Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
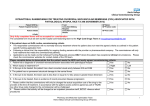
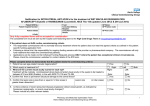
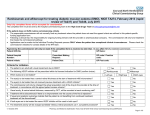
COMMENTARY New England Journal of Medicine Ranibizumab for Neovascular Age-Related Macular Degeneration Philip J. Rosenfeld, MD, PhD, David M. Brown, MD, Jeffrey S. Heier, MD, David S. Boyer, MD, Peter K. Kaiser, MD, Carol Y. Chung, PhD, Robert Y. Kim, MD, for the MARINA Study Group. Background: Ranibizumab—a recombinant, humanized, monoclonal antibody Fab that neutralizes all active forms of vascular endothelial growth factor A—has been evaluated for the treatment of neovascular age-related macular degeneration. Methods: In this multicenter, 2-year, double-blind, sham-controlled study, we randomly assigned patients with age-related macular degeneration with either minimally classic or occult (with no classic lesions) choroidal neovascularization to receive 24 monthly intravitreal injections of ranibizumab (either 0.3 mg or 0.5 mg) or sham injections. The primary end point was the proportion of patients losing fewer than 15 letters from baseline visual acuity at 12 months. Results: We enrolled 716 patients in the study. At 12 months, 94.5% of the group given 0.3 mg of ranibizumab and 94.6% of those given 0.5 mg lost fewer than 15 letters, as compared with 62.2% of patients receiving sham injections (P⬍.001 for both comparisons). Visual acuity improved by 15 or more letters in 24.8% of the 0.3-mg group and 33.8% of the 0.5-mg group, as compared with 5.0% of the sham-injection group (P⬍.001 for both doses). Mean increases in visual acuity were 6.5 letters in the 0.3-mg group and 7.2 letters in the 0.5-mg group, as compared with a decrease of 10.4 letters in the shaminjection group (P⬍.001 for both comparisons). The benefit in visual acuity was maintained at 24 months. During 24 months, presumed endophthalmitis was identified in five patients (1.0%) and serious uveitis in six patients (1.3%) given ranibizumab. Conclusions: Intravitreal administration of ranibizumab for 2 years prevented vision loss and improved mean visual acuity, with low rates of serious adverse events, in patients with minimally classic or occult (with no classic lesions) choroidal neovascularization secondary to age-related macular degeneration. (ClinicalTrials.gov number, NCT00056836.) N Engl J Med. 2006;355:1419-1431. Bevacizumab vs Ranibizumab Treatment for Age-Related Macular Degeneration A Head-to-Head Comparison Is Needed A YEAR AGO, I WENT TO COLLEAGUES AT THE Northwestern University Kellogg School of Business. I described a dilemma that I thought might make an interesting case study for their students and could be the subject for an editorial or commentary. A large pharmaceutical company, Genentech (South San Francisco, Calif), had developed a drug, bevacizumab (Avastin) for the treatment of cancer. The drug is an antibody against vascular endothelial growth factor (VEGF) that can cut off the blood supply to tumors and thereby assist in the management of cancer. The company had received Food and Drug Administration (FDA) approval for the adjunct treatment of colorectal cancer, and trials were being executed for a wide variety of other tumors. At the same time, Genentech spent large amounts of time and money creating a derivative, smaller antibody fragment against VEGF, ranibizumab (Lucentis), that could penetrate the retina and be used intravitreally for treatment of age-related macular degeneration (AMD) or other retinal diseases characterized by abnormal growth of vessels. The phase 3 clinical trials1,2 were completed and showed impressive visual results in this blinding disease; FDA approval was granted for treatment of neovascular AMD; and additional trials were initiated for other (REPRINTED) ARCH OPHTHALMOL / VOL 125, APR 2007 557 neovascular diseases in the eye including diabetic retinopathy. While physicians and scientists were waiting for FDA approval of the ocular product, ranibizumab, bevacizumab was available, and physicians began using it, first intravenously. To avoid systemic adverse effects, the intravitreal route was then tried. This occurred despite the absence of ocular animal studies or clinical trials. The need for effective treatments for AMD was so great that bevacizumab became widely used. To everyone’s delight, bevacizumab appeared as efficacious as ranibizumab, and the adverse events appeared similar. However, there was one difference: the product (bevacizumab) without the extensive animal or major clinical trials would cost somewhere in the range of $25 to $75 per dose, whereas the now FDA-approved product, ranibizumab, was in the range of $2000 per dose. Both drugs have to be used multiple times to obtain maximal benefit, perhaps as frequently as monthly. Therefore, the price differential of therapy with bevacizumab vs ranibizumab is great. The retinal community appealed to Genentech to develop bevacizumab for ophthalmologic use. But Genentech had spent so much time and effort developing ranibizumab, it had little interest in assisting the WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at Univ Of Southern California, on June 1, 2007 ©2007 American Medical Association. All rights reserved. development of bevacizumab for ocular use. At that time, I talked to people at the Federal Trade Commission and lawyers familiar with the topic, and they agreed that Genentech was under no requirement to develop bevacizumab for the eye. The October 5, 2006, issue of The New England Journal of Medicine contains an unprecedented number of AMD articles. There is a beautiful review of the pathophysiology of AMD by de Jong.3 Two articles1,2 describe the 1-year results of the clinical trials that led to FDA approval of ranibizumab. The bottom line of these studies is that this drug is clearly more efficacious than other presently available therapies for AMD, including photodynamic therapy with verteporfin and intravitreal use of triamcinolone or pegaptanib sodium (Macugen; Pfizer, New York, NY), also a VEGF inhibitor. In the 2 AMD trials, choroidal neovascularization, whether minimally classic, occult, or predominantly classic, responded dramatically to multiple intravitreal injections of ranibizumab, with approximately 95% of patients losing fewer than 15 letters at 1 year as compared with about 60% for sham injections or for photodynamic therapy. In addition, unlike photodynamic therapy and pegaptanib use, improvement in visual acuity by 15 or more letters was seen in one quarter to one third of the patients treated with ranibizumab, as compared with only 5% of the sham-injection group and the photodynamic therapy group. Notably, the adverse effects of ranibizumab were acceptable. Rare cases of endophthalmitis or uveitis were seen, and a low incidence of systemic thromboembolism was recorded. Although it has been suggested that VEGF may have a neuroprotective or trophic effect on the retina, and that the inhibition of all active isoforms of VEGF-A might be harmful, to date, this has not been reported clinically. Most of the clinical trials with ranibizumab, including the 2 articles cited,1,2 have used monthly injections for up to 2 years. Some data exist to indicate that regimens that use fewer injections are less efficacious and that treatment in many cases might have to be continued for 2 years or even longer. The enormous cost of these injections (for a disease that is becoming more prevalent as the population ages) could put Centers for Medicare and Medicaid Services payments to physicians for other procedures at risk. If bevacizumab is proven equally effective as ranibizumab, the cost to Medicare, Medicare patients (for their deductible and copayments), patients without insurance, and patients in other parts of (REPRINTED) ARCH OPHTHALMOL / VOL 125, APR 2007 558 the world where treatment with ranibizumab is not fiscally feasible could be dramatically lowered. It is clear that anti-VEGF therapy with ranibizumab or bevacizumab is now our best weapon against neovascular AMD. It is unclear whether combining it with other therapies such as photodynamic therapy or intravitreal corticosteroids might reduce the number of injections required. What is desperately needed is a head-to-head comparison of the efficacy and adverse consequences of bevacizumab and ranibizumab therapies. It seems unlikely that such a study will show that bevacizumab is superior to ranibizumab since the results with ranibizumab are so good. However, a study that shows equivalency would allow more affordable widespread use of antiVEGF therapy. The National Eye Institute has announced its intention to fund a head-to-head comparison of bevacizumab and ranibizumab, but the results of this trial will not be available for 3 or 4 years. In the meantime, some physicians continue to use ranibizumab for AMD exclusively because of its FDA approval, and others continue to use bevacizumab because of its price. Some physicians are using both medications: for example, ranibizumab for Centers for Medicare and Medicaid Services–covered procedures and bevacizumab for the patient where medical insurance does not cover treatment for diseases (other than AMD) for which ranibizumab is not FDA approved. This situation will persist until the National Eye Institute study is completed or a more effective therapy appears. Lee M. Jampol, MD Correspondence: Dr Jampol, Department of Ophthalmology, Feinberg School of Medicine, Northwestern University, 645 N Michigan Ave, Suite 440, Chicago, IL 60611 ([email protected]). Financial Disclosure: None reported. Funding/Support: This work was supported in part by an unrestricted grant from Research to Prevent Blindness, Inc, New York, NY. REFERENCES 1. Rosenfeld PJ, Brown DM, Heier JS, et al; MARINA Study Group. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355:14191431. 2. Brown DM, Kaiser PK, Michels M, et al; ANCHOR Study Group. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355:1432-1444. 3. de Jong PT. Age-related macular degeneration. N Engl J Med. 2006;355:1474-1485. WWW.ARCHOPHTHALMOL.COM Downloaded from www.archophthalmol.com at Univ Of Southern California, on June 1, 2007 ©2007 American Medical Association. All rights reserved.