intracellular Ca2+ uptake into the sarcoplasmic reticulum Ca2+-ATPase [28,29]. On the other hand, the dysfunction was mild in offspring of the high-salt diet-fed dams only during gestation (HN_n group) compared to that the effects of highsalt intake during gestation and lactation (HH_n group). These results suggest that maternal exposure to a high-salt diet from gestation until the early post-weaning period may be required for the full development of cardiac dysfunction in offspring. In other words, restriction of salt intake during lactation may be a significant approach to help reduce cardiovascular dysfunction in offspring in later life. The current study suggests that the period of gestation also plays an important role in the effects of maternal high-salt intake on NOdependent vasodilation in offspring. When dams were fed with the high-salt diet during gestation alone (HN_n group), this was sufficient to impair the vasodilatory response to an NO-donor (nitroprusside) in Citation: Kagota S, Maruyama K, Vliet BNV, et al. Gestational High-Salt Intake Causes Cardiovascular Dysfunction in Adulthood. Heart Circ 2017; 1:007. Kagota et al. Volume 1, Issue 1 offspring, and the extent of the dysfunction was the same as in offspring of the high-salt diet-fed dams during both gestation and lactation (HH_n group). An impaired dilatory response to NO is likely to be key contributor to vascular dysfunction, irrespective of whether endothelial production of NO is reduced or not. Furthermore, the extent of the vascular dysfunction caused by a maternal high-salt diet (HN_n and HH_n group) was the same as in the high-salt diet-fed offspring of the normal dams (NN_h group). In other words, the influence of a maternal high-salt diet on vascular functions was approximately equivalent to that of a post-weaning high-salt intake. This may be the reason that post-weaning high-salt intake did not cause further impairment in offspring of dams fed a high-salt diet. Concerning the underlying mechanisms, impairment of sGC-related pathway in vascular smooth muscle cells may be anticipated to play a role based on our previous findings that both perinatal 4% NaCl diet [24] and post-weaning 8% NaCl diet [8,30] decreased sGC expressions in SHR arteries. This possibility is also consistent with a recent report that a 8% NaCl maternal diet during gestation alone increased vascular contractility in association with decreased sGC expression in Sprague-Dawley rat offspring [23]. In that study, nitroprusside-induced increases in cGMP were attenuated in the arteries of offspring of the high-salt diet fed mothers. This mechanism could also explain the decreased response to nitroprusside in aorta and mesenteric artery in the offspring of salt fed mothers in the present study. Taken together, the findings indicate the potential for exposure to high-salt to lead to vascular dysfunction as a consequence of an impaired response to NO in vascular smooth muscle cells, particularly in aorta. In mesenteric artery, a maternal high-salt intake (4%NaCl diet) during pregnancy and lactation was also shown to reduce NO-independent vasodilations in fetal offspring (day 18), weanling offspring (day 21) and adult offspring (day 135) in SpragueDawley rats [31]. Since a number of factors contribute to vasodilation in mesenteric arteries, further studies will be required to determine the detailed mechanisms underlying the vascular dysfunction induced by a maternal high-salt diet in this vessel. In addition, by comparing with the data of the present study with our previous observation [24], the extent of the dysfunction in offspring of a 6% NaCl diet-fed dams was greater than that in the group fed 4% NaCl diet during gestation and lactation, suggesting that the severity of the vascular dysfunction is likely dependent on the amount of NaCl in the maternal diet. On the other hand, several studies and a recent review have raised concern that excessive maternal salt restriction during pregnancy could also lead to development of disease in adult offspring [32]. Thus, in the future, it will be important to further define the levels of maternal salt intake that may trigger, or prevent, cardiovascular dysfunction in offspring. In conclusion, the results of the present study suggest that consumption of a maternal high-salt diet during gestation alone is sufficient to impair the vascular dilatory response to NO in adult offspring, to an extent that is comparable with that induced by a post-weaning high-salt diet. Furthermore, our results indicate that consumption of a maternal high salt diet during gestation and lactation significantly impairs offspring cardiac function, and that this impairment can be alleviated, at least in part, by salt-restriction during the lactation period. It has been reported that preference for salt increases during pregnancy in women [17,18]. The data of the present study provides a contribution to our understanding of the time periods in which maternal salt restriction may help prevent a disturbance in cardiovascular function in offspring. Acknowledgments This research was partly supported by a grant from the Salt Sciences Research Foundation (No. 1533, to S. Kagota) in Japan. The authors greatly thank Ms. Iwata Saki, Ms. Shiori Koyanagi, Ms. Yuki Fukao and Ms. Madoka Nagai for their technical support. Heart Circ 2017; 1:007 References 1. Strazzullo P, D’Elia L, Kandala NB, Cappuccio FP. Salt intake, stroke, and cardiovascular disease: meta-analysis of prospective studies. BMJ. 2009; 339:b4567. 2. Muntzel M, Drueke T. A comprehensive review of the salt and blood pressure relationship. Am J Hypertens. 1992; 5:1S-42S. 3. Johnson C, Raj TS, Trieu K, Srcand J, Wong MMY, McLean R. et al., The Science of Salt: A Systematic Review of Quality Clinical Salt Outcome Studies June 2014 to May 2015. J Clin Hypertens. 2016; 18: 832–839. 4. de la Sierra A, Antonio MT, Coca A. Endothelial dysfunction in salt-sensitive essential hypertension. Hypertension. 2001; 37: 444-448. 5. Miyoshi A, Suzuki H, Fujiwara M, Masai M, Iwasaki T. Impairment of endothelial function in salt-sensitive hypertension in humans. Am J Hypertens. 1997; 10:1083-1090. 6. Dickinson KM, Clifton PM, Keogh JB. Endothelial function is impaired after a high-salt meal in healthy subjects. Am J Clin Nutr. 2011; 93:500-505. 7. Tzemos N, Lim PO, Wong S, Struthers AD, MacDonald TM. Adverse cardiovascular effects of acute salt loading in young normotensive individuals. Hypertension. 2008; 51:1525-1530. 8. Kagota S, Tamashiro A, Yamaguchi Y, Sugiura R, Kuno T, Nakamura K, et al. Downregulation of vascular soluble guanylate cyclase induced by high salt intake in spontaneously hypertensive rats. Br J Pharmacol. 2001; 134:737744. 9. Mervaala EM, Malmberg L, Teräväinen TL, Lähteenmäki T, Karjala K, Paakkari I, et al. Influence of different dietary salts on the cardiovascular and renal effects of moxonidine in spontaneously hypertensive rats. Naunyn Schmiedebergs Arch Pharmacol. 1997; 356:107-114. 10.Luscher TF, Raij L, Vanhoutte PM. Endothelium-dependent vascular responses in normotensive and hypertensive Dahl rats. Hypertension. 1987; 9:157-163. 11.Boegehold MA. Reduced influence of nitric oxide on arteriolar tone in hypertensive Dahl rats. Hypertension. 1992; 19:290-295. 12.Matavelli LC, Zhou X, Varagic J, Susic D, Frohlich ED. Salt loading produces severe renal hemodynamic dysfunction independent of arterial pressure in spontaneously hypertensive rats. Am J Physiol Heart Circ Physiol. 2007; 292:H814-9. 13.Schlaich MP, Klingbeil A, Hilgers K, Schobel HP, Schmieder RE. Relation between the renin-angiotensin-aldosterone system and left ventricular structure and function in young normotensive and mildly hypertensive subjects. Am Heart J. 1999; 138:810-817. 14.Varagic J, Frohlich ED, Díez J, Susic D, Ahn J, González A, et al. Myocardial fibrosis, impaired coronary hemodynamics, and biventricular dysfunction in salt-loaded SHR. Am J Physiol Heart Circ Physiol. 2006; 290:H1503-1509. 15.Warner MJ, Ozanne SE. Mechanisms involved in the developmental programming of adulthood disease. Biochem J. 2010; 427:333-347. 16.Szostak-Wegierek D. Intrauterine nutrition: long-term consequences for vascular health. Int J Womens Health. 2014; 6:647-656. 17.Brown JE, Toma RB. Taste changes during pregnancy. Am J Clin Nutr. 1986; 43:414-418. 18.Morris MJ, Na ES, Johnson AK. Salt craving: the psychobiology of pathogenic sodium intake. Physiol Behav. 2008; 94:709-721. 19.Piecha G, Koleganova N, Ritz E, Müller A, Fedorova OV, Bagrov AY, et al. High salt intake causes adverse fetal programming--vascular effects beyond blood pressure. Nephrol Dial Transplant. 2012; 27:3464-3476. 20.Ding Y, Lv J, Mao C, Zhang H, Wang A, Zhu L, et al. High-salt diet during pregnancy and angiotensin-related cardiac changes. J Hypertens. 2010; 28:1290-1297. 21.Lv J, Zhang P, Zhang Y, Kuang H, Cao L, Wu C, et al. Maternal high-salt intake during pregnancy reprogrammed renin-angiotensin system-mediated cardiomyocyte apoptosis in the adult offspring heart. Reprod Sci. 2014; 21:52-62. Citation: Kagota S, Maruyama K, Vliet BNV, et al. Gestational High-Salt Intake Causes Cardiovascular Dysfunction in Adulthood. Heart Circ 2017; 1:007. Kagota et al. Volume 1, Issue 1 22.Hunt RA, Tucker DC. Developmental sensitivity to high dietary sodium chloride in borderline hypertensive rats. Hypertension. 1993; 22:542-550. 23.Jiang L, Yin X, He A, Li L, Bo L, Zhou X, et al. High-salt diets during pregnancy increases renal vascular reactivity due to altered soluble guanylyl cyclase-related pathways in rat offspring. J Nutr Biochem. 2016; 28:121128. 24.Maruyama K, Kagota S, Van Vliet BN, Wakuda H, Shinozuka K. A maternal high salt diet disturbs cardiac and vascular function of offspring. Life Sci. 2015; 136:42-51. 25.Gray C, Gardiner SM, Elmes M, Gardner DS. Excess maternal salt or fructose intake programmes sex-specific, stress- and fructose-sensitive hypertension in the offspring. Br J Nutr. 2016; 115:594-604. 26.Di Nicolantonio R, Hoy K, Spargo S, Morgan TO. Perinatal salt intake alters blood pressure and salt balance in hypertensive rats. Hypertension. 1990; 15:177-182. 27.Hazon N, Parker C, Leonard R, Henderson IW. Influence of an enriched dietary sodium chloride regime during gestation and suckling and post-natally on the ontogeny of hypertension in the rat. J Hypertens. 1988; 6:517-524. Heart Circ 2017; 1:007 28.Periasamy MP, Bhupathy, Babu GP. Regulation of sarcoplasmic reticulum Ca2+ ATPase pump expression and its relevance to cardiac muscle physiology and pathology. Cardiovasc Res. 2008; 77:265-273. 29.Trieber CA, Ceholski DK, Stokes DL, Young HS. Phosphorylation and mutation of phospholamban alter physical interactions with the sarcoplasmic reticulum calcium pump. J Mol Biol. 2011; 405:707-723. 30.Kagota S, Tamashiro A, Yamaguchi Y, Nakamura K, Kunitomo M. High salt intake impairs vascular nitric oxide/cyclic guanosine monophosphate system in spontaneously hypertensive rats. J Pharmacol Exp Ther. 2002; 302:344351. 31.Gray C, Harrison CJ, Segovia SA, Reynolds CM, Vickers MH. Maternal salt and fat intake causes hypertension and sustained endothelial dysfunction in fetal, weanling and adult male resistance vessels. Sci Rep. 2015; 5:9753. 32.Sakuyama H, Katoh M, Wakabayashi H, Zulli A, Kruzliak P, Uehara Y. Influence of gestational salt restriction in fetal growth and in development of diseases in adulthood. J Biomed Sci. 2016; 23:12. Citation: Kagota S, Maruyama K, Vliet BNV, et al. Gestational High-Salt Intake Causes Cardiovascular Dysfunction in Adulthood. Heart Circ 2017; 1:007.