Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
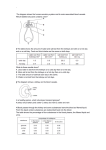
Renal System Joanna Shedd, MS, CNS, RN Disorders of the Urinary Tract Presented By: Joanna Shedd Kidneys • Left and right • Adrenal on each kidney • Vascular organ • Nephrons in cortex Diagnostic Exams for Kidneys • Routine UA • Color significance p. 1506 • Creatinine Clearance • 24-hr Cr. Clearance Diagnostics: Urinalysis – “UA” • • • • • Color – amber to yellow Clarity - clear pH – 4.6 – 8.0 Specific gravity – 1.010 – 1.030 Protein – 0 – 8 mg/dL Diagnostics: Urinalysis Continued • • • • • Sugar – no sugar normally Ketones – none, normally Red blood cells (RBC) – 0 – 4 White blood cells (WBC) – 0 – 5 Casts – none, normally Diagnostics Continued • Culture & Sensitivity • Blood Tests BUN (blood urea nitrogen) Creatinine CBC (complete blood count) Diagnostics: Blood Urea Nitrogen (BUN) • Passes through glomerular filtrate unchanged • Reabsorbed during passage through nephron • Range: 5 – 20 mg/dL Processes that can affect BUN • • • • • • High-protein diet GI bleeding Hepatic disease Dehydration Medications Catabolic state – starvation, injury, infection Diagnostics Continued Radiology: • KUB (kidney, ureters, bladder) • IVP (intravenous pyelogram) • Prep with laxatives, • NPO after MN • Check for allergies, • Baseline renal function Diagnostic Continued • Blood Urea Nitrogen (BUN) – ability of the kidney to excrete nitrogenous wastes • End product of protein metabolism • Can be affected by many factors • Creatinine (Cr) – ability of the kidney to excrete creatinine • End product of creatine • Muscle is more stable • Better indicator of kidney function Functions of the Kidney • • • • • Remove waste products Regulate fluid balance Maintain electrolyte imbalance Regulate BP Activates growth hormone Diagnostics Continued Radiology: • Renal angiography • Arterial, more invasive • Post care similar to angio care Diagnostics Continued Other: • Cystoscopy – Direct visualization of urinary tract • Renal biopsy – Examine tissue under microscope Intake and Output (I&O) • Essential to determine fluid deficit or excess • Can affect patient outcomes • Doctors will treat patient accordingly, i.e., IV therapy • Assess patient for accompanying signs/ symptoms Intake • Orally – including ice chips • Parenterally – IV fluids, blood products • Rectally • Tubes, etc • Semi-solid foods Output • • • • • • Urine – color and amount Gastric secretions Vomitus GI drainage Wound drainage Stools Functions of the Kidney • Ultra filtration • Process by which urine is formed • Around 1-2L/day excreted • Filtration in Bowman’s capsule • Reabsorption and secretion in tubules and collecting duct Functions of the Kidney • Electrolyte balance • Aldosterone • Anti-diuretic hormone (ADH) • Acid-base balance • Lungs – CO2 • Kidneys – HCO3 Functions of the Kidney • Erythropoietin – red blood cell production • Calcium regulation • Multiple processes • Phosphorous regulation • Component of all intermediates of glucose metabolism Functions • Blood pressure regulation • ADH • Renin-angiotensin-aldosterone System (RAAS) Functions • Excretion of metabolic wastes and toxins • Excreted in glomerular filtrate • Drugs either excreted directly from kidneys • OR metabolized in liver, then excreted by kidneys URINARY TRACT INFECTION • Infection anywhere in the urinary tract • Cystitis (Bladder Infection) • Pyelonephritis (kidney infection) • Urosepsis Urinary Tract Infection Continued Predisposing Factors: • Women>Men • Aging • Certain disease processes • Injury/trauma to mucosal lining • Urinary stasis/ retention • Poor hygiene/ clothing • Allergens/ irritants Cystitis: Signs and Symptoms • • • • • Burning/Dysuria Frequency/Urgency Void small amounts Low back/ suprapubic pain Bladder spasm • • • • Malaise Chills/fever Nausea/vomiting Cloudy, possibly bloody urine Pyelonephritis: Signs/Symptoms • • • • • • • • High fever Chills Nausea Pain on affected side Headache Malaise Cloudy, bloody, foul-smelling urine Dysuria Interventions • • • • • • • Bladder- usually po, 7-10 days Pyelo – usually IV 3-5 days, then po 2-4 weeks Increase fluid intake Acidify urine Comfort measures Eliminate cause Education on prevention UROLITHIASIS • Stones in urinary tract • Most common: renal Predisposing factors: • • • • Supersaturation of urine Urine Stasis Urinary PH Presence of precipitate UROLITHIASIS Signs/Symptoms: • Nausea/vomiting • Pale, clammy skin • Hematuria • Can lead to hydro-nephrosis, obstruction • Can lead to acute renal failure • Intense, colicky pain on affected side UROLITHIASIS: Interventions • • • • • • Push fluids Encourage ambulation Antispasmodics/ narcotics Moist heat to flank Anti-emetics for nausea Strain all urine UROLITHIASIS: Interventions • Ureteral Catheters • Extracorporeal shockwave lithotripsy (ESWL) • After procedure: drink water and ambulate • Watch for bleeding, strain urine • Surgical intervention • Percutaneous nephroscopic removal • Open surgical procedure ACUTE RENAL FAILURE • • • • Abrupt loss of kidney function Can be over few hours to few days Usually reversible Can progress to Chronic renal failure Acute Renal Failure Acute Renal Failure Causes: Prerenal • Any condition that interferes with blood flow to kidneys • Most common: hypovolemia & hypotension • Decrease perfusion leads to decrease urine Causes: Intrarenal • • • • • Damage to kidneys themselves Kidney disease Trauma/injury Nephrotoxins Acute tubular necrosis Causes: Postrenal • Obstruction in urinary tract • Benign prostatic hypertrophy (BPH) • Tumors • Calculi • Secondary damage to kidneys Clinical Phases • Initiation phase • Maintenance phase • Oliguric period • Diuretic period • Recovery phase Signs/Symptoms Fluid imbalances HTN CHF Pulmonary edema Acidemia Uremia Electrolyte imbalances K+ Ca2+ Na+ pre-renal (low Na+) Intrarenal (high Na+) Anemia Interventions: Correct Cause Electrolyte Balance • K+ - kayexalate • Phosphorous • Calcium • Correct acidosis • NaHCO3 • Dialysis Fluid Balance • I&O • BP • Daily Weight – 1lb = 500cc • Breath sounds • Na+ levels Shock • Inadequate blood flow to vital organs • Cells become unable to extract and use oxygen Blood flow • Adequate amounts of blood for heart to pump • Effective pumping by heart • Constriction and dilation of blood vessels to maintain blood pressure Hypovolemic Shock • Most common • Caused by loss of: • Whole blood • Plasma • Interstitial fluid • Loss is so great, body’s metabolic needs are not met Causes of Hypovolemic shock • • • • • • Trauma GI bleeding Burns Severe vomiting/ diarrhea Diuretic therapy Renal failure Hypovolemic Shock - Pathophysiology • Loss of volume affects circulation to organs and body • Affects balance of release of hormones to maintain homeostasis Hypovolemic shock - Patho • • • • Body preserves vital organs first Decreased cardiac output Vasoconstriction of kidneys Decreased renal perfusion Hypovolemic shock • Ischemia stimulates release of renin (activates RAAS) • Release of Aldosterone reabsorbs Na+ and H2O • Reduced renal perfusion Hypovolemic shock • Oliguria – markedly decreased urine • Decrease cardiac output • Cycle continues to spiral downward Interventions • Return volume with either fluid or plasma • Watch electrolytes • Strict intake and output (I&O) Creatinine • Excreted unchanged in urine • • • • Range: 0.6 – 1.5 mg/dL Usual ratio to BUN 1:10 Creatinine clearance test Levels tested in 12-24 hr urine test Nursing • Understand importance of I&Os • Importance to maintain >30cc/hr • Other cues for hydration: skin turgor, urine color, odor, etc. • Good health history/ assessment • Renal system important for homeostasis An abnormal finding on a urinalysis is? A. B. C. D. Color – pale yellow Glucose – present 3+ RBC – 0 Specific gravity – 1.020 Oliguria is said to be present with urine output is? A. B. C. D. About 50mL/hr Between 60-70 mL/hr Greater than 100 mL/hr Less than 30 mL/hr A client in an auto accident has lost over a liter of blood . What assessment would the nurse note about the client? A. B. C. D. Face pale, pulse weak & thready Pressures of 110/70 – 120/80 Respirations even, unlabored at 16 Urine yellow, output 200mL/4 hours The nurse is doing I&Os at the end of the shift and notes the following: Oral intake – 480 mls, IV intake – 900 mls; urine output 500 mls. What conclusion can be drawn about the I&Os? A. B. C. D. Client is in homeostaisis balance Client is experiencing fluid deficit of 880 mls Client is experiencing fluid excess of 880mls Client needs to have a foley catheter placed Which of the following is not a function of the kidneys? A. B. C. D. Filtration Maintaining BP levels Maintaining pH levels Making WBCs