Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
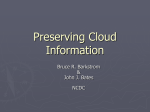
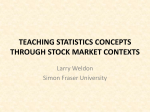
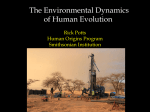
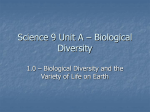
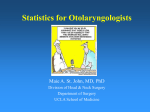
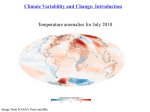
Inverse Relationship Between Heart Rate and Blood Pressure Variabilities in Rats ALBERTO U. FERRARI, ANNA DAFFONCHIO, FRANCESCO ALBERGATI, AND GIUSEPPE MANCIA Downloaded from http://hyper.ahajournals.org/ by guest on April 29, 2017 SUMMARY The interplay of heart rate variability, baroreceptor control of heart rate, and blood pressure (BP) variability was examined in chronically instrumented, unanesthetized, freely moving rats in which the efferent neural influences on heart rate were pharmacologically altered. In each rat, BP was recorded continuously for 90 minutes in the control condition and in one or more of the following conditions: 1) /3-adrenergic receptor blockade by propranolol, 1 mg/kg; 2) cholinergic blockade by atropine, 0.75 mg/kg, and 3) combined blockade by propranolol plus atropine. Each BP recording was analyzed beat-to-beat by a computer that calculated heart rate and BP variabilities, both expressed as variation coefficients. In addition, under each condition the sensitivity of the arterial baroreceptor control of heart rate was assessed by measuring the reflex changes in pulse interval in response to BP changes induced by bolus i.v. injections of phenylephrine and nitroprusside. As compared with the control condition, 1) propranolol (n = 10) reduced heart rate variability by 23 ± 4% (p<0.01), only slightly impaired baroreceptor reflex sensitivity, and did not significantly modify BP variability ( +11 ± 7%); 2) atropine (n = 11) reduced heart rate variability by 30 ± 7% (p<0.01), drastically impaired baroreceptor reflex sensitivity, and increased BP variability ( + 40 ± 8 % , p<0.01); 3) combined blockade (n= 10) caused variability and baroreceptor reflex changes similar to those induced by atropine alone. Thus, heart rate variability depends on both vagal and sympathetic influences. However, only the former component affects BP variability, that is, it plays an antioscillatory role. This role is likely to originate from arterial baroreceptor modulation of vagal cardiac drive. (Hypertension 10: 533-537, 1987) KEY WORDS • blood pressure variability • cardiac parasympathetic nervous system cardiac sympathetic nervous system • arterial baroreceptors • rats S Despite these considerations, our understanding of the mechanisms controlling BP variability is limited. Neurogenic influences are responsible for a substantial proportion of this phenomenon,6 but it is unclear whether its overall magnitude depends more on central modulation of autonomic cardiovascular nerves than on the buffering action of arterial baroreceptor reflexes.7 A further open question concerns the relationship between BP variability and spontaneous heart rate variability, that is, whether heart rate variability plays no role in, enhances, or buffers the BP variations. In the present study pharmacological interventions interfering with the cardiac parasympathetic and sympathetic influences were used to examine the relationship of baroreceptor reflex sensitivity, heart rate variability, and BP variability. The study was conducted in unanesthetized, freely moving rats subjected to continuous BP and heart rate recordings to adequately assess the variability phenomena. TUDIES in several animal species have demonstrated that, in the unanesthetized state, blood pressure (BP) is characterized by a large, spontaneous variability. 12 This variability also has been documented in humans and may have clinical relevance. For example, BP variability is responsible for the poor correlation between cuff BP measurements and 24-hour or daytime BP values.3-4 Furthermore, at any given BP mean, a greater 24-hour BP variability is accompanied by a greater rate and severity of target organ damage than is a smaller BP variability.5 From the Centro di Fisiologia Clinica e Ipertensione, Ospedale Maggiore, CNR, Cattedra di Semeiotica Medica, and Istituto di Clinica Medica Generale e Terapia Medica, Universita di Milano, Milano, Italy. Address forreprints:Dr. Alberto Ferrari, Centro Fisiologia Clinica e Ipertensione, Ospedale Policlinico, Via F. Sforza 35, 20122 Milano, Italy. Received December 15, 1986; accepted June 5, 1987. 533 534 HYPERTENSION Materials and Methods The study used 17 male and female Sprague-Dawley rats (Charles River Italia SpA, Calco, Italy) with a mean age of 11.9 ±0.6 (SE) weeks. With the rats under ketamine anesthesia, 80 mg/kg i.p., PE-50 catheters were implanted in the femoral artery and vein, tunneled subcutaneously, exteriorized at the dorsal neck region and kept patent by flushing with appropriate heparin solution (0.01% vol/vol). The animals were allowed 2 days to recover from the operation and to get acquainted with the experimental environment, which consisted of wide individual cages in which rats could walk, explore, and eat and drink ad libitum. Protocol Downloaded from http://hyper.ahajournals.org/ by guest on April 29, 2017 All recordings were performed during the daytime. The arterial catheter was connected to a Statham P23Dc pressure transducer (Oxnard, CA, USA) for arterial pressure recording; the venous catheter was connected to a long extension so that drug administration could be performed out of the animal's sight. Care was taken to keep the room noiseless and to maintain a low degree of illumination. For the assessment of BP and heart rate variability, the pressor trace was chart-displayed on a Grass polygraph (Quincy, MA, USA) and recorded on a Racal Store 4 tape recorder (Southampton, Hampshire, England) for subsequent analysis. A continuous recording lasting at least 90 minutes was obtained under each experimental condition. After the continuous BP recording was completed, the baroreceptor control of heart rate was examined. To this aim, the pressor trace was ink-written at a paper speed of 2.5 mm/sec and simultaneously derived to trigger a tachograph for beat-to-beat heart rate display. Bolus i.v. injections of phenylephrine and nitroprusside (1—4 /ig/kg for both drugs) were administered respectively to stimulate and to deactivate arterial baroreceptors, thus eliciting reflex heart rate changes. Two to three boluses of each drug were given in a random order. Both the study of BP and heart rate variability and the baroreceptor reflex study were performed under control conditions and during 1) cholinergic blockade by atropine sulfate, 0.75 mg/kg i.v. (n = 11); 2) £adrenergic blockade by propranolol, 1 mg/kg i.v. (n = 10); and 3) combined blockade by propranolol plus atropine (n = 10). The effectiveness of autonomic blockades was checked immediately after the atropine or propranolol injection and every 30 minutes thereafter. /3-Adrenergic blockade was considered effective if an i.v. injection of isoproterenol, 0.2 Atg/kg, caused no tachycardic response. Cholinergic blockade was considered effective if the small, residual bradycardic response to phenylephrine injection that was observed immediately after atropine injection showed no recovery. Supplemental doses of either blocking agent were given as needed. The experimental session under control conditions was the initial one in each rat. The session employing either atropine or propranolol was then performed and VOL 10, No 5, NOVEMBER 1987 was followed by the session using combined blockade. Finally, after a 24-hour drug washout interval, the session in which a single drug was omitted (atropine or propranolol) was performed. Only four rats went through all four experimental sessions, however. Of the remaining rats, seven underwent the study with a single drug and six were additionally given combined blockade. Data Analysis To measure BP and heart rate variability, each 90minute BP recording was analyzed beat-to-beat by a PDP11 computer (Digital Equipment, Maynard, MA, USA) that scanned the trace every 60 msec and calculated 1) the mean values of heart rate and systolic, diastolic, and mean arterial pressures for each 10-minute period during the 90-minute cycle, 2) the corresponding variation coefficients (i.e., the standard deviation divided by the mean multiplied by 100), and 3) the average of the nine 10-minute values to obtain a single measure for each variable examined. Baroreceptor control of heart rate was analyzed by calculating the ratio of the peak change in pulse interval to the peak change in mean arterial pressure induced by the vasoactive drug. In each rat, the ratios obtained by the various injections of phenylephrine were averaged. The same procedure was adopted for the nitroprusside injections. The statistical comparison of control and drug treatment conditions was performed by the nonparametric Wilcoxon rank sum test (variability data) and the paired t test (all other data). Because more than one comparison was made for the same group of animals (control vs 3 types of autonomic blockade), the/j level of statistical significance was set below 0.01. Results As shown in Table 1, under control conditions mean arterial pressure and heart rate were similar in the three groups. Autonomic interventions did not significantly alter BP, whereas they induced the expected heart rate changes; namely, a slight bradycardia and a more pronounced tachycardia accompanying, respectively, propranolol and atropine administration. During combined blockade a modest but significant tachycardia was observed. After administration of all autonomic blocking drugs, the behavior of the animal (physical activity, grooming, eating, drinking, exploring patterns) showed no apparent variations from that observed during control conditions. Effects of Autonomic Blockade on BP and Heart Rate Variabilities As shown in Figure 1, following atropine administration heart rate increased markedly and became less variable, whereas BP oscillations were markedly enhanced. This response was apparent in 10 of the 11 animals studied, and the results were significant for the group as a whole (Figure 2). The average reduction in heart rate variability induced by atropine was 30 ± 7%, and the corresponding average increase in BP variability was 40 ± 8%. BP VARIABILITY AND BARORECEPTOR REFLEXES IN RATS/Ferrari et al. 535 TABLE 1. Average Values of Mean Arterial Pressure and Heart Rate Under Control Conditions and During Treatment with Autonomic Blocking Drugs Atropine + Propranolol Propranolol Control Control Variable (n=10) (71=10) (71=10) (n=10) MAP (mm Hg) 105 ± 3 101 ±2 100±3 100 + 2 106±5 106 + 3 38O±8 334 + 7 417 + 3* HR (beats/min) 361 ±6 355 + 2 379 + 5* Entries are means ± SE of the data obtained in single animals by computer analysis of a 90-minute continuous BP recording under each experimental condition. MAP = mean arterial pressure; HR = heart rate. *p<0.01, compared with control values. Control Atropine Downloaded from http://hyper.ahajournals.org/ by guest on April 29, 2017 The results obtained after propranolol administration are shown in Figure 3. Propranolol reduced heart rate variability in nine of the 10 animals studied, and the average change (— 23 ± 4%) was significant for the group as a whole. However, the reduction in heart rate variability was not accompanied by a significant change in BP variability. The results of combined autonomic blockade are shown in Figure 4. The effects of this intervention closely mimicked those observed after administration of atropine alone, that is, a marked reduction in heart rate variability (— 40 ± 5%) and a marked increase in BP variability (+ 33 ± 7%) occurred. Effects of Autooomlc Blockade on Baroreceptor Control of Heart Rate As shown in Figure 5 (left panels), following atropine administration thereflexincrease andreductionin pulse interval induced by phenylephrine and nitroprusside, respectively, were drastically blunted. In contrast, propranolol administration (see Figure 5, middle panels) did not affect the pulse interval response to phenylephrine, and it reduced the pulse interval response to nitroprusside to a much lesser extent than was observed after the administration of atropine. The pulse interval responses to phenylephrine and nitroprusside were almost completely abolished by combined autonomic blockade (see Figure 5, right panels). Discussion In our unrestrained rats, a 30% reduction in heart rate variability induced by cholinergic blockade was accompanied by an increase in BP variability. In contrast, a comparable reduction in heart rate variability induced by J9-adrenergic blockade was not accompanied by any changes in BP variability. Finally, combined cholinergic and /3-adrenergic blockade caused alterations in heart rate and BP variability that were superimposable on those induced by cholinergic blockade alone. These results cannot be explained by behavioral differences induced by the central effects of atropine or propranolol because no drug-related behavioral changes were observed. Thus, they indicate that in the unrestrained condition 1) cardiac neural drive is responsible for a substantial fraction of spontaneous heart rate variability, 2) the oscillatory role is played by both the vagi and the sympathetic cardiac nerves, and 3) only the vagally mediated heart rate oscillations subserve a BP-stabilizing effect (i.e., display a trend toward a reduction in the magnitude of the spontaneous BP oscillations that characterize the unrestrained state). As to the mechanisms underlying these results, a plausible hypothesis is that the vagally mediated oscillations in heart rate are triggered by the arterial baroreceptors, reflecting the ability of this reflex system to buffer BP changes through opposite changes in cardiac I ATROPINE 0.75mg/Kg 200 mm ABP Hg 0 500 HR L 15sec 250 FIGURE 1. Original recording showing the effects of atropine administration on arterial blood pressure (ABP) and heart rate (HR) in an unanesthetized normotensive rat. Note the increase in ABP variability and the decrease in HR variability after injection of the drug (arrow). HYPERTENSION 536 HR VOL 10, No 5, NOVEMBER MAP p<0 .01 p c C .01 T a> 3 o a o o c o J o o Control Atropin* Control Downloaded from http://hyper.ahajournals.org/ by guest on April 29, 2017 output. This hypothesis is supported by the observation made in this and in previous studies that the vagus is primarily responsible for the bradycardia accompanying baroreceptor stimulation8 and for the tachycardia accompanying baroreceptor deactivation, with the sympathetic nervous system playing a minor role. It is also supported by the results of studies conducted in animals and humans. In animals, the increased BP variability that follows denervation of the arterial baroreceptors has been shown to be accompanied by a reduced heart rate variability.2910 Likewise, the sensitivity of the baroreceptor-heart rate control has been found to correlate positively with 24-hour heart HR MAP 6 I o Control Propranolol Control Proprsnolol * p<0.01 vs Control FIGURE 3. Modifications in the heart rate (HR) and mean arterial pressure (MAP) variation coefficients caused by propranolol-induced fi-adrenergic blockade in 10 individual rats ( ) and in the group as a whole (o o). i 1• % HR I FIGURE 2. Modifications in the heart rate (HR) and mean arterial pressure (MAP) variation coefficients caused by atropine-induced cholinergic blockade in 11 individual rats ( ) and in the group as a whole (o o). 36 ' Atroplne * p < 0 0 1 vs Control c e 73 T T r s 1987 MAP I Cont rol Y//,:i P r o p r a n o l o l + Atropine (n-10) FIGURE 4. Effects of combined autonomic blockade by propranolol plus atropine on the variation coefficients of heart rate (HR) and mean arterial pressure (MAP). rate variability and negatively with 24-hour BP variability."'12 Three further comments should be made. The first comment concerns the report by Buchholz and Nathan13 that administration of methylatropine to conscious rats caused a reduction in heart rate variability but no change in BP variability.13 However, BP variability was measured by analyzing a single pressure wave every 15 seconds (i.e., 1-2% of all BP waves), and intermittent sampling is known to limit precise estimation of this phenomenon.14 Furthermore, methylatropine is endowed with ganglionic blocking properties" that may blunt sympathetic influences on peripheral circulation. This blunting effect may have prevented an increased BP variability from being observed. The second aspect concerns the role of the sympathetically mediated heart rate variability in overall cardiovascular control. This question arises because the propranolol-induced reduction in heart rate oscillations did not cause any change in BP variability. As we mentioned, failure of BP variability to increase following propranolol-induced reduction in heart rate variability can be easily explained by the fact that baroreceptorreflexinfluences on the sinus node are mediated largely by the vagus. It is more difficult, however, to explain why a propranolol-induced reduction in the variability of heart rate (and probably of cardiac output) was not followed by a reduction in BP variability. One possibility is that, at variance with the sudden vagally evoked heart rate alterations, the slower-developing changes in heart rate mediated by the sympathetic system are not easily transformed into BP changes. An alternative possibility is that when the /3-adrenergic drive is removed, BP oscillations are maintained by sympathetic influences on a-adrenergic receptors. The third aspect relates to thefindingthat combined BP VARIABILITY AND BARORECEPTOR REFLEXES IN RATS/Ferrari et al. BARORECEPTOR STIMULATION 1 _ 1,5 FIGURE 5. Effects of cholinergic (left panels), fi-adrenergic (middle panels), and combined (right panels) blockade on baroreceptor control of heart rate as studied by the vasoactive drug technique. Baroreceptor reflex sensitivity was calculated as the ratio of the peak change in pulse interval (PI) to the peak change in mean arterial pressure (MAP) following baroreceptor stimulation by phenylephrine administration (upperpanels) or baroreceptor deactivation by nitroprusside administration (lower panels). I -p<0.01 , 537 BARORECEPTOR DEACTIVATION .- p<0.01-< -p<0.01 - < 1.0 Downloaded from http://hyper.ahajournals.org/ by guest on April 29, 2017 u u • • oa ZZ2 Control CD Atropin* (»:11) ropr.nolol (n = 10> n* (n-.IO) cholinergic and /3-adrenergic blockade of the heart, although more effective than selective blockade of either autonomic division, reduced spontaneous heart rate variability by only slightly more than 40%. Because the effectiveness of total autonomic cardiac blockade was well established (see Materials and Methods), this finding indicates that in the rat more than 50% of this phenomenon is unrelated to neural modulation, at least as far as the traditional autonomic pathways are concerned. The factors involved in this residual heart rate variability are unknown, although various humoral and physical mechanisms' 6 can be regarded as possible candidates. Our propranolol data, however, allow us to exclude the possibility that, among the humoral factors, circulating catecholamines play a role. 4. 5. 6. 7. 8. 9. 10. Acknowledgments Tbe authors gratefully acknowledge the contributions of Dr. Carla Zanchetti (illustrations), Mr. Riccardi Sarri (photography), and Mrs. Paola Boccaccini (manuscript typing). References 1. Anderson DE, Yingling JE, Sagawa K. Minute-to-minute covariations in cardiovascular activity in conscious dogs. Am J Physiol 1979;236:H434-H439 2. Ramirez J, Bertinieri G, Belli G, et al. Reflex control of blood pressure and heart rate by arterial baroreceptors and by cardiopulmonary receptors in the unanesthetized cat. J Hypertens 1985^:327-335 3. Sokolow M, Werdegar D, Kain HK, Hineman AT. Relationship between level of blood pressure measured casually and by 11. 12. 13. 14. 15. 16. portable recorders and severity of complications in essential hypertension. Circulation 1966^6:279-298 Perloff D, Sokolow M, Cowan R. The prognostic value of ambulatory blood pressure. JAMA 1983;240:2792-2798 Parati G, Pomidossi G, Albini F, Malaspina D, Mancia G. Relationship of 24 hour blood pressure mean and variability to severity of target organ damage in hypertension. J Hypertens 1987;5:93-98 Mancia G, Ferrari A, Gregorini L, et al. Blood pressure and heart rate variabilities in normotensive and hypertensive human beings. Circ Res 1983;53:96-1O4 Mancia G, Zanchetti A. Blood pressure variability. In: Zanchetti A, Tarazi RC, eds. Pathophysiology of hypertension — cardiovascular aspects. Amsterdam: Elsevier Science Publishers, 1986:125-152 (Handbook of hypertension; vol 7) Coleman TG. Arterial baroreceptor control of heart rate in the conscious rat. Am J Physiol 1980;238:H515-H520 Ito CS, Scher AM. Hypertension following arterial baroreceptor denervation in the unanesthetized dog. Circ Res 1981; 48:576-586 Buchholz RA, Hubbard JW, Nathan MA. Comparison of 1hour and 24-hour blood pressure recordings in central or peripheral baroreceptor-denervated rats. Hypertension 1986;8: 1154-1163 Conway J, Boon N, Davies C, Jerres JV, Sleight P. Neural and humoral mechanisms involved in blood pressure variability. J Hypertens 1984;2:203-208 Mancia G, Parati G, Pomidossi G, Casadei R, Di Rienzo M, Zanchetti A. Arterial baroreflcxes and blood pressure and heart rate variabilities in humans. Hypertension 1986;8:147-153 Buchholz RA, Nathan MA. Chronic lability of the arterial blood pressure produced by electrolytic lesion of the nucleus tractus solitarii in the rat. Circ Res 1984|54:227-238 Di Rienzo M, Grassi G, Pedotti A, Mancia G. Continuous vs intermittent blood pressure measurements in estimating 24hour average blood pressure. Hypertension 1983^:264-269 Fink LD, Cervoni P. Ganglionic blocking action of atropine and methylatropine. J Pharmacol Exp Ther 1953; 109:372-376 Lange G, Lee HH, Chang A, McBrooks C. Effect of stretch on the isolated cat sinoarrial node. Am J Physiol 1966;211: 1192-1196 Inverse relationship between heart rate and blood pressure variabilities in rats. A U Ferrari, A Daffonchio, F Albergati and G Mancia Downloaded from http://hyper.ahajournals.org/ by guest on April 29, 2017 Hypertension. 1987;10:533-537 doi: 10.1161/01.HYP.10.5.533 Hypertension is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1987 American Heart Association, Inc. All rights reserved. Print ISSN: 0194-911X. Online ISSN: 1524-4563 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://hyper.ahajournals.org/content/10/5/533 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Hypertension can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Hypertension is online at: http://hyper.ahajournals.org//subscriptions/