Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Alzheimer's disease wikipedia , lookup
Auditory system wikipedia , lookup
Telecommunications relay service wikipedia , lookup
Lip reading wikipedia , lookup
Evolution of mammalian auditory ossicles wikipedia , lookup
Hearing aid wikipedia , lookup
Hearing loss wikipedia , lookup
Noise-induced hearing loss wikipedia , lookup
Audiology and hearing health professionals in developed and developing countries wikipedia , lookup
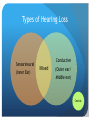
Loss of Hearing and Tinnitus Dr Deborah Amott ENT Surgeon [email protected] Core Presentations By the end of this year, you should be able to perform a competent medical interview, physical examination and suggest a basic investigational plan for a patient presenting with this symptom. Ask 4 Questions… What is the most likely diagnosis? Could this be life-threatening? What information do I need to confirm my diagnosis? What’s my time frame? Context of this Symptom Symptom itself: Acuity Duration Severity Fixed/Variability Progression Triggers/Relievers Associated features: what else is changing? Local, adjacent structures Regional Distant organ dysfunction Systemic symptoms Patient: Demographics: age, sex, race, ethnicity Lifestyle: profession, hobbies, smoking, alcohol, other drugs, other carcinogens, diet. Immune status: Immunosuppressed/Atopic/A utoimmune disease Comorbidities, previous medical conditions or treatment. Environment: season, latitude, humidity/temperature, recent events. What can an ear do? Otorrhoea Otalgia Hear Tinnitus Vertigo Tinnitus: Definition “Perception of a sound in the absence of an environmental acoustic stimulus” Objective OR Subjective Unilateral OR Bilateral: Symmetrical OR Asymmetrical Pulsatile OR Non-Pulsatile Pitch or specific description usually not helpful Tinnitus: Causes ? Tinnitus: Causes All the causes of hearing loss can cause tinnitus, and many commonly do It is possible to experience tinnitus in an ear with normal hearing no hearing at all everything in between. People who have had their inner ear surgically removed can - and often do - experience tinnitus. Pulsatile Tinnitus With the pulse or not? Hypervascularity Physiological Pathological Arterial Arteriosclerosis Aneurysms Dissection Aberrant vessels Venous Benign intracranial hypertension Dehiscent jugular bulb Both AVMs Other Myoclonus: stapedius, tensor tympani, tensor veli palatini So, how do you investigate pulsatile tinnitus? Audiogram Imaging: Anatomy? Vessels? So, how do you investigate pulsatile tinnitus? Audiogram Imaging: Anatomy: CT Temporal Bones for tumours, high riding/dehiscent jugular bulbs, abberrant vessels Vessels: carotid doppler, MRI/MRA/MRV. Hearing Loss Types of Hearing Loss Sensorineural (Inner Ear) Conductive Mixed (Outer ear/ Middle ear) Central General Pathological Processes VINDICATE V-vascular I-infectious/inflammatory N-neoplasia D-drugs/degeneration I-idiopathic C-congenital A-anoxia/acid-base imbalance/auto-immune T-trauma/toxins E-ethyl alcohol, endocrine Genetic: too much vs. too little of an otherwise good thing Audiology: Nomenclature Audiograms Sensorineural (SNHL) Conductive (CHL) Mixed Hearing Loss Causes of Hearing Loss Conductive Sensorineural Causes of Hearing Loss Conductive EAC: material in canal lumen, narrowed lumen TM: perforation, infection, scar, retraction MEC: fluid, ossicular chain disease: discontinuity, ‘rusting tight’, scars Sensorineural Aging: presbycusis Noise Induced HL Trauma Neoplasm Infection … VINDICATE away Asymmetrical SNHL What’s the big deal? Aging Noise Induced HL Trauma Neoplasm Infection … VINDICATE away Weber and Rinne You do need to know these… www.youtube.com/watch?v=o-QKT_o0abc Sudden Sensorineural Hearing Loss • Acute sensorineural hearing loss of at least 30dB across at least 3 frequencies, occurring within three days. • Causes – – – – Infection/Inflammation Vascular Neoplasm Idiopathic • Examination • Why do you need to diagnose it? Anatomy does not Change Fluctuating Hearing Loss Conductive Sensorineural Fluctuating Hearing Loss Conductive Eustachian Tube dysfunction Infections Effusions Barotrauma Sensorineural Endolymphatic hydrops Meniere’s Disease Syphilis Sublethal injury Infection, trauma, vascular Autoimmune ear disease SSNHL (recurrent) Investigations • Know the question you want to answer. • Only order an investigation if the result will affect your management • A proper initial clinical assessment and then repeated thorough clinical assessment is always much better than multiple non-targeted tests. • Recruit help So what can you do? Tinnitus: Is your patient going to top themselves? Treat the distress, and the tinnitus will sort itself out. Tinnitus Association of Victoria Hearing loss: whether conductive or sensorineural Treat reversible causes Optimize functional hearing Aid what needs aiding Cochlear implantation Learn ENT