Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
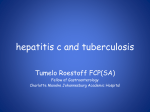
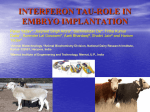
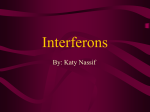
Archives of Andrology, 50:379–385, 2004 Copyright # Taylor & Francis Inc. ISSN: 0148-5016 print / 1521-0375 online DOI: 10.1080/01485010490474823 INTERFERON a-2B MAY IMPAIR TESTICULAR HISTOLOGY INCLUDING SPERMATOGENESIS IN A RAT MODEL E. ULUSOY, S. C° AYAN, N. YILMAZ, S. AKTAS° , D. ACAR, and E. DORUK Department of Urology, University of Mersin School of Medicine, Mersin, Turkey Interferon-a has been used in various diseases at the reproductive ages. However, the effect of interferon-a on testicular histology has not been studied in literature. The aim of this study was to investigate the effects of interferon a-2B on testicular histology including spermatogenesis in a rat model. Seventeen adult male Wistar albino rats were divided into 3 groups: Six rats received 7.500 units (5 MIU=m2) of interferon a-2B (Intron), considered clinical treatment dose range. Six rats received 30.000 units (20 MIU=m2) of interferon a-2B (Intron), considered high treatment dose. Five rats served as a control group receiving 0.5 mL of saline injection. All injections were done intraperitoneally 3 times weekly for 3 weeks under inhalation anesthesia. All rats underwent bilateral orchiectomy 30 days after the experiment. Histological examination included the mean seminiferous tubular diameter (STD), germinal epithelial cell thickness (GECT), and testicular biopsy score (TBS). The mean STD was significantly lower in the low-dose interferon and high-dose interferon groups than in the control group (p ¼ 0.008 and p ¼ 0.004, respectively). The mean GECT was significantly lower in the low-dose interferon and high-dose interferon groups than in the control group (p ¼ 0.008 and p ¼ 0.004, respectively). The mean TBS was significantly lower in the lowdose interferon group (p ¼ 0.05) and the high-dose interferon group (p ¼ 0.01) than in the control group. The decreases in the mean values of the STD, GECT and TBS were not related to the interferon dose. Interferon a-2B may impair testicular histology even in clinical widely used treatment dose. Therefore, men at the reproductive ages should be fully informed for the use of interferon-a in the treatment of various diseases. Keywords interferon, rat, spermatogenesis, testis INTRODUCTION Interferons are widely used in the treatment of various diseases including acute and chronic viral illnesses and certain autoimmune and neoplastic diseases [8]. These agents have a variety of biologic roles, including antiviral activity, regulation of cell growth, and modulation of cellular immunity. Interferon-a is the most commonly used antiviral drug among the interferons as having in vitro antiviral and biologic effects on human cells [6]. Address correspondence to Ercüment Ulusoy, M.D., Associate Professor of Urology, University of Mersin School of Medicine, Department of Urology, Zeytinlibahc° e Caddesi, 33079-Mersin, Turkey. E-mail: erulusoy@ hotmail.com 379 380 E. Ulusoy et al. The use of interferons is associated with early side effects such as a flu-like syndrome and later consequences of treatment which include hematologic, infectious, autoimmune, neuro-psychiatric, and hormonal problems [17]. Interferon-a has been used in many male and female patients at the reproductive ages. Interferon-a has been shown to impair fertility and alter hormone levels in females [13, 15]. However, the effect of interferon-a on testicular function in males undergoing interferon treatment has been controversial in literature. The aim of this study was to investigate the effects of interferon-a on testicular histology including spermatogenesis in an animal model. MATERIALS AND METHODS Study Design The study included 17 adult male Wistar albino rats weighing between 240 and 280 gm, and all rats were maintained on a 12L: 12D cycle. The experiments were approved by the ethical committee on animal research at our institution. We provided appropriate care and use of the laboratory animals as recommended by the Board of Registry publication guidelines. The rats were divided into 3 groups: 6 rats received 7.500 units (5 MIU=m2) of interferon a-2B (Intron), considered in clinical treatment dose range, 3 times weekly for 3 weeks (low-dose interferon group). Six rats received 30.000 units (20 MIU=m2) of interferon a-2B (Intron), considered high treatment dose, 3 times weekly for 3 weeks (highdose interferon group). Five rats served as a control group, receiving 0.5 mL of saline injection 3 times weekly for 3 weeks. All injections were done intraperitoneally under inhalation anesthesia. After 30 days, bilateral orchiectomy was performed through standard ilioinguinal incisions, and the rats were sacrified by pentobarbital overdose (200 mg=kg) and bilateral thoracotomy. Histological examination included the mean seminiferous tubular diamater (STD), germinal epithelial cell thickness (GECT), and testicular biopsy score (TBS). Histological Preparation and Evaluation The testicles were fixed in Bouin’s solution (7.5 ml of saturated picric acid, 2.65 ml of glacial acetic acid and 2.5 ml of 7% formaldehyde), postfixed in 70% alcohol and embedded in paraffin blocks. Five mm sections were obtained, deparaffinized, and stained with Hematoxylin and Eosin to examine the mean STD, GECT, and TBS. Testicular tissue was evaluated with standard light microscopy by a blinded observer in random order. Three slides prepared from the upper, lower and mid portions of the testes were evaluated completely for each testis. The mean STD, GECT, and TBS were used to evaluate in 20 seminiferous tubule of each section. The mean STD and GECT were calculated using a microscope-adaptable micrometer. Therefore, the mean STD and GECT of each testis were determined in mm. The mean TBS was graded using modified Johnsen’s score [20]. A score of 0–12 was given to each tubule according to epithelial maturation. This method of histologic analysis gives an accurate measurement of the degree to which Interferon a-2B and Testicular Histology 381 spermatozoal maturation is taking place within the seminiferous tubule and also the level of spermiogenesis. Statistical Analysis All data were expressed as mean standard deviation (SD). Multiple comparisons were made using Mann Whitney U test between the groups. A p value of <0.05 was considered as statistically significant. RESULTS Figures 1, 2, and 3 show histology of the testis in a rat of the low-dose interferon group, high-dose interferon group, and the control group, respectively. The mean values of the STD, GECT and TBS (modified Johnsen’s score) in all groups are shown in Table 1. The mean STD was significantly lower in the low-dose interferon and high-dose interferon groups than in the control group (p ¼ 0.008 and p ¼ 0.004, respectively). The mean GECT was significantly lower in the low-dose interferon and high-dose interferon groups than in the control group (p ¼ 0.008 and p ¼ 0.004, respectively). The mean testicular biopsy score (modified Johnsen’s score) was lower in the low-dose interferon and high-dose interferon groups than in the control group, revealing statistical significance (p ¼ 0.05 and p ¼ 0.01). Figure 1. Histology of the testis in a rat of the low-dose interferon treatment group, showing decreases in seminiferous tubular diameter, germinal epithelial cell thickness and testicular biopsy score. 382 E. Ulusoy et al. Figure 2. Histology of the testis in a rat of the high-dose interferon treatment group, showing decreases in seminiferous tubular diameter, germinal epithelial cell thickness and testicular biopsy score. The mean values of the STD, GECT and TBS (modified Johnsen’s score) were not statistically significantly different between the low-dose interferon and high-dose interferon groups (p ¼ 0.429, p ¼ 0.792, and p ¼ 0.931, respectively), showing that the decreases in the mean values of the STD, GECT, and TBS were not related to the dose of the interferon treatment. DISCUSSION Interferon-a is approved in the United States for treatment of condyloma acuminatum, chronic hepatitis C, chronic hepatitis B, Kaposi’s sarcoma in HIV-infected patients, and other malignancies including leukemia, multiple myeloma, non-Hodgkin’s lymphoma, and urogenital carcinomas such as renal cell cancer, bladder cancer, and ovarian cancer [8]. Interferons may have direct effects such as inhibition of cell proliferation, induction of differentiation and antiviral effects, and indirect effects such as stimulation of immunologic functions, anti-angiogenesis, and production of other cytokines [1]. Human interferons consist of the multiple type 1 species (alpha, beta, omega and kappa), and the one type 2 species (gamma) [1]. However, three types of human interferons (a, b, w) have been recognized in the clinical use [8]. Interferon w has less antiviral activity but more potent immunoregulatory effects. The principal antiviral interferons, Interferon a-2B and Testicular Histology 383 Figure 3. Histology of the testis in a rat of the control group, showing normal seminiferous tubular diameter, germinal epithelial cell thickness and spermatogenesis. interferon-a, and interferon-b are approximately 30% homologous at the amino acid level. In addition, interferon a is actually a family of multiple species that share a high degree of amino acid sequence homology (>70%) but differ in vitro antiviral and biologic effects on human cells [6]. Therefore, interferon-a is a commonly used antiviral drug among the interferons. The beneficial effect of interferon-a in the treatment of viral hepatitis is related to the activation of lymphocytes such as T cells and natural killer cells, which participate in the elimination of infected cells. The side effects of interferon-a during treatment are seen as general symptoms with a flu-like syndrome in 40 to 85% of cases, neuropsychiatric signs in up to 30% of cases, Table 1. The mean values of the STD, GECT, and TBS (modified Johnsen’s score) of the groups Groups Low-dose interferona (n ¼ 6) High-dose interferonb (n ¼ 6) Control (n ¼ 5) a Seminiferous tubular diameter SD (mm) Germinal epithelial cell thickness SD (mm) Testicular biopsy score SD 219.8 16.43 226.7 14.04 275.5 4.03 62.7 5.33 62.66 4.51 81.8 5 11.76 0.22 11.83 0.06 11.95 0.05 versus control p ¼ 0.008 for STD, p ¼ 0.008 for GECT and p ¼ 0.05 for TBS. versus control p ¼ 0.004 for STD, p ¼ 0.004 for GECT and p ¼ 0.01 for TBS. b 384 E. Ulusoy et al. thyroid dysfunction in 5 to 10% of cases, hematological side effects in more than 50% of cases, dermatological abnormalities frequently, and cardiovascular and ophthalmic disorders rarely [7]. Although interferon-a has been used in the treatment of mumps orchitis, the preventive role of the interferon treatment has still been controversial. Significant preventive effects of systemic treatment with interferon a-2B for infertility from mumps orchitis has been reported by two articles [5, 11]. In contrast to these studies, Yeniyol et al. reported the role of interferon-a for the prevention of testicular atrophy in postpubertal men with unilateral mumps orchitis [19]. They found that systemic treatment with interferon a-2B was not completely effective in preventing testicular atrophy after mumps orchitis. Deterioration of reproductive function and alteration of serum hormone have been shown with the use of interferon-a in women [13, 15]. Interferons have been shown to inhibit Leydig cell steroidogenesis in vitro, through inhibition of StAR expression [12, 16]. Corssmit et al. reported acute effects of interferon-a treatment on the hypothalamicpituitary-testicular axis in healthy men, and they found that interferon treatment decreased serum testosterone and free androgen index [3]. Therefore, interferon treatment may change feedback relationships between the pituitary and the testis. Karamfilov et al. investigated the effect of low dose interferon-a therapy in patients with melanoma, and they found no significant effect on serum inhibin B level as a marker of male fertility with the use of low dose interferon-a [10]. However, the effect of interferon-a on spermatogenesis has not been clearly demonstrated in men with normal testes. Possible effects of interferon-a on sperm parameters in the treatment of male infertility have been controversial. Yamamoto and Miyake reported successful use of interferon for male infertility [18]. However, azoospermia was reported in a patient receiving interferon alpha for a stage 3 melanoma [14]. Hibi et al. found that daily sperm production and epididymal sperm concentrations were significantly increased after interferon alpha treatment in the nude rats [9]. Therefore, they concluded that these promising results with interferon-a may pave the way for a new approach to treating male infertility. However, they did not investigate testicular spermatogenesis using Johnsen’s score. In the present study, we investigated the effects of interferon a-2B on testicular histology including spermatogenesis in a rat model. We found that the mean STD, GECT, and TBS were significantly lower in the low-dose interferon and high-dose interferon groups than in the control group. The decreases in the mean values of the STD, GECT and TBS were not related to the interferon dose, showing that interferon might impair testicular histology regardless of the dose of the treatment. Interferons have been considered as apoptosis inducing cytokines [2]. Both type 1 and type 2 interferons have been found in the testis, and are stimulated by viral infections, particularly in Sertoli and Leydig cells. They are involved in protecting the testis against viral infections [4]. It has been demonstrated that interferons induce apoptosis by activating the death receptor cascade in cancer patients [2]. However, testicular apoptosis has not been studied with the use of interferons. Increased apoptosis might impair spermatogenesis in male patients undergoing interferon treatment. In conclusion, our findings suggest that interferon a-2B may impair testicular histology even in clinical widely used treatment dose. Therefore, men at the reproductive ages should be fully informed for the use of interferon-a in the treatment of various diseases. Interferon a-2B and Testicular Histology 385 REFERENCES 1. Borden EC, Williams BRG (2000): Interferons. In: Cancer Medicine, 5th edition. Bast RC Jr, Holland JF, Gansler TS, (Eds). Toronto: B.C. Decker Inc, pp 815–824. 2. Chawla-Sarkar M, Lindner DJ, et al. (2003): Apoptosis and interferons: role of interferonstimulated genes as mediators of apoptosis. Apoptosis 8:237–249. 3. Corssmit EP, Endert E, et al. (2000): Acute effects of interferon-alpha administration on testosteron concentrations in healthy men. Eur J Endocrinol 143:371–374. 4. Dejucq N, Lienard MO, Jegou B (1998): Interferons and interferon-induced antiviral proteins in the testis. J Reprod Immunol 41:291–300. 5. Erpenbach KH (1991): Systemic treatment with interferon-alpha 2B: an effective method to prevent sterility after bilateral mumps orchitis. J Urol 146:54–56. 6. Finter NB (1991): Why are there so many subtypes of alpha-interferons? In: Journal of Interferon Research. Marcus PI, (ed). New York: Mary Ann Liebert Publishers, pp 185–194. 7. Fontaine H, Pol S (2001): Side effects of interferon-alpha in treating hepatitis C virus infection. Transplantation Proceedings 33:2327–2329. 8. Hayden FG (2000): Antiviral drugs (other than antiretrovirals). In: Principles and Practice of Infectious Diseases. Mandell GL, Bennett JE, Dolin R (Eds). Philadelphia: Churchill Livingstone, pp 460–491. 9. Hibi H, Yokoi K, Yamamoto M (1997): Effects of alpha-interferon on sperm production, concentration, and motility in the rat. Int J Urol 4:603–607. 10. Karamfilov T, Wollina U, et al. (2000): Effects of adjuvant interferon-alpha low-dose therapy in melanoma patients on serum inhibin B. J Dermatol 27:639–642. 11. Ku JH, Kim YH, et al. (1999): The preventive effect of systemic treatment with interferon-alpha 2B for infertility from mumps orchitis. BJU Int 84:839–842. 12. Lin T, Hu J, et al. (1998): Interferon-gamma inhibits the steroidogenic acute regulatory protein Messenger ribonucleic acid expression and protein levels in primary cultures of rat Leydig cells. Endocrinology 139:2217–2222. 13. Lipton JH, Derzko CM, Curtis J (1996): Alpha-interferon and pregnancy in a patient with CML. Hematol Oncol 14:119–122. 14. Longo I, Sanchez-Mateos P, et al. (2002): Azoospermia in a patient receiving interferon alpha for a stage 3 melanoma. Acta Derm Venereol 82:389–390. 15. Naz RK, Butler A, et al. (1995): Levels of interferon-gamma and tumor necrosis factor-alpha in sera and cervical mucus of fertile and infertile women: implication in infertility. J Reprod Immunol 29:105–117. 16. Orava M, Cantell K, Vihko R (1985): Human leukocyte interferon inhibits human chorionic gonadotropin stimulated testosterone production by porcine Leydig cells in culture. Biochem Biophys Res Commun 127:809–815. 17. Quesada JR, Talpaz M, et al. (1986): Clinical toxicity of interferons in cancer patients. J Clin Oncol 4:234–243. 18. Yamamoto M, Miyake K (1994): Successful use of interferon for male infertility. Lancet 344 (8922):614. 19. Yeniyol CO, Sorguc S, et al. (2000): Role of interferon-alpha-2B in prevention of testicular atrophy with unilateral mumps orchitis. Urology 55:931–933. 20. Yoshida A, Miura K, Shirai M (1997): Evaluation of seminiferous tubule scores obtained through testicular biopsy examinations of nonobstructive azoospermic men. Fertil Steril 68: 514–518.